A Component-Based Approach for Securing Indoor Home Care Applications




Abstract
:1. Introduction
2. eHealthcare Application Demands
3. Distributed Applications Management Platform (DAMP)
3.1. DAMP Architecture
3.2. DAMP Services for Application Management
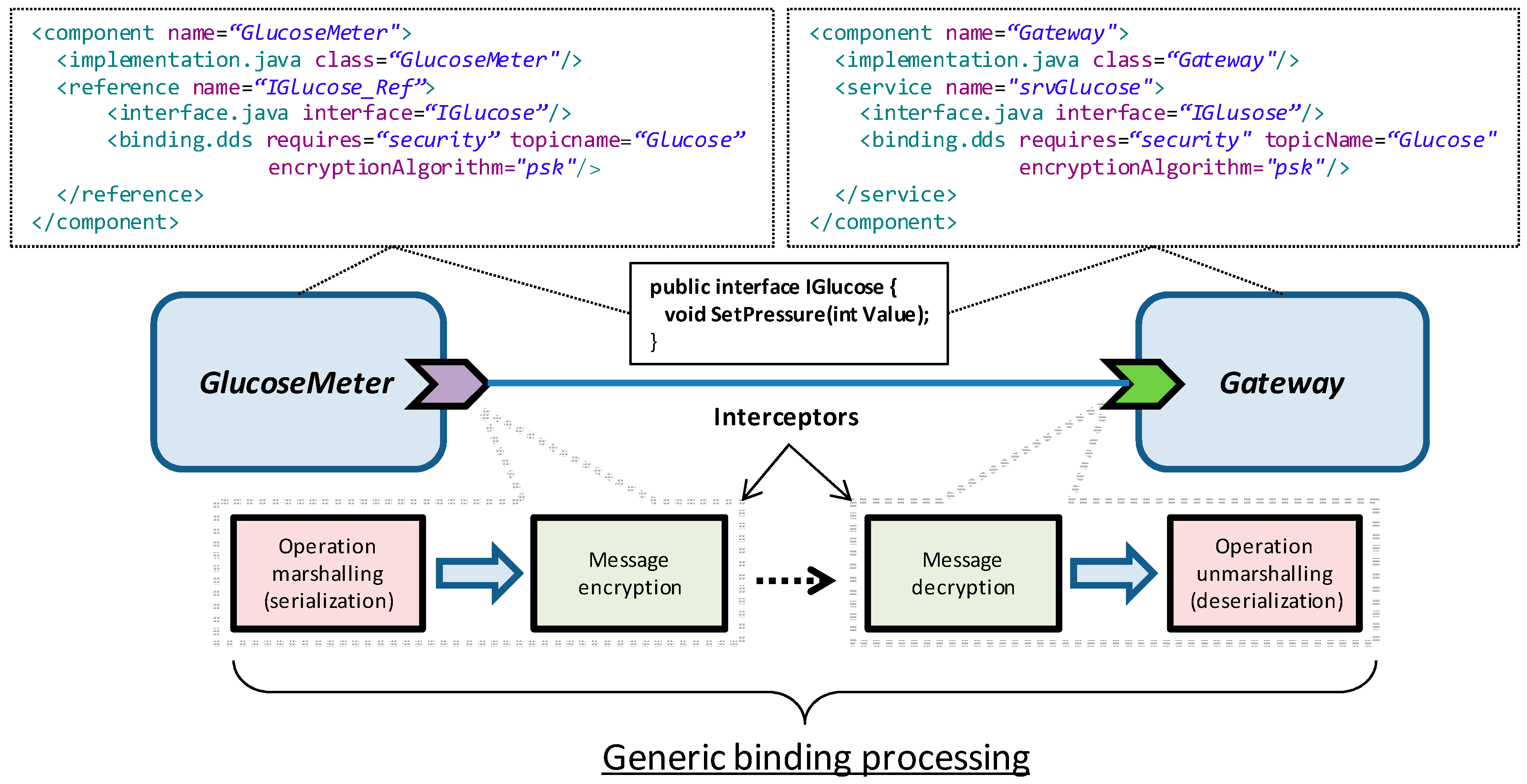
3.3. Security Considerations
3.4. Privacy and Availability of Historical Application Data
4. ehealth-Centered Design and Development
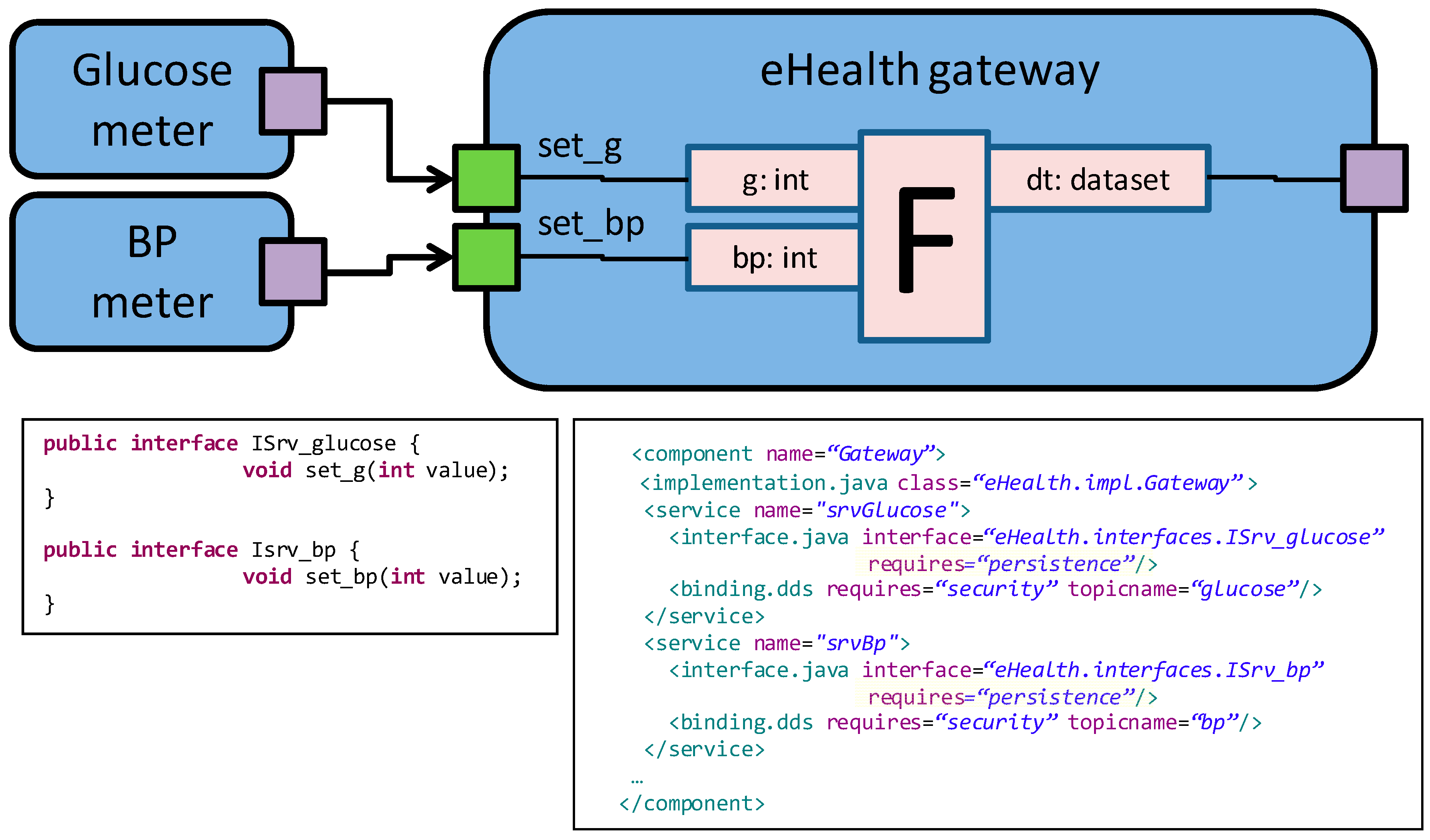
4.1. Application Specification
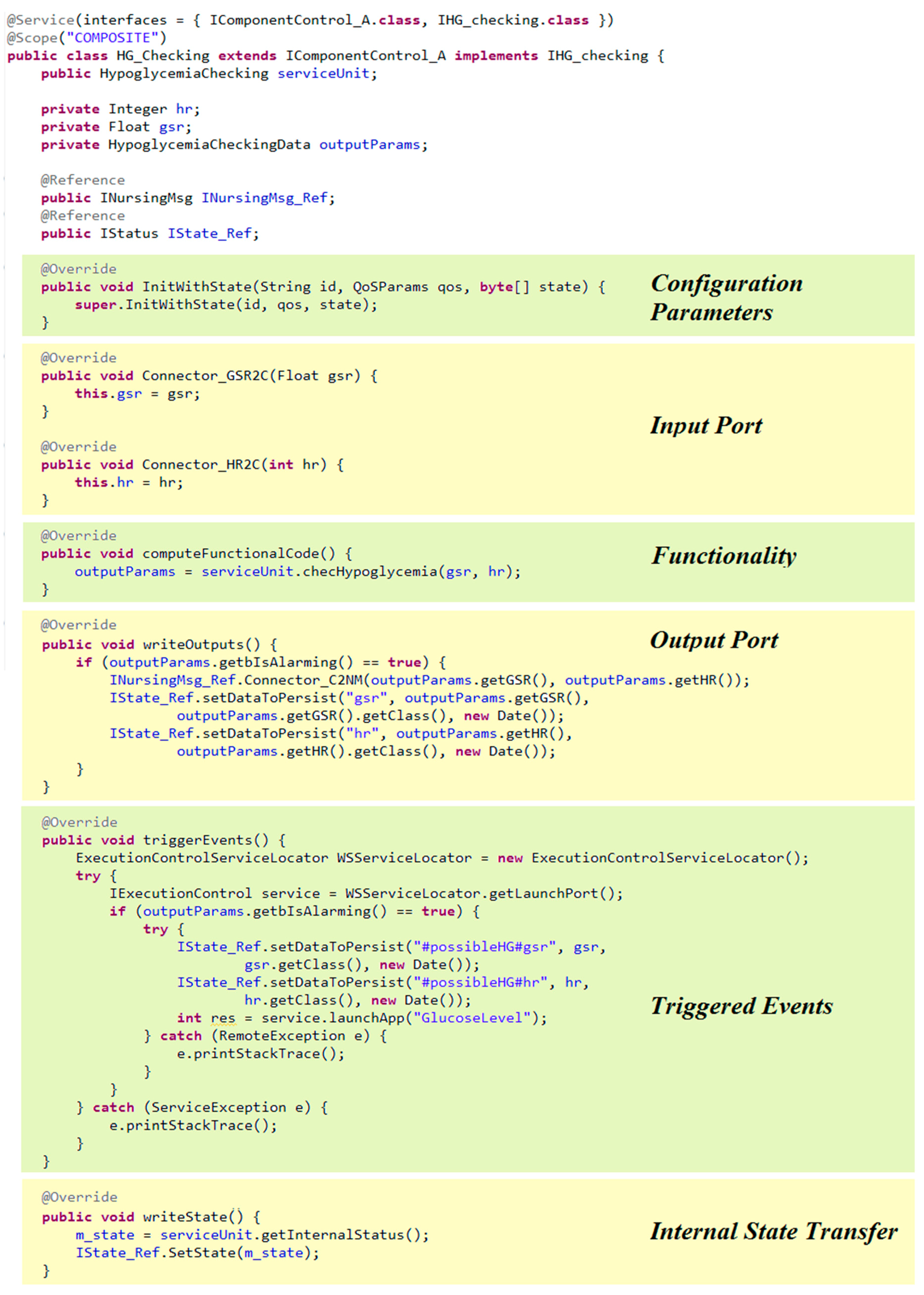
4.2. Application Development
5. Assessment
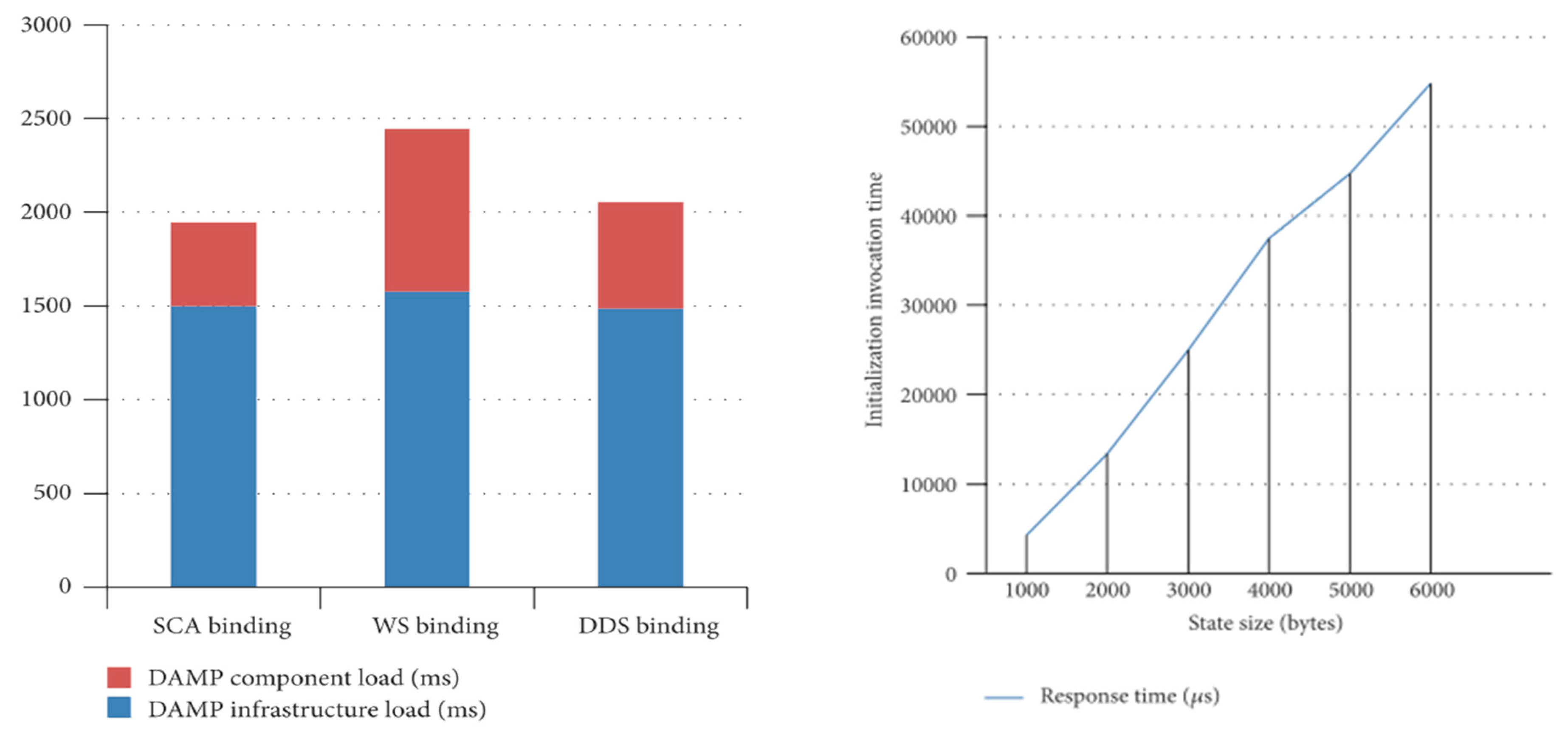
5.1. Stateful System Recovery
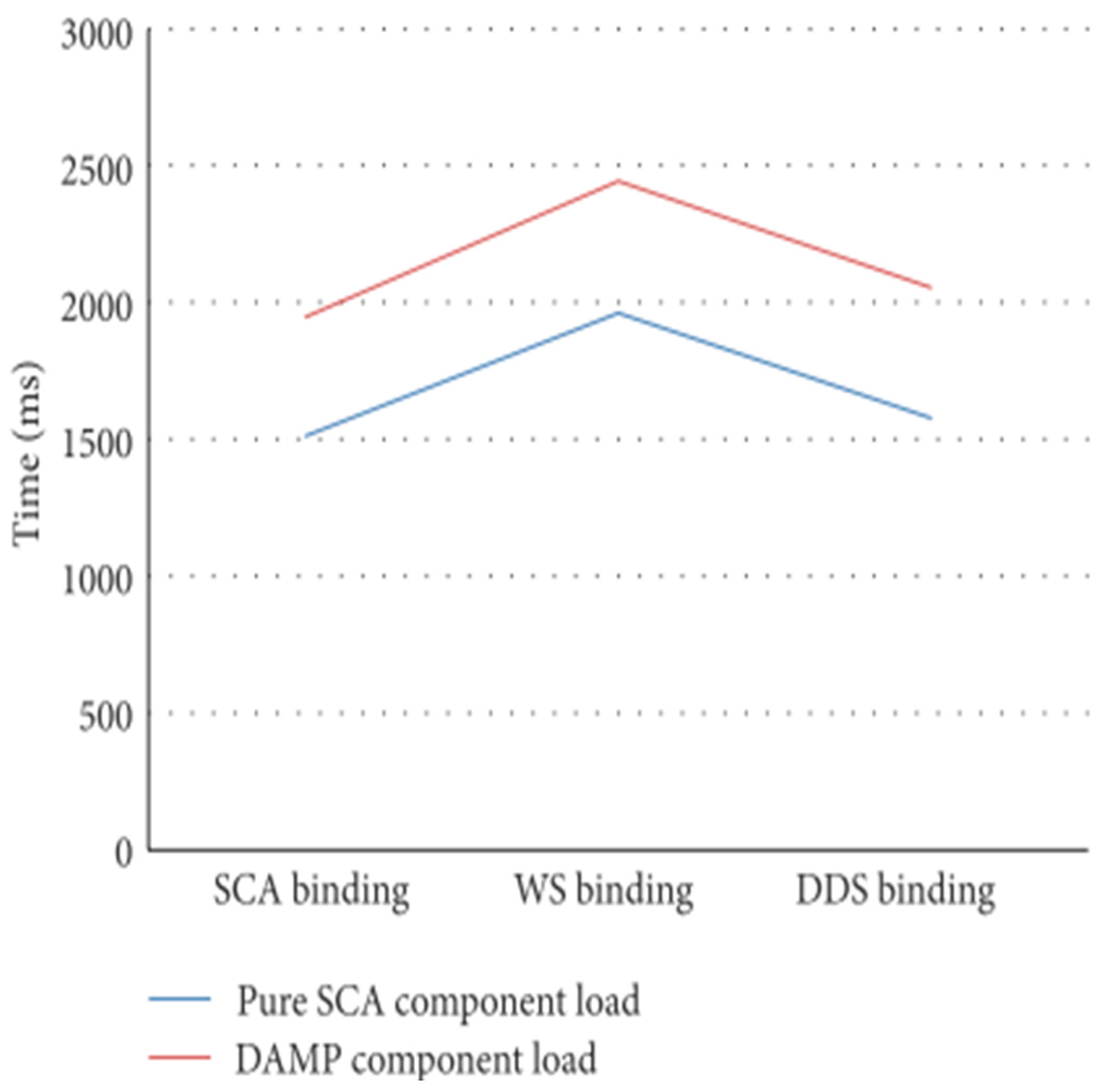
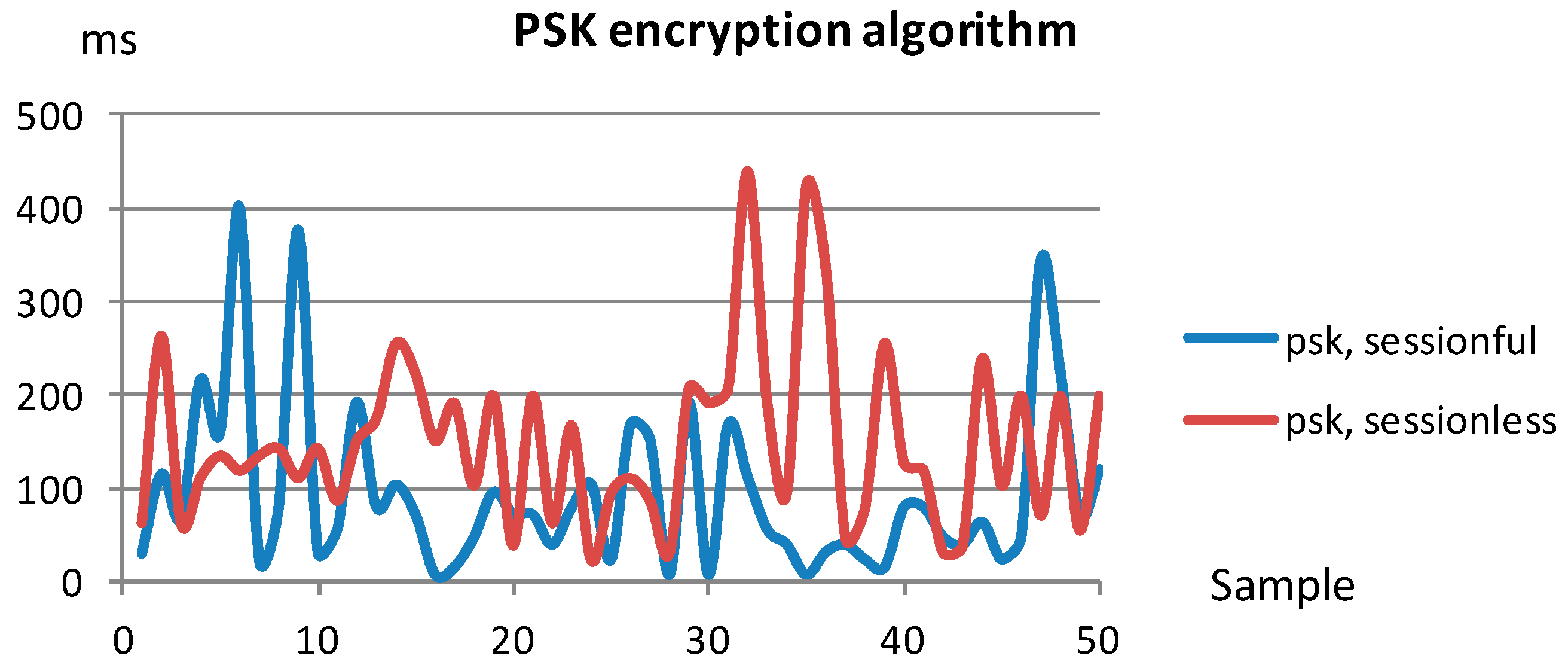
5.2. Security Binding Assesment
6. Related Work
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Leyens, L.; Hackenitz, E.; Horgan, D.; Richer, E.; Brand, A.; Bußhoff, U.; Ballensiefen, W. Csa permed: Europe’s commitment to personalised medicine. Eurohealth (Lond.) 2014, 20, 41–44. [Google Scholar]
- Building a Better Delivery System: A New Engineering/Health Care Partnership; Reid, P.P.; Compton, W.D.; Grossman, J.H.; Fanjiang, G. (Eds.) The National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Gobierno Vasco País Vasco: Transformando el Sistema de Salud; Osakidetza: Bilbao, Spain, 2012; p. 80.
- Martín-Lesende, I.; Orruño, E.; Mateos, M.; Recalde, E.; Asua, J.; Reviriego, E.; Bayón, J.C. Telemonitoring in-home complex chronic patients from primary care in routine clinical practice: Impact on healthcare resources use. Eur. J. Gen. Pract. 2017, 23, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Rani, P.; Raychoudhury, V.; Sandha, S.S.; Patel, D. Mobile health application for early disease outbreak-period detection. In Proceedings of the 2014 IEEE 16th International Conference on e-Health Networking, Applications and Services (Healthcom), Natal, Brazil, 15–18 October 2014. [Google Scholar]
- Li, J.; Ray, P. Applications of E-Health for pandemic management. In Proceedings of the The 12th IEEE International Conference on e-Health Networking, Applications and Services, Lyon, France, 1–3 July 2010. [Google Scholar]
- Culotta, A. Towards detecting influenza epidemics by analyzing Twitter messages. In Proceedings of the First Workshop on Social Media Analytics—SOMA ’10, Washington, DC, USA, 25–28 July 2010. [Google Scholar]
- Barrett, M.A.; Humblet, O.; Hiatt, R.A.; Adler, N.E. Big Data and Disease Prevention: From Quantified Self to Quantified Communities. Big Data 2013, 1, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Dugas, A.F.; Hsieh, Y.-H.; Levin, S.R.; Pines, J.M.; Mareiniss, D.P.; Mohareb, A.; Gaydos, C.A.; Perl, T.M.; Rothman, R.E. Google Flu Trends: Correlation With Emergency Department Influenza Rates and Crowding Metrics. Clin. Infect. Dis. 2012, 54, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; Committee on Patient Safety and Health Information Technology. Health IT and Patient Safety: Building Safer Systems for Better Care; The National Academies Press: Washington, DC, USA, 2012; ISBN 978-0-309-22112-2. [Google Scholar]
- Agirre, A.; Parra, J.; Armentia, A.; Ghoneim, A.; Estévez, E.; Marcos, M. QoS management for dependable sensory environments. Multimed. Tools Appl. 2016, 75, 13397–13419. [Google Scholar] [CrossRef]
- Kargl, F.; Lawrence, E.; Fischer, M.; Lim, Y.Y. Security, Privacy and Legal Issues in Pervasive eHealth Monitoring Systems. In Proceedings of the 2008 7th International Conference on Mobile Business, Barcelona, Spain, 7–8 July 2008. [Google Scholar]
- Lake, D.; Milito, R.; Morrow, M.; Vargheese, R. Internet of Things: Architectural Framework for eHealth Security. J. ICT Stand. 2014, 1, 301–328. [Google Scholar] [CrossRef]
- Adibi, S.; Agnew, G.B. On the diversity of eHealth security systems and mechanisms. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008. [Google Scholar]
- Rodríguez, M.; Zalama, E.; González, I. Improving the interoperability in the Digital Home through the automatic generation of software adapters. RIAI Rev. Iberoam. Autom. Inform. Ind. 2016, 13, 363–369. [Google Scholar] [CrossRef]
- Agirre, A.; Parra, J.; Armentia, A.; Estévez, E.; Marcos, M. QoS Aware Middleware Support for Dynamically Reconfigurable Component Based IoT Applications. Int. J. Distrib. Sens. Netw. 2016, 2016. [Google Scholar] [CrossRef]
- Armentia, A.; Gangoiti, U.; Priego, R.; Estévez, E.; Marcos, M. Flexibility Support for Homecare Applications Based on Models and Multi-Agent Technology. Sensors 2015, 15, 31939–31964. [Google Scholar] [CrossRef] [PubMed]
- PCHAlliance Continua Design Guidelines. Available online: http://www.pchalliance.org/continua-design-guidelines (accessed on 25 December 2017).
- HL7 Messaging Standard, Version 2.6. 2007. Available online: http://www.hl7.org/implement/standards/product_brief.cfm?product_id=145 (accessed on 25 December 2017).
- Avizienis, A.; Laprie, J.C.; Randell, B.; Landwehr, C.E. Basic concepts and taxonomy of dependable and secure computing. IEEE Trans. Dependable Sec. Comput. 2004, 1, 11–33. [Google Scholar] [CrossRef]
- World Health Organization. Global Diffusion of eHealth: Making Universal Health Coverage Achievable; World Health Organization: Geneva, Switzerland, 2017; ISBN 9789241511780. [Google Scholar]
- World Health Organization (WHO). Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; Volume 978. [Google Scholar]
- Alfaro Martínez, J.J.; Mora Escudero, I.; Huguet Moreno, I.; Gonzalvo Díaz, C. Hipoglucemia. Med. Programa Form. Médica Contin. Acreditado 2012, 11, 1089–1095. [Google Scholar] [CrossRef]
- Graveling, A.J.; Frier, B.M. The risks of nocturnal hypoglycaemia in insulin-treated diabetes. Diabetes Res. Clin. Pract. 2017, 133, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Mezquita-Raya, P.; Reyes-García, R.; Moreno-Pérez, Ó.; Muñoz-Torres, M.; Merino-Torres, J.F.; Gorgojo-Martínez, J.J.; Jódar-Gimeno, E.; Escalada San Martín, J.; Gargallo-Fernández, M.; Soto-Gonzalez, A.; et al. Position statement: Hypoglycemia management in patients with diabetes mellitus. Diabetes Mellitus Working Group of the Spanish Society of Endocrinology and Nutrition. Endocrinol. Nutr. (Engl. Ed.) 2013, 60, 517.e1–517.e18. [Google Scholar] [CrossRef]
- Novodvorsky, P.; Bernjak, A.; Chow, E.; Iqbal, A.; Sellors, L.; Williams, S.; Fawdry, R.A.; Parekh, B.; Jacques, R.M.; Marques, J.L.B.; et al. Diurnal Differences in Risk of Cardiac Arrhythmias During Spontaneous Hypoglycemia in Young People With Type 1 Diabetes. Diabetes Care 2017, 40, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Hervás, R.; Fontecha, J.; Ausín, D.; Castanedo, F.; Bravo, J.; López-de-Ipiña, D. Mobile monitoring and reasoning methods to prevent cardiovascular diseases. Sensors 2013, 13, 6524–6541. [Google Scholar] [CrossRef] [PubMed]
- Agirre, A.; Marcos, M.; Estevez, E. Distributed applications management platform based on Service Component Architecture. In Proceedings of the 17th IEEE International Conference on Emerging Technologies and Factory Automation (ETFA), Krakow, Poland, 17–21 September 2012. [Google Scholar]
- Laws, S.; Combellack, M.; Feng, R.; Mahbod, H.; Nash, S. Tuscany SCA in Action; Manning: Shelter Island, NY, USA, 2011. [Google Scholar]
- OASIS SCA Policy Framework Version 1.1; OASIS: Manchester, UK, 2011.
- Seinturier, L.; Merle, P.; Rouvoy, R.; Romero, D.; Schiavoni, V.; Stefani, J.-B. A component-based middleware platform for reconfigurable service-oriented architectures. Softw. Pract. Exp. 2011, 42, 559–583. [Google Scholar] [CrossRef] [Green Version]
- Agirre, A.; Perez, J.; Priego, R.; Marcos, M.; Estévez, E. SCA extensions to support safety critical distributed embedded systems. In Proceedings of the IEEE International Conference on Emerging Technologies and Factory Automation, ETFA, Cagliari, Italy, 10–13 September 2013. [Google Scholar]
- Sheldon, T. Encyclopedia of Networking & Telecommunications; McGraw-Hill, Ed.; McGraw-Hill: New York, NY, USA, 2001; ISBN 0072120053. [Google Scholar]
- IANA Transport Layer Security (TLS) Parameters. Available online: https://www.iana.org/assignments/tls-parameters/tls-parameters.xhtml (accessed on 25 December 2017).
- Szyperski, C. Component Software: Beyond Object-Oriented Programming, 2nd ed.; Addison-Wesley, Ed.; ACM Press: New York, NY, USA, 1998. [Google Scholar]
- Heineman, G.T.; Councill, W.T. Component-Based Software Engineering: Putting the Pieces Together, 1st ed.; Addison-Wesley Longman Publishing Co., Inc.: Boston, MA, USA, 2001; ISBN 0-201-70485-4. [Google Scholar]
- Papazoglou, M.P.; Traverso, P.; Dustdar, S.; Leymann, F. Service-Oriented Computing: State of the Art and Research Challenges. Computer 2007, 40, 38–45. [Google Scholar] [CrossRef]
- Erl, T. Service-Oriented Architecture (SOA): Concepts, Technology, and Design; Prentice Hall PTR: Upper Saddle River, NJ, USA, 2005; ISBN 0131858580. [Google Scholar]
- Wooldridge, M.; Jennings, N.R. Intelligent agents: Theory and practice. Knowl. Eng. Rev. 2009, 10, 115–152. [Google Scholar] [CrossRef]
- Weiss, G. Multiagent Systems: A Modern Approach to Distributed Artificial Intelligence; Weiss, G., Ed.; The MIT Press: Cambridge, MA, USA, 1999; ISBN 9780262731317. [Google Scholar]
- Cardellini, V.; Casalicchio, E.; Grassi, V.; Iannucci, S.; Presti, F.L.; Mirandola, R. MOSES: A framework for qos driven runtime adaptation of service-oriented systems. IEEE Trans. Softw. Eng. 2012, 38, 1138–1159. [Google Scholar] [CrossRef]
- Bellifemine, F.; Caire, G.; Poggi, A.; Rimassa, G. JADE: A software framework for developing multi-agent applications. Lessons learned. Inf. Softw. Technol. 2008, 50, 10–21. [Google Scholar] [CrossRef]
- Bajo, J.; Fraile, J.A.; Pérez-Lancho, B.; Corchado, J.M. The THOMAS architecture in Home Care scenarios: A case study. Expert Syst. Appl. 2010, 37, 3986–3999. [Google Scholar] [CrossRef]
- Büsching, F.; Bottazzi, M.; Wolf, L. The GAL monitoring concept for distributed AAL platforms. In Proceedings of the IEEE 14th International Conference on e-Health Networking, Applications and Services, Beijing, China, 10–13 October 2012. [Google Scholar]
- Lamprinakos, G.C.; Asanin, S.; Broden, T.; Prestileo, A.; Fursse, J.; Papadopoulos, K.A.; Kaklamani, D.I.; Venieris, I.S. An integrated remote monitoring platform towards Telehealth and Telecare services interoperability. Inf. Sci. (N. Y.) 2015, 308, 23–37. [Google Scholar] [CrossRef]
- Hnetynka, P.; Murphy, L.; Murphy, J. Comparing the service component architecture and fractal component model. Comput. J. 2011, 54, 1026–1037. [Google Scholar] [CrossRef]
- The OSGi Alliance, Version 4.3. Available online: https://www.osgi.org/release-4-version-4-3/ (accessed on 25 December 2017).
- Malohlava, M.; Hnetynka, P.; Bures, T. SOFA 2 Component Framework and Its Ecosystem. Electron. Notes Theor. Comput. Sci. 2013, 295, 101–106. [Google Scholar] [CrossRef]
- Farella, E.; Falavigna, M.; Ricc, B. Aware and smart environments: The Casattenta project. Microelectron. J. 2010, 41, 697–702. [Google Scholar] [CrossRef]
- Søberg, J.; Goebel, V.; Plagemann, T. CommonSens: Personalisation of complex event processing in automated homecare. In Proceedings of the 6th International Conference on Intelligent Sensors, Sensor Networks and Information Processing, Brisbane, Australia, 7–10 December 2010. [Google Scholar]
- Rocha, A.; Martins, A.; Freire, J.C.; Kamel Boulos, M.N.; Vicente, M.E.; Feld, R.; van de Ven, P.; Nelson, J.; Bourke, A.; ÓLaighin, G.; et al. Innovations in health care services: The CAALYX system. Int. J. Med. Inform. 2013, 82, e307–e320. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.; Dowdall, A.; Lines, L.; Hone, K. Multimodal and ubiquitous computing systems: Supporting independent-living older users. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Stav, E.; Walderhaug, S.; Mikalsen, M.; Hanke, S.; Benc, I. Development and evaluation of SOA-based AAL services in real-life environments: A case study and lessons learned. Int. J. Med. Inform. 2013, 82, e269–e293. [Google Scholar] [CrossRef] [PubMed]
- García-Valls, M.; Rodríguez-López, I.; Fernández-Villar, L. iLAND: An Enhanced Middleware for Real-Time Reconfiguration of Service Oriented Distributed Real-Time Systems. IEEE Trans. Ind. Inform. 2013, 9, 228–236. [Google Scholar] [CrossRef]
- Gui, N.; De Florio, V.; Sun, H.; Blondia, C. Toward architecture-based context-aware deployment and adaptation. J. Syst. Softw. 2011, 84, 185–197. [Google Scholar] [CrossRef]
- Wegdam, M.; Almeida, J.P.A.; van Sinderen, M.J.; Nieuwenhuis, L.J.M. Dynamic Reconfiguration for Middleware-Based Applications; University of Twente, Centre for Telematics and Information Technology (CTIT): Enschede, The Netherlands, 2003. [Google Scholar]
- Hofmeister, C.R. Dynamic Reconfiguration of Distributed Applications. Doctoral Dissertation, University of Maryland, College Park, MD, USA, 1998. [Google Scholar]
- Léger, M.; Ledoux, T.; Coupaye, T. Reliable Dynamic Reconfigurations in a Reflective Component Model. In Proceedings of the 13th International Conference on Component-Based Software Engineering, Prague, Czech Republic, 23–25 June 2010. [Google Scholar]
- Hassine, J. Describing and assessing availability requirements in the early stages of system development. Softw. Syst. Model. 2015, 14, 1455–1479. [Google Scholar] [CrossRef]
- Gharzouli, M.; Boufaida, M. A generic P2P collaborative strategy for discovering and composing semantic web services. In Proceedings of the 4th International Conference on Internet and Web Applications and Services, Venice/Mestre, Italy, 24–28 May 2009; pp. 449–454. [Google Scholar]
- Hallsteinsen, S.; Geihs, K.; Paspallis, N.; Eliassen, F.; Horn, G.; Lorenzo, J.; Mamelli, A.; Papadopoulos, G.A. A development framework and methodology for self-adapting applications in ubiquitous computing environments. J. Syst. Softw. 2012, 85, 2840–2859. [Google Scholar] [CrossRef]
- García-Magariño, I.; Palacios-Navarro, G. A model-driven approach for constructing ambient assisted-living multi-agent systems customized for Parkinson patients. J. Syst. Softw. 2016, 111, 34–48. [Google Scholar] [CrossRef]
- Cervantes, H.; Hall, R.S. A Framework for Constructing Adaptive Component-Based Applications: Concepts and Experiences. In Proceedings of the 7th International Symposium Component-Based Software Engineering (CBSE), Edinburgh, UK, 24–25 May 2004; Springer: Berlin/Heidelberg, Germany, 2004; pp. 130–137. [Google Scholar]
- Noguero, A.; Calvo, I.; Pérez, F.; Almeida, L. FTT-MA: A flexible time-triggered middleware architecture for time sensitive, resource-aware AmI systems. Sensors 2013, 13, 6229–6253. [Google Scholar] [CrossRef] [PubMed]
- Li, W. QoS assurance for dynamic reconfiguration of component-based software systems. IEEE Trans. Softw. Eng. 2012, 38, 658–676. [Google Scholar] [CrossRef]
- Kramer, J.; Magee, J. The evolving philosophers problem: Dynamic change management. IEEE Trans. Softw. Eng. 1990, 16, 1293–1306. [Google Scholar] [CrossRef] [Green Version]
- Vandewoude, Y. Dynamically Updating Component-Oriented Systems; Faculty of Engineering, K.U. Leuven: Leuven, Belgium, 2007. [Google Scholar]
- OASIS Service Component Architecture (SCA). Available online: http://www.oasis-opencsa.org/sca (accessed on 25 December 2017).
- IEC IEC 61784-3-3: Indutrial Communication Networks—Profiles—Part 3–3: Functional Safety Fieldbuses—Additional Specifications for CFP 3. Available online: https://webstore.iec.ch/publication/25404 (accessed on 25 December 2017).
- Bai, Y.; Dai, L.; Li, J. Issues and Challenges in Securing eHealth Systems. Int. J. E-Health Med. Commun. 2014, 5, 1–19. [Google Scholar] [CrossRef]
- Rashidi, P.; Mihailidis, A. A survey on ambient-assisted living tools for older adults. IEEE J. Biomed. Health Inform. 2013, 17, 579–590. [Google Scholar] [CrossRef]
- Kumar, P.; Lee, S.-G.; Lee, H.-J. E-SAP: Efficient-strong authentication protocol for healthcare applications using wireless medical sensor networks. Sensors 2012, 12, 1625–1647. [Google Scholar] [CrossRef] [PubMed]
- Becker, M. Software Architecture Trends and Promising Technology for Ambient Assisted Living Systems. In Dagstuhl Seminar Proceedings-Assisted Living Systems-Models, Architectures and Engineering Approaches; Schloss Dagstuhl—Leibniz-Zentrum fuer Informatik, Germany: Dagstuhl, Germany, 2008; Volume 7462. [Google Scholar]
- Yilmaz, T.; Foster, R.; Hao, Y. Detecting vital signs with wearable wireless sensors. Sensors 2010, 10, 10837–10862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theoharidou, M.; Tsalis, N.; Gritzalis, D. Smart Home Solutions: Privacy Issues. In Handbook of Smart Homes, Health Care and Well-Being; Springer International Publishing: Cham, Switzerland, 2014; pp. 1–14. ISBN 9783319015835. [Google Scholar]
- Lee, M.; Gatton, T.M. Wireless health data exchange for home healthcare monitoring systems. Sensors 2010, 10, 3243–3260. [Google Scholar] [CrossRef] [PubMed]
- Abdmeziem, M.R.; Tandjaoui, D. An end-to-end secure key management protocol for e-health applications. Comput. Electr. Eng. 2015, 44, 184–197. [Google Scholar] [CrossRef]
- Lim, S.; Oh, T.H.; Choi, Y.B.; Lakshman, T. Security Issues on Wireless Body Area Network for Remote Healthcare Monitoring. In Proceedings of the IEEE International Conference on Sensor Networks, Ubiquitous, and Trustworthy Computing (SUTC), Hyatt Newport Beach, CA, USA, 7–9 June 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 327–332. [Google Scholar]
- Strategic Research and Innovation Agenda (SRIA v3.0); BDVA Correspondence & Registered Office: Bruxelles, Belgium, 2017.





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Requirement ID | Requirement Description |
|---|---|
| R1. Remote monitoring | Remote monitoring of physiological data. |
| R2. Health-centered monitoring | Health monitoring, alarm detection and reaction customized to the particularities of every patient. |
| R3. Remote application management | Remote deployment, upgrade and control of eHealth applications. |
| R4. Heterogeneity and interoperability | The typology of application can be diverse, in terms of implementation language, hardware platforms and operating systems. The interoperability with external systems (e.g., legacy systems) must be supported. |
| R5. Global diffusion of medical data | Support for the diffusion of digital medical data through a global network infrastructure. |
| R6. Availability | Availability of critical nodes must be ensured, to achieve adequate dependability levels. |
| R7. Reliable data transmission | Reliable communication mechanisms over inherently unsafe channels (black channels), including message integrity. |
| R8. Secure data transmission | Security of the communication channels, including sender identification, authentication and message integrity. |
| R9. Reliable and secure data persistence | Historical data persistence. The integrity and confidentiality of the database must be guaranteed. |
| Hypoglycemia Checking (HG_Checking) | ||||
|---|---|---|---|---|
| Description | Analyzes if the galvanic skin response of the patient together with its heart rate are related to a possible hypoglycemic episode. | |||
| Activation | After data reception | |||
| Availability Level | 1 | Is Stateful | Yes | |
| Required Parameters | ||||
| Name | hr | Description | Measured heart rate. | |
| Name | gsr | Description | Measure of the galvanic skin response. | |
| Provided Parameters | ||||
| Name | isAlarming | Description | Heart rate and galvanic skin response are too high for the patient. Risk of a hypoglycemic episode. | |
| Name | hr | Description | Measured heart rate. | |
| Name | gsr | Description | Measure of the galvanic skin response. | |
| Configuration Parameters | ||||
| Name | patientID | Value | 31085621 | |
| Description | Unique identifier of the patient in the eHealth system | |||
| GSR2C | |||
|---|---|---|---|
| Source | GSR_Acq | Target | HG_Checking |
| Safety | Yes | Security | No |
| Persisted | No | ||
| Connections | |||
| Output Parameter | galvanicSkinResponse | Input Parameter | gsr |
| GSR2S | |||
|---|---|---|---|
| Source | GSR_Acq | Target | GSR_Storage |
| Safety | Yes | Security | PSK Symmetric |
| Persisted | Yes | ||
| Connections | |||
| Output Parameter | galvanicSkinResponse | Input Parameter | gsrValue |
| Output Parameter | instant | Input Parameter | timeStamp |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agirre, A.; Armentia, A.; Estévez, E.; Marcos, M. A Component-Based Approach for Securing Indoor Home Care Applications. Sensors 2018, 18, 46. https://doi.org/10.3390/s18010046
Agirre A, Armentia A, Estévez E, Marcos M. A Component-Based Approach for Securing Indoor Home Care Applications. Sensors. 2018; 18(1):46. https://doi.org/10.3390/s18010046
Chicago/Turabian StyleAgirre, Aitor, Aintzane Armentia, Elisabet Estévez, and Marga Marcos. 2018. "A Component-Based Approach for Securing Indoor Home Care Applications" Sensors 18, no. 1: 46. https://doi.org/10.3390/s18010046
APA StyleAgirre, A., Armentia, A., Estévez, E., & Marcos, M. (2018). A Component-Based Approach for Securing Indoor Home Care Applications. Sensors, 18(1), 46. https://doi.org/10.3390/s18010046