
The Objective Dementia Severity Scale Based on MRI with Contrastive Learning: A Whole Brain Neuroimaging Perspective
 , and
, and
Abstract
:1. Introduction
- (1)
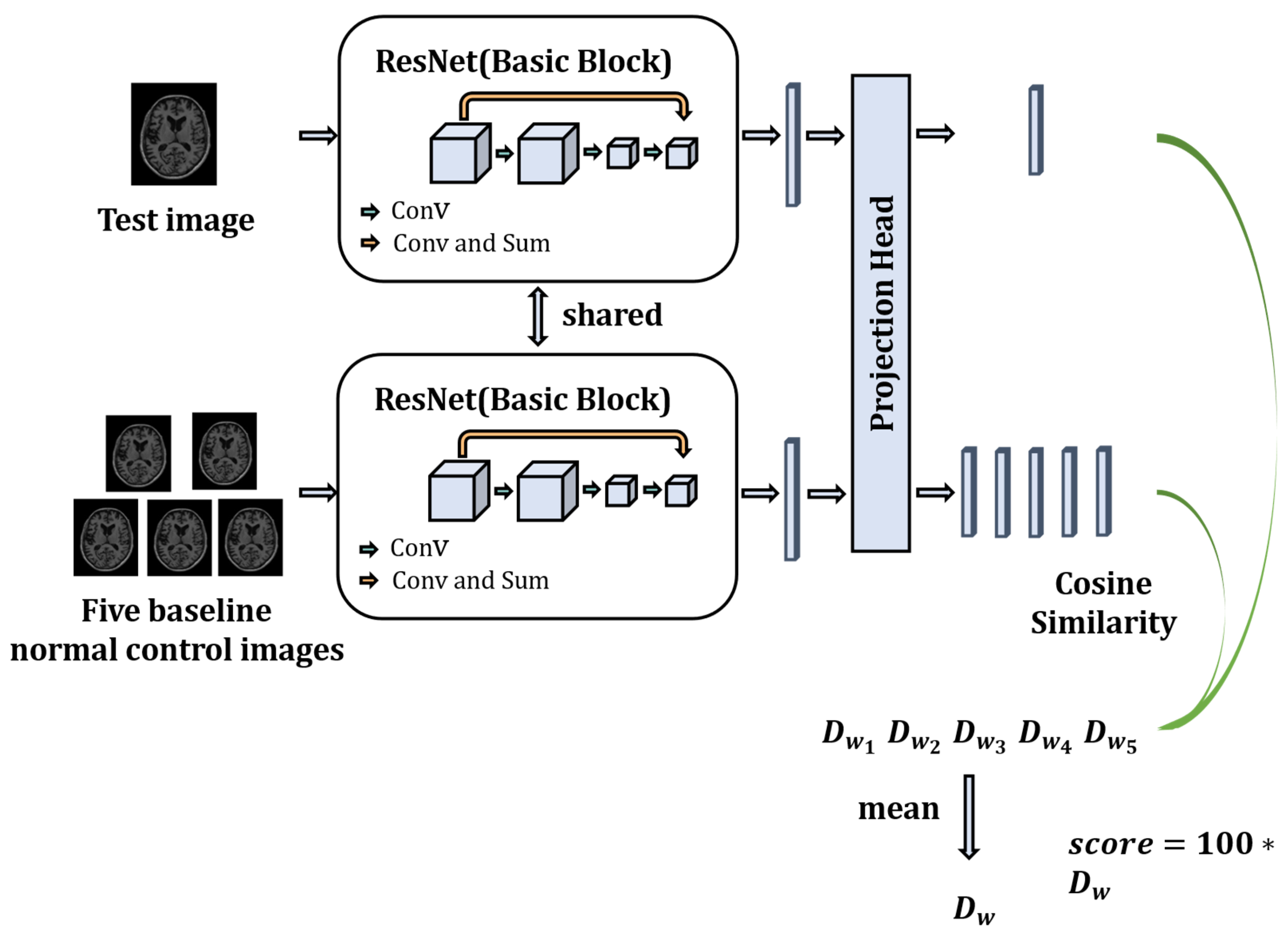
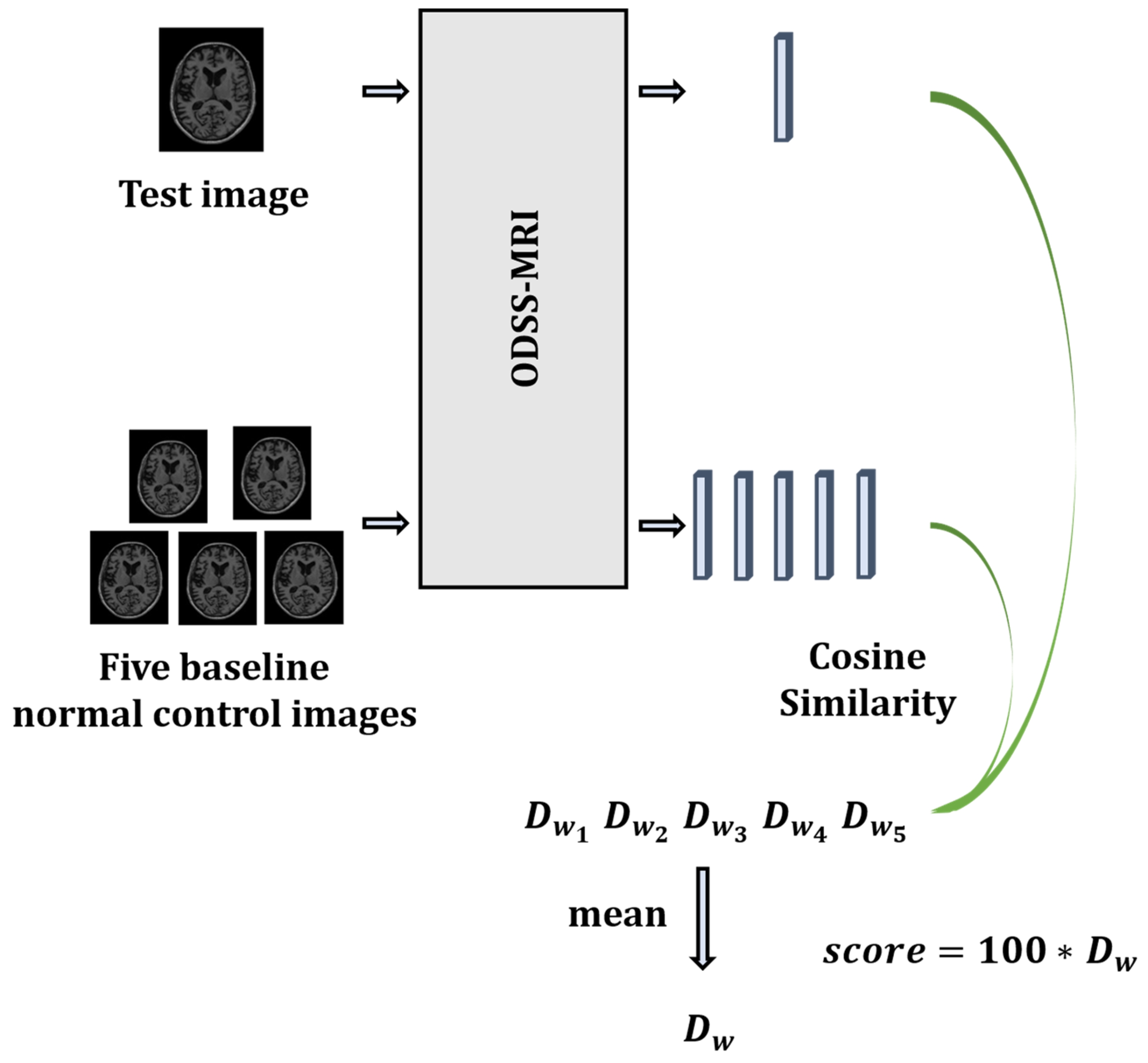
- We propose an objective dementia severity scale based on MRI (ODSS-MRI) using a contrastive learning framework to evaluate neurological function during AD progression, which is driven by the whole brain image of the patient. This effectively ensures that the evaluation score will not be affected by any possible biased subjective factors during the testing of the physician or patient.
- (2)
- The score obtained from the proposed ODSS-MRI is highly correlated with the stages of AD, indicating that ODSS-MRI can accurately describe the neurological function changes during AD progression.
- (3)
- The ODSS-MRI scores perform much better on discriminating different stages of AD progression compared to traditional psychiatric rating scales, indicating its advantage in the neurological function evaluation of AD.
2. Related Work
2.1. Evaluation of Neurological Function in Alzheimer’s Disease
2.2. Alzheimer’s Diagnosis Based on Deep Learning
2.3. Contrastive Learning
3. Materials and Methods
3.1. Materials
3.1.1. Participants
3.1.2. Data Pre-Processing
3.2. Methods
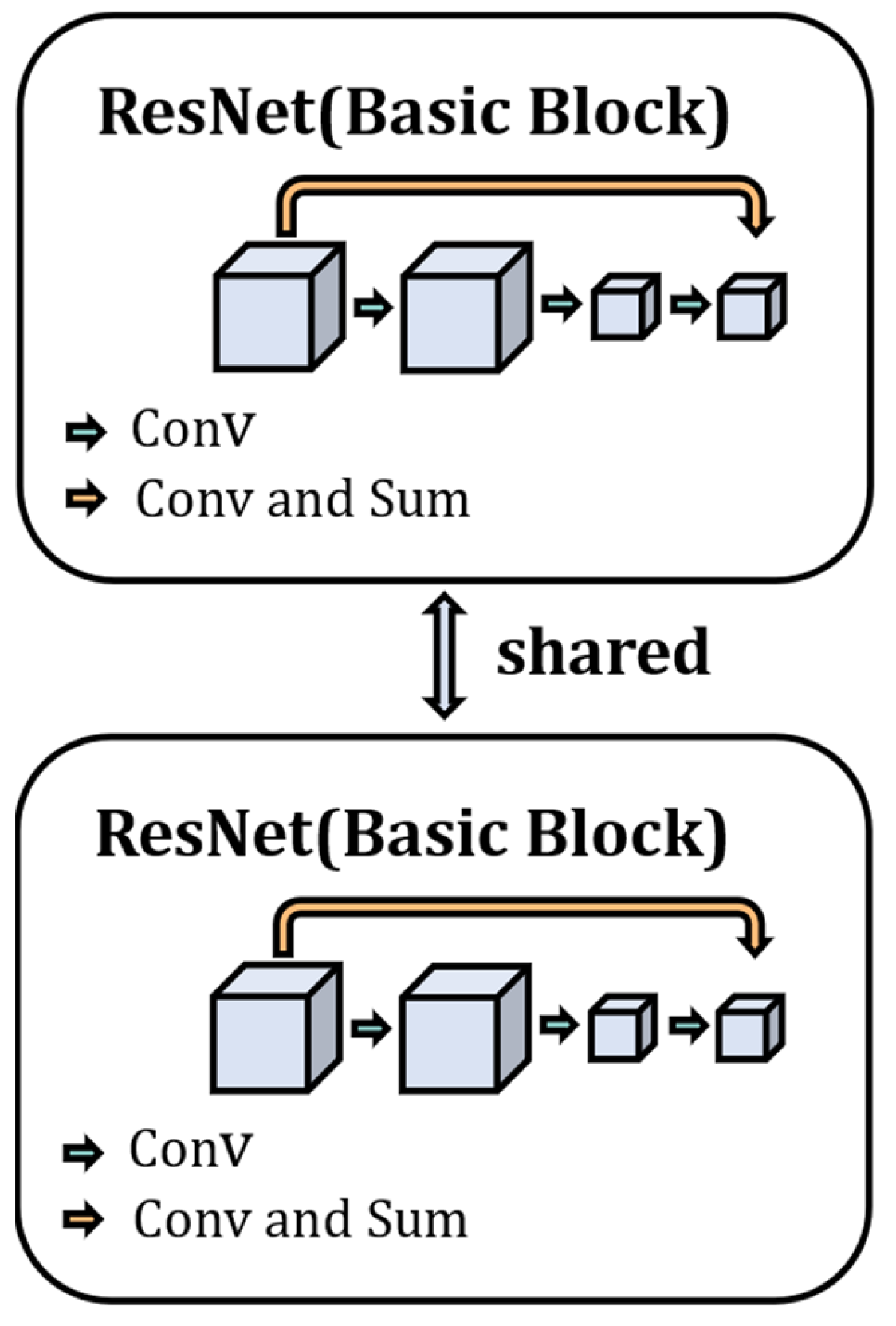
- Main structure of the model
- 2.
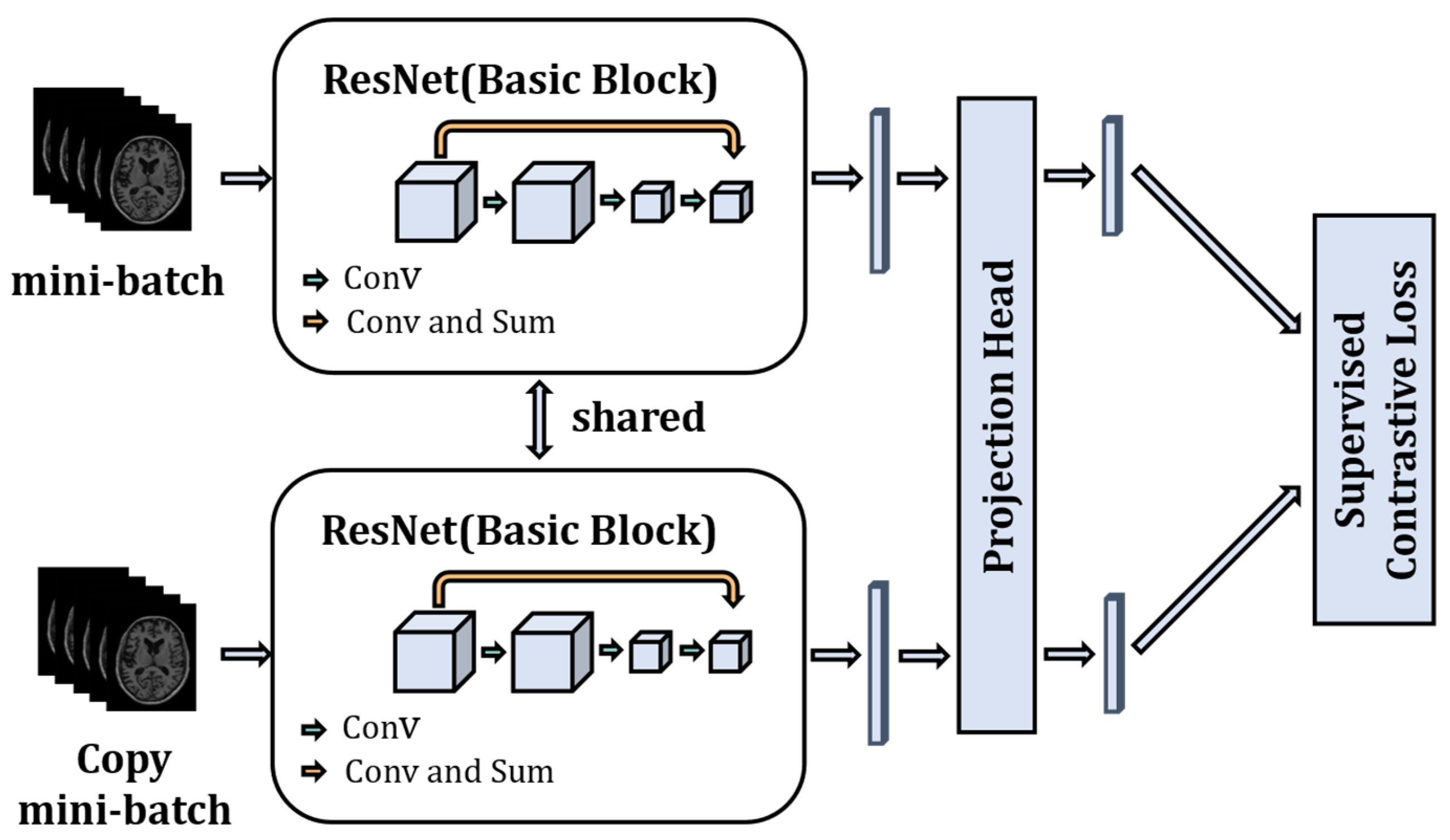
- Model Training
- 3.
- Supervised contrastive learning loss function
- 4.
- Neurological function scoring
4. Results
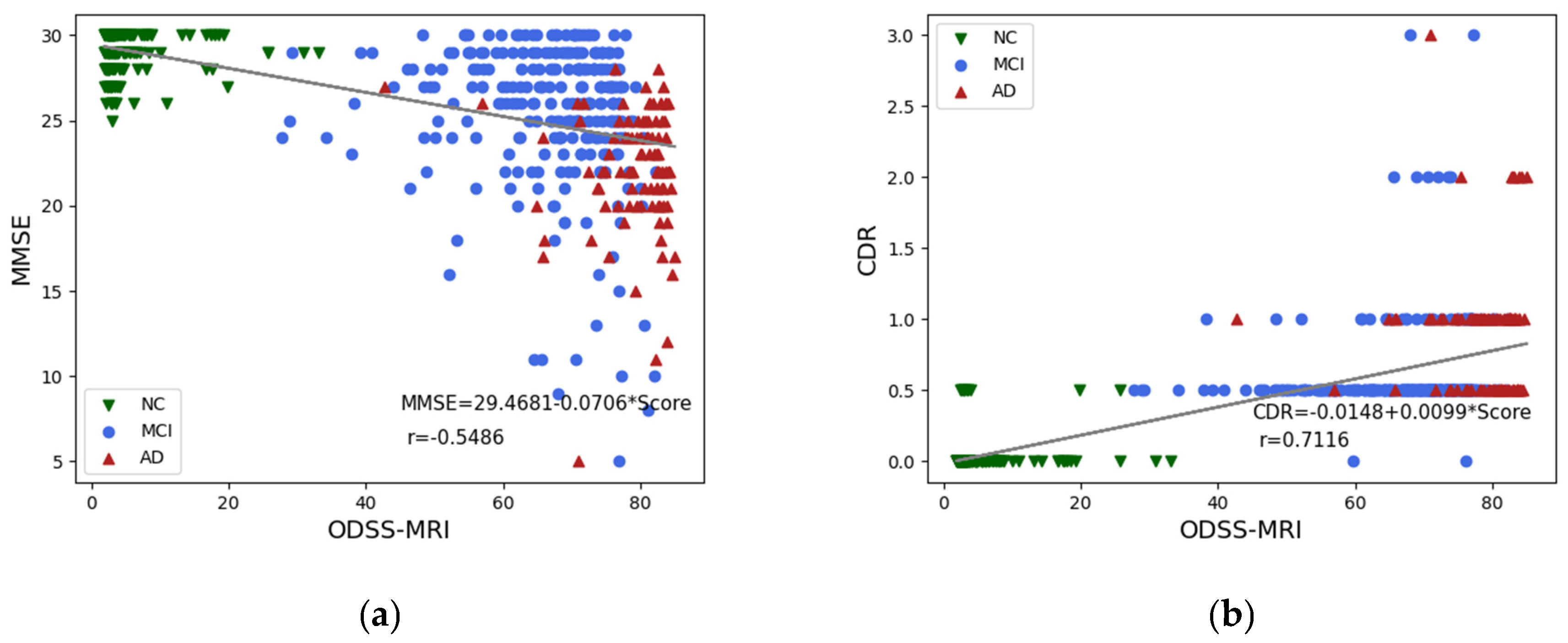
4.1. Correlation Analysis
4.2. Differential Analysis
4.3. Sensitivity, Specificity, and Accuracy
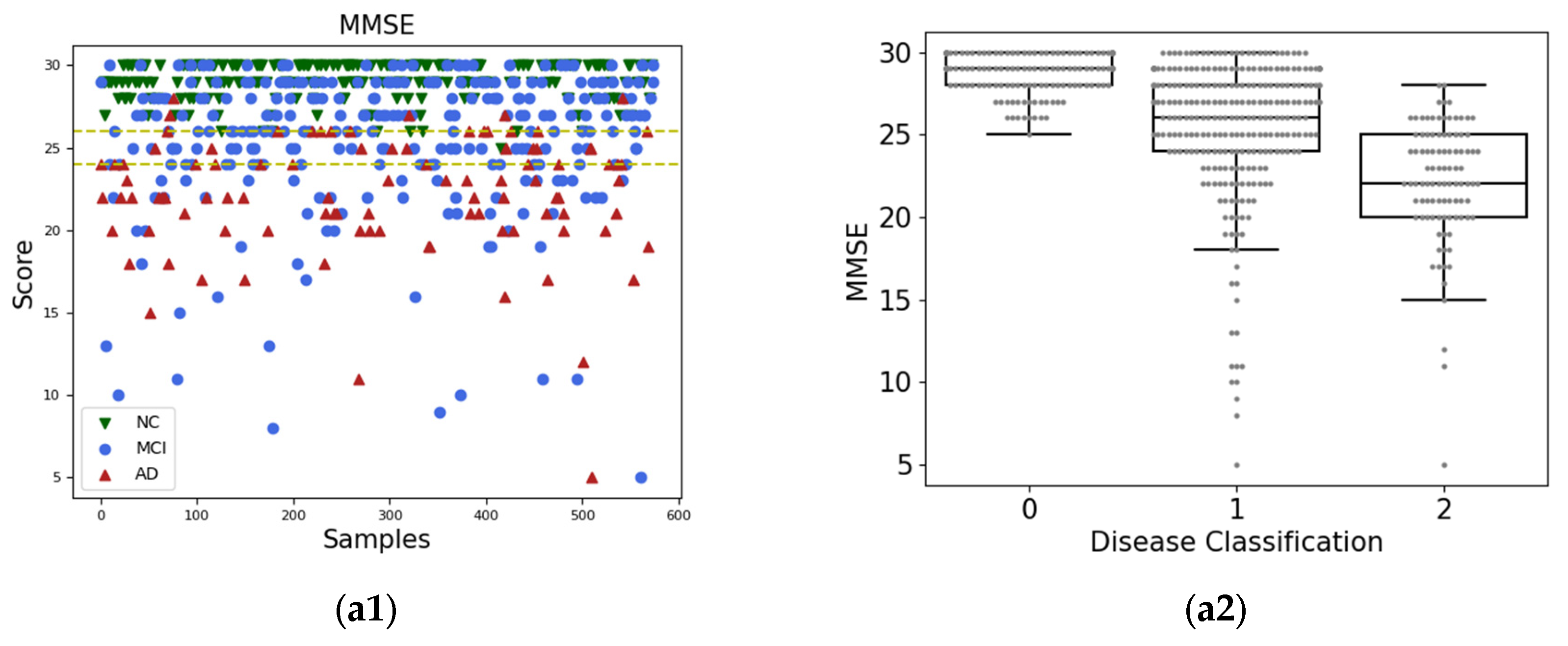
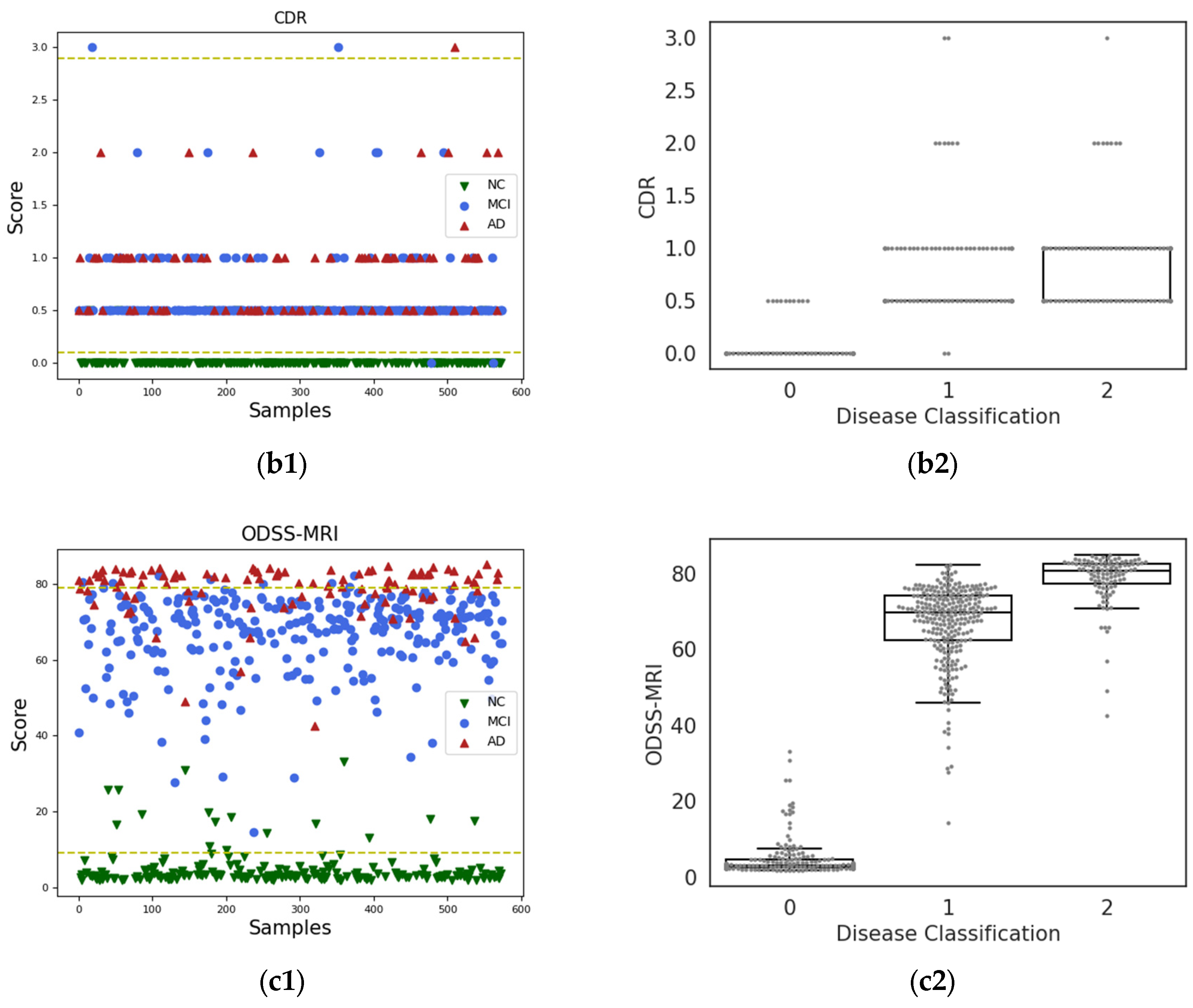
4.4. Scatter and Box-Line Plots
4.5. Statistical Information Table
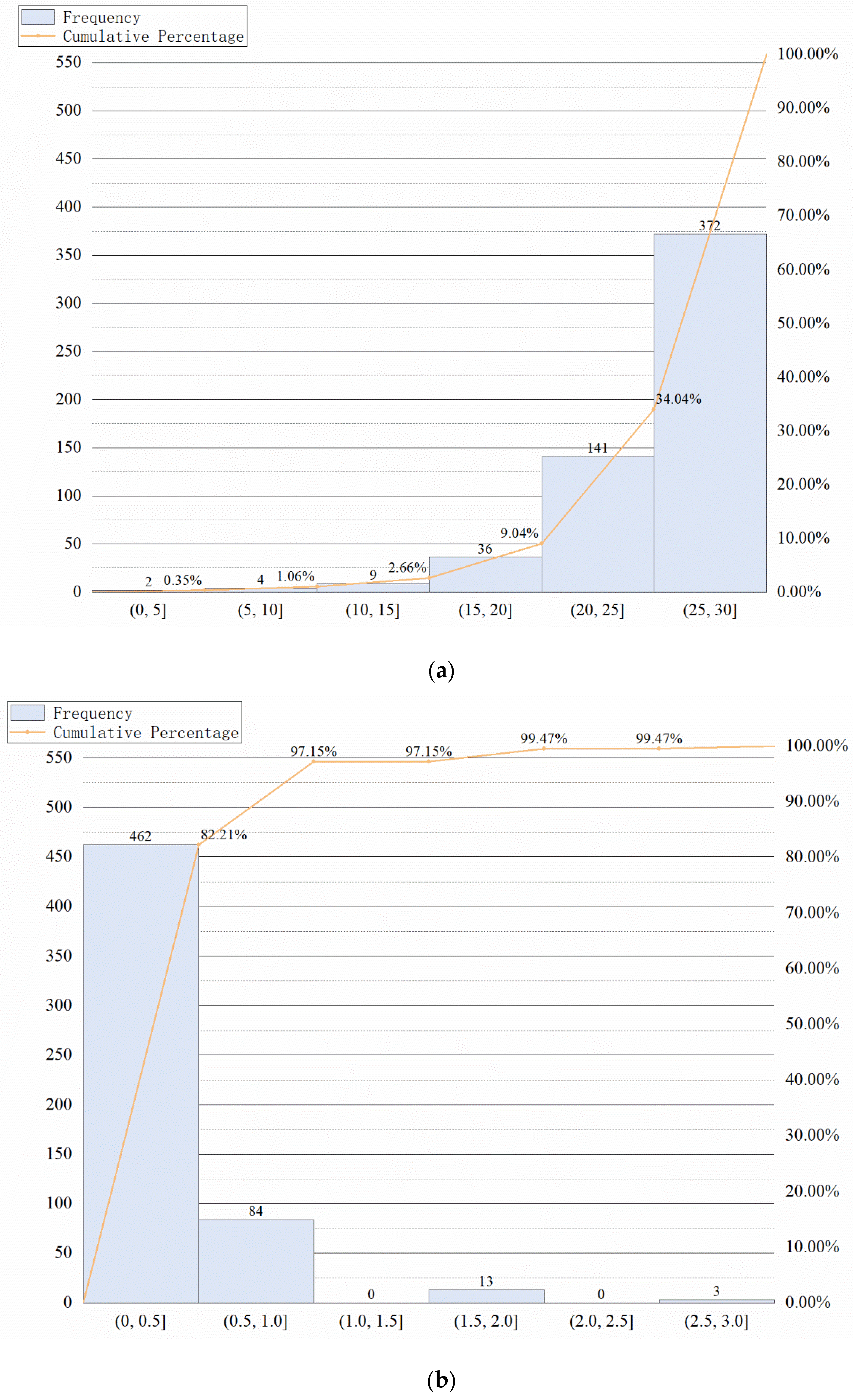
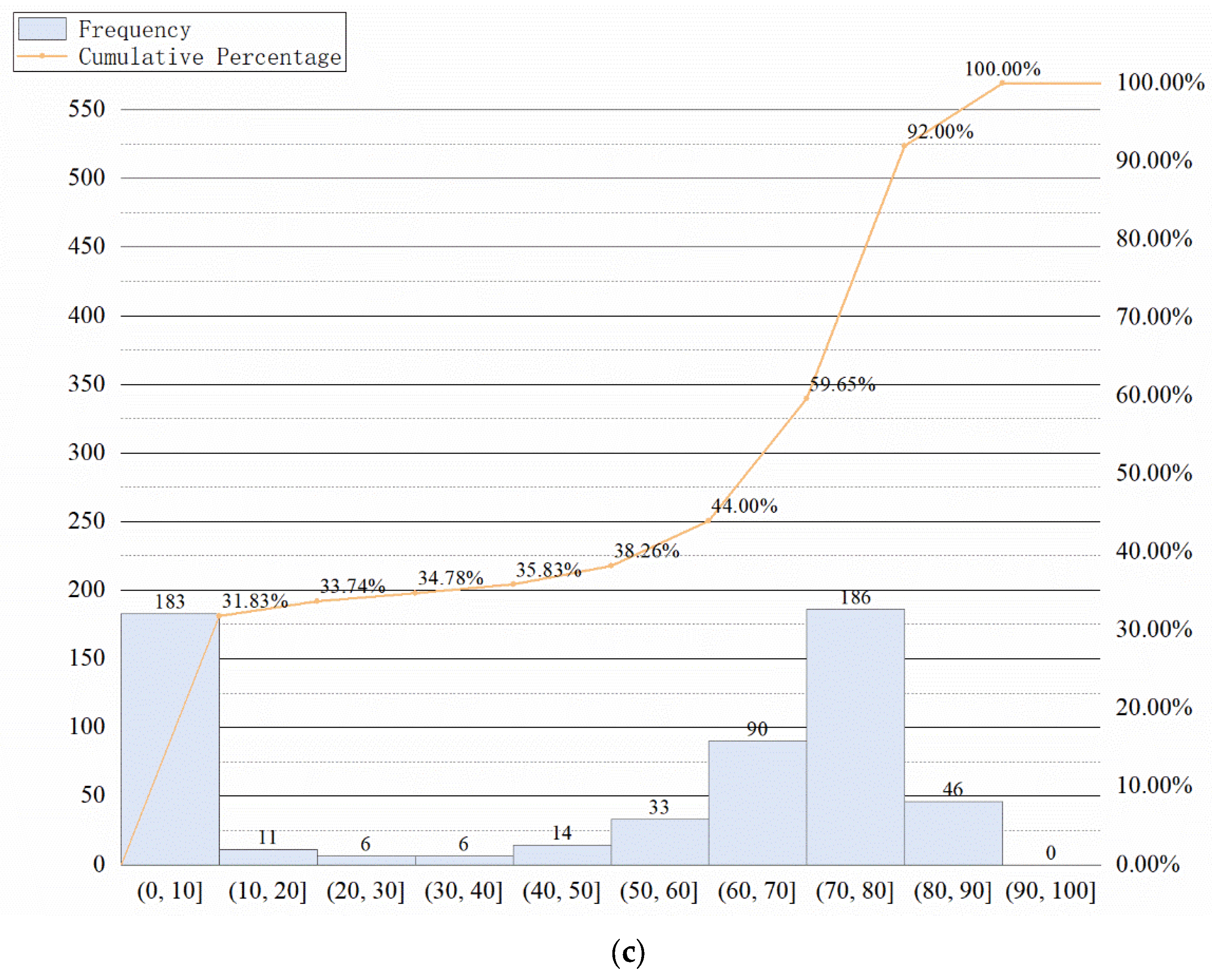
4.6. Pareto Analysis
5. Discussion and Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thies, W.; Bleiler, L. 2013 Alzheimer’s disease facts and figures. Alzheimers Dement. 2013, 9, 208–245. [Google Scholar]
- Zhou, Z.; Sodha, V.; Rahman Siddiquee, M.M.; Feng, R.; Tajbakhsh, N.; Gotway, M.B.; Liang, J. Models genesis: Generic autodidactic models for 3d medical image analysis. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2019, 22nd International Conference, Shenzhen, China, 13–17 October 2019. [Google Scholar]
- Saini, M.; Susan, S. VGGIN-Net: Deep Transfer Network for Imbalanced Breast Cancer Dataset. IEEE/ACM Trans. Comput. Biol. Bioinform. 2023, 20, 752–762. [Google Scholar] [CrossRef]
- Khader, F.; Mueller-Franzes, G.; Arasteh, S.T.; Han, T.; Haarburger, C.; Schulze-Hagen, M.; Schad, P.; Engelhardt, S.; Baebler, B.; Foersch, S. Medical Diffusion--Denoising Diffusion Probabilistic Models for 3D Medical Image Generation. arXiv 2022, arXiv:2211.03364. [Google Scholar]
- Lian, C.; Liu, M.; Zhang, J.; Shen, D. Hierarchical fully convolutional network for joint atrophy localization and Alzheimer’s disease diagnosis using structural MRI. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 42, 880–893. [Google Scholar] [CrossRef] [PubMed]
- Shao, W.; Peng, Y.; Zu, C.; Wang, M.; Zhang, D.; Alzheimer’s Disease Neuroimaging Initiative. Hypergraph based multi-task feature selection for multimodal classification of Alzheimer’s disease. Comput. Med. Imaging Graph. 2020, 80, 101663. [Google Scholar] [CrossRef] [PubMed]
- Saratxaga, C.L.; Moya, I.; Picón, A.; Acosta, M.; Moreno-Fernandez-De-Leceta, A.; Garrote, E.; Bereciartua-Perez, A. MRI deep learning-based solution for Alzheimer’s disease prediction. J. Pers. Med. 2021, 11, 902. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; Mchugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Berg, L. Clinical Dementia Rating (CDR). Psychopharmacol. Bull. 1988, 24, 637. [Google Scholar]
- Pfeffer, R.I.; Kurosaki, T.T.; Harrah, C.H.; Chance, J.M.; Filos, S. Measurement of Functional Activities in Older Adults in the Community. J. Gerontol. 1982, 37, 323–329. [Google Scholar] [CrossRef]
- Rosen, W.G.; Mohs, R.C.; Davis, K.L. A New Rating Scale for Alzheimer’s Disease. Am. J. Psychiatry 1984, 141, 1356–1364. [Google Scholar]
- Schmidt, M. Rey Auditory Verbal Learning Test: A Handbook; Western Psychological Services: Los Angeles, CA, USA, 1996. [Google Scholar]
- Prasher, V.; Farooq, A.; Holder, R. The Adaptive Behaviour Dementia Questionnaire (ABDQ): Screening questionnaire for dementia in Alzheimer’s disease in adults with Down syndrome. Res. Dev. Disabil. 2004, 25, 385–397. [Google Scholar] [CrossRef]
- Dickerson, B.C. Advances in quantitative magnetic resonance imaging-based biomarkers for Alzheimer disease. Alzheimers Res. Ther. 2010, 2, 21. [Google Scholar] [CrossRef]
- Zhou, Y.; Tan, C.; Wen, D.; Sun, H.; Han, W.; Xu, Y. The biomarkers for identifying preclinical Alzheimer’s disease via structural and functional magnetic resonance imaging. Front. Aging Neurosci. 2016, 8, 92. [Google Scholar] [CrossRef] [PubMed]
- Qing, Z.; Chen, F.; Lu, J.; Lv, P.; Li, W.; Liang, X.; Wang, M.; Wang, Z.; Zhang, X.; Zhang, B.; et al. Causal structural covariance network revealing atrophy progression in Alzheimer’s disease continuum. Hum. Brain Mapp. 2021, 42, 3950–3962. [Google Scholar] [CrossRef] [PubMed]
- Heung-Il, S. Deep Learning-Based Feature Representation for AD/MCI Classification. Med. Image Comput. Comput. Assist. Interv. MICCAI 2013, 16, 583–590. [Google Scholar]
- Andres, O. Ensembles of Deep Learning Architectures for the Early Diagnosis of the Alzheimer’s Disease. Int. J. Neural Syst. 2016, 26, 1650025. [Google Scholar]
- Li, M.D.; Chang, K.; Bearce, B.; Chang, C.Y.; Huang, A.J.; Campbell, J.P.; Brown, J.M.; Singh, P.; Hoebel, K.V.; Erdogmus, D.; et al. Siamese neural networks for continuous disease severity evaluation and change detection in medical imaging. NPJ Digit. Med. 2020, 3, 48. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wu, Z.; Zhao, S.; Wu, X.; Kuang, Y.; Yan, Y.; Ge, S.; Wang, K.; Fan, W.; Chen, X.; et al. PSENet: Psoriasis severity evaluation network. Proc. AAAI Conf. Artif. Intell. 2020, 34, 800–807. [Google Scholar] [CrossRef]
- Wu, Z.; Xiong, Y.; Yu, S.X.; Lin, D. Unsupervised feature learning via non-parametric instance discrimination. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 3733–3742. [Google Scholar]
- He, K.; Fan, H.; Wu, Y.; Xie, S.; Girshick, R. Momentum contrast for unsupervised visual representation learning. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 9729–9738. [Google Scholar]
- Chen, T.; Kornblith, S.; Norouzi, M.; Hinton, G. A simple framework for contrastive learning of visual representations. International conference on machine learning. PMLR 2020, 119, 1597–1607. [Google Scholar]
- Chen, X.; He, K. Exploring simple siamese representation learning. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Nashville, TN, USA, 19–25 June 2021; pp. 15750–15758. [Google Scholar]
- Khosla, P.; Teterwak, P.; Wang, C.; Sarna, A.; Tian, Y.; Isola, P.; Maschinot, A.; Liu, C. Supervised contrastive learning. Adv. Neural Inf. Process. Syst. 2020, 33, 18661–18673. [Google Scholar]
- Chen, T.; Kornblith, S.; Swersky, K.; Norouzi, M.; Hinton, G. Big self-supervised models are strong semi-supervised learners. Adv. Neural Inf. Process. Syst. 2020, 33, 22243–22255. [Google Scholar]
- Wang, X.; Zhang, R.; Shen, C.; Kong, T.; Li, L. Dense contrastive learning for self-supervised visual pre-training. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Nashville, TN, USA, 19–25 June 2021; pp. 3024–3033. [Google Scholar]
- Han, T.; Xie, W.; Zisserman, A. Self-supervised co-training for video representation learning. Adv. Neural Inf. Process. Syst. 2020, 33, 5679–5690. [Google Scholar]
- Grill, J.B.; Strub, F.; Altché, F.; Tallec, C.; Richemond, P.; Buchatskaya, E.; Doersch, C.; Pires, B.A.; Guo, Z.; Azar, M.; et al. Bootstrap your own latent-a new approach to self-supervised learning. Adv. Neural Inf. Process. Syst. 2020, 33, 21271–21284. [Google Scholar]
- Xie, S.; Gu, J.; Guo, D.; Qi, C.R.; Guibas, L.; Litany, O. Pointcontrast: Unsupervised pre-training for 3d point cloud understanding. In Proceedings of the Computer Vision–ECCV 2020, 16th European Conference, Glasgow, UK, 23–28 August 2020; Proceedings, Part III 16. Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 574–591. [Google Scholar]
- Tian, Y.; Krishnan, D.; Isola, P. Contrastive multiview coding. In Proceedings of the Computer Vision–ECCV 2020, 16th European Conference, Glasgow, UK, 23–28 August 2020; Proceedings, Part XI 16. Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 776–794. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage of Disease | AD | MCI | NC |
|---|---|---|---|
| Number | 149 | 263 | 221 |
| Sex (male/female) | 79/70 | 156/107 | 115/106 |
| Age | 76.3 | 75.8 | 77.4 |
| Number of Images | 542 | 1425 | 1030 |
| Pearson Correlation (%) | Spearman Correlation (%) | |
|---|---|---|
| APOE4 A1 | 27.74 | 28.078 |
| APOE4 A2 | 33.78 | 33.89 |
| NPI-Q | 40.04 | 50.59 |
| GDS | 23.25 | 31.96 |
| FAQ | 65.73 | 74.60 |
| MMSE | 57.956 | 68.51 |
| CDR | 70.81 | 85.77 |
| ODSS-MRI | 88.55 ± 0.86 | 87.12 ± 1.3 |
| NC vs. MCI | MCI vs. AD | NC vs. AD | |
|---|---|---|---|
| APOE4 A1 | |||
| APOE4 A2 | |||
| NPI-Q | |||
| GDS | |||
| FAQ | |||
| MMSE | |||
| CDR | |||
| ODSS-MRI |
| Tasks | Scores | Sensitivity(%) | Specificity(%) | Accuracy(%) |
|---|---|---|---|---|
| NC/MCI | FAQ | 32.09 | 99.35 | 68.06 |
| MMSE | 29.63 | 95.43 | 63.21 | |
| CDR | 99.25 | 94.87 | 97.41 | |
| ODSS-MRI | 100.00 | 89.85 | 95.62 | |
| MCI/AD | FAQ | 88.33 | 33.33 | 50.79 |
| MMSE | 76.09 | 40.88 | 55.02 | |
| CDR | 1.03 | 99.25 | 73.15 | |
| ODSS-MRI | 75.73 | 94.55 | 89.42 | |
| NC/AD | FAQ | 91.38 | 100.00 | 97.63 |
| MMSE | 93.33 | 100.00 | 98.10 | |
| CDR | 100.00 | 100.00 | 100.00 | |
| ODSS-MRI | 100.00 | 100.00 | 100.00 |
| Tasks | Scores | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|---|
| FAQ | AD | 81.54 | 77.01 | 77.68 |
| MCI | 19.55 | 96.35 | 57.86 | |
| NC | 99.35 | 66.32 | 77.90 | |
| MMSE | AD | 72.16 | 82.66 | 80.85 |
| MCI | 20.74 | 89.46 | 56.56 | |
| NC | 95.43 | 62.40 | 73.94 | |
| CDR | AD | 1.03 | 99.57 | 82.56 |
| MCI | 98.52 | 63.70 | 80.43 | |
| NC | 94.87 | 99.46 | 97.86 | |
| ODSS-MRI | AD | 75.73 | 96.82 | 93.04 |
| MCI | 94.55 | 85.00 | 89.57 | |
| NC | 89.85 | 100.00 | 96.52 |
| ODSS-MRI | MMSE | CDR | |
|---|---|---|---|
| Variance | 0.151101 | 0.027904 | 0.022673 |
| Standard deviation | 0.388717 | 0.167044 | 0.150577 |
| Quartile deviation | 0.849023 | 0.2 | 0.166667 |
| Variation ratio | 0.998261 | 0.801418 | 0.510676 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Fan, W.; Chen, X.; Li, W.; on behalf of the for Alzheimer’s Disease Neuroimaging Initiative. The Objective Dementia Severity Scale Based on MRI with Contrastive Learning: A Whole Brain Neuroimaging Perspective. Sensors 2023, 23, 6871. https://doi.org/10.3390/s23156871
Zhang Y, Fan W, Chen X, Li W, on behalf of the for Alzheimer’s Disease Neuroimaging Initiative. The Objective Dementia Severity Scale Based on MRI with Contrastive Learning: A Whole Brain Neuroimaging Perspective. Sensors. 2023; 23(15):6871. https://doi.org/10.3390/s23156871
Chicago/Turabian StyleZhang, Yike, Wenliang Fan, Xi Chen, Wei Li, and on behalf of the for Alzheimer’s Disease Neuroimaging Initiative. 2023. "The Objective Dementia Severity Scale Based on MRI with Contrastive Learning: A Whole Brain Neuroimaging Perspective" Sensors 23, no. 15: 6871. https://doi.org/10.3390/s23156871
APA StyleZhang, Y., Fan, W., Chen, X., Li, W., & on behalf of the for Alzheimer’s Disease Neuroimaging Initiative. (2023). The Objective Dementia Severity Scale Based on MRI with Contrastive Learning: A Whole Brain Neuroimaging Perspective. Sensors, 23(15), 6871. https://doi.org/10.3390/s23156871