Willingness to Self-Collect a Sample for HPV-Based Cervical Cancer Screening in a Well-Screened Cohort: HPV FOCAL Survey Results

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Exit Survey
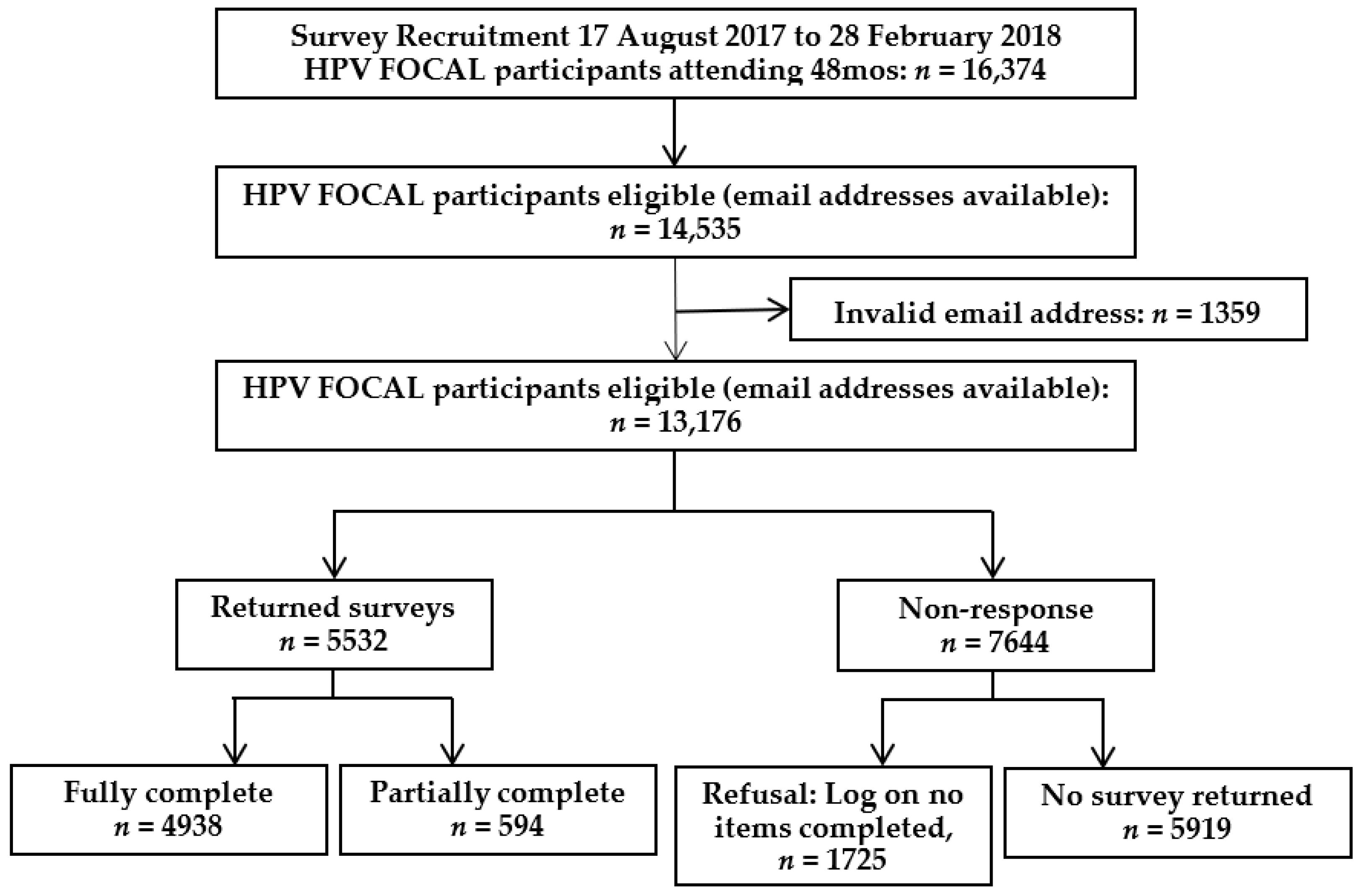
2.2. Response Rate and Inclusion Criteria
2.3. Statistical Model
3. Results
3.1. Characteristics of Study Population
3.2. Willingness to Self-Collect
3.3. Multivariable Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castellsagué, X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol. Oncol. 2008, 110 (Suppl. S2), 4–7. [Google Scholar] [CrossRef] [PubMed]
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human Papillomavirus Is a Necessary Cause. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Steben, M.; Thompson, M.T.; Rodier, C.; Mallette, N.; Racovitan, V.; DeAngelis, F.; Stutz, M.; Rampakakis, E. A Review of the Impact and Effectiveness of the Quadrivalent Human Papillomavirus Vaccine: 10 Years of Clinical Experience in Canada. J. Obstet. Gynaecol. Can. 2018, 40, 1635–1645. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, H.B.; Trotter, C.; Hickman, M.; Audrey, S. Barriers and facilitators to HPV vaccination of young women in high-income countries: A qualitative systematic review and evidence synthesis. BMC Public Health 2014, 14, 700. [Google Scholar] [CrossRef] [Green Version]
- WHO. Primary and Secondary Prevention of Cancer: Response by Country. 2020, p. 1. Available online: https://apps.who.int/gho/data/view.main.24766 (accessed on 25 May 2021).
- BC Cancer; van Niekerk, D. BC Cancer Cervix Screening Program Overview. 2021. Available online: http://www.bccancer.bc.ca/screening/Documents/Cervix-Program-Overview.pdf (accessed on 24 May 2021).
- Ogilvie, G.S.; van Niekerk, D.; Krajden, M.; Smith, L.W.; Cook, D.; Gondara, L.; Ceballos, K.; Quinlan, D.; Lee, M.; Martin, R.E.; et al. Effect of screening with primary cervical HPV testing vs cytology testing on high-grade cervical intraepithelial neoplasia at 48 months: The HPV FOCAL randomized clinical trial. JAMA—J. Am. Med. Assoc. 2018, 320, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Mayrand, M.-H.; Duarte-Franco, E.; Rodrigues, I.; Walter, S.D.; Hanley, J.; Ferenczy, A.; Ratnam, S.; Coutlée, F.; Franco, E. Human Papillomavirus DNA versus Papanicolaou Screening Tests for Cervical Cancer. N. Engl. J. Med. 2007, 357, 1579–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbyn, M.; Verdoodt, F.; Snijders, P.J.F.; Verhoef, V.M.J.; Suonio, E.; Dillner, L.; Minozzi, S.; Bellisario, C.; Banzi, R.; Zhao, F.-H.; et al. Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: A meta-analysis. Lancet Oncol. 2014, 15, 172–183. [Google Scholar] [CrossRef]
- Petignat, P.; Faltin, D.L.; Bruchim, I.; Tramèr, M.R.; Franco, E.L.; Coutlée, F. Are self-collected samples comparable to physician-collected cervical specimens for human papillomavirus DNA testing? A systematic review and meta-analysis. Gynecol. Oncol. 2007, 105, 530–535. [Google Scholar] [CrossRef]
- Australian Government D of H. Quick Reference Guide—Self-Collected Vaginal Sample for HPV Test. Available online: https://www.health.gov.au/sites/default/files/documents/2019/10/national-cervical-screening-program-quick-reference-guide-self-collected-cervical-screening-tests.pdf (accessed on 10 June 2021).
- RIVM: National Institute For Public Health and the Environment. Cervical Cancer Screening Program. 2022. Available online: https://www.rivm.nl/en/cervical-cancer-screening-programme (accessed on 26 April 2022).
- Regionala Cancercentrum I Samverkan. National Care Program Cervical Cancer Prevention. 2021. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/livmoderhalscancerprevention/vardprogram/ (accessed on 10 June 2021).
- Ogilvie, G.; Krajden, M.; Maginley, J.; Isaac-Renton, J.; Hislop, G.; Elwood-Martin, R.; Sherlock, C.; Taylor, D.; Rekart, M. Feasibility of self-collection of specimens for human papillomavirus testing in hard-to-reach women. Can. Med Assoc. J. 2007, 177, 480–483. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Smith, S.B.; Temin, S.; Sultana, F.; Castle, P. Detecting cervical precancer and reaching underscreened women by using HPV testing on self samples: Updated meta-analyses. BMJ 2018, 363, k4823. [Google Scholar] [CrossRef] [Green Version]
- Morgan, K.; Azzani, M.; Khaing, S.L.; Wong, Y.L.; Su, T.T. Acceptability of Women Self-Sampling versus Clinician-Collected Samples for HPV DNA Testing: A Systematic Review. J. Low Genit. Tract. Dis. 2019, 23, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Breithaupt, L.; Das Marais, A.; Rastas, C.; Richman, A.; Barclay, L.; Brewer, N.T.; Smith, J.S. Acceptability and ease of use of mailed HPV self-collection among infrequently screened women in North Carolina. Sex. Transm. Infect. 2017, 94, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, G.S.; Krajden, M.; Van Niekerk, D.J.; Martin, R.E.; Ehlen, T.G.; Ceballos, K.; Smith, L.W.; Kan, L.; Cook, D.A.; Peacock, S.; et al. Primary cervical cancer screening with HPV testing compared with liquid-based cytology: Results of round 1 of a randomised controlled trial—The HPV FOCAL Study. Br. J. Cancer 2012, 107, 1917–1924. [Google Scholar] [CrossRef]
- Ogilvie, G.S.; Van Niekerk, D.J.; Krajden, M.; Martin, R.E.; Ehlen, T.G.; Ceballos, K.; Peacock, S.J.; Smith, L.W.; Kan, L.; Cook, D.A.; et al. A randomized controlled trial of Human Papillomavirus (HPV) testing for cervical cancer screening: Trial design and preliminary results (HPV FOCAL Trial). BMC Cancer 2010, 10, 111. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.W.; Khurshed, F.; Van Niekerk, D.J.; Krajden, M.; Greene, S.B.; Hobbs, S.; Coldman, A.J.; Franco, E.L.; Ogilvie, G.S. Women’s intentions to self-collect samples for human papillomavirus testing in an organized cervical cancer screening program. BMC Public Health 2014, 14, 1060. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.W.; Racey, C.S.; Gondara, L.; Krajden, M.; Lee, M.; Martin, R.E.; Stuart, G.; Peacock, S.; Coldman, A.J.; Franco, E.L.; et al. Women’s acceptability of and experience with primary human papillomavirus testing for cervix screening: HPV FOCAL trial cross-sectional online survey results. BMJ Open 2021, 11, e052084. [Google Scholar] [CrossRef]
- AAPOR. Standard Definitions: Final Dispositions of Case Codes and Outcome Rates for Surveys, 9th ed.; American Association for Public Opinion Research: Atlanta, GA, USA, 2016. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 14 June 2021).
- Yeh, P.T.; Kennedy, C.E.; De Vuyst, H.; Narasimhan, M. Self-sampling for human papillomavirus (HPV) testing: A systematic review and meta-Analysis. BMJ Glob. Health 2019, 4, e001351. [Google Scholar] [CrossRef]
- BC Cancer. BC Cancer Cervix Screening 2018 Program Results. 2020. Available online: http://www.bccancer.bc.ca/screening/Documents/Cervix_ProgramResults2016_OPT.pdf (accessed on 5 July 2021).
- Tisci, S.; Shen, Y.H.; Fife, D.; Huang, J.; Goycoolea, J.; Ma, C.P.; Belinson, J.; Huang, R.-D.; Qiao, Y.-L. Patient Acceptance of Self-Sampling for Human Papillomavirus in Rural China. J. Low. Genit. Tract Dis. 2003, 7, 107–116. [Google Scholar] [CrossRef]
- Anhang, R.; Nelson, J.A.; Telerant, R.; Chiasson, M.A.; Wright, T.C. Acceptability of self-collection of specimens for HPV DNA testing in an urban population (Abstract). J. Women’s Health 2005, 14, 721–728. [Google Scholar] [CrossRef]
- Gakidou, E.; Nordhagen, S.; Obermeyer, Z. Coverage of cervical cancer screening in 57 countries: Low average levels and large inequalities. PLoS Med. 2008, 5, 0863–0868. [Google Scholar] [CrossRef]
- Sarai Racey, C.; Withrow, D.R.; Gesink, D. Self-collected HPV testing improves participation in cervical cancer screening: A systematic review and meta-analysis. Can. J. Public Health 2013, 104, 159–166. [Google Scholar] [CrossRef]
- Duke, P.; Godwin, M.; Ratnam, S.; Dawson, L.; Fontaine, D.; Lear, A.; Traverso-Yepez, M.; Graham, W.J.; Ravalia, M.; Mugford, G.; et al. Effect of vaginal self-sampling on cervical cancer screening rates: A community-based study in Newfoundland. BMC Womens Health 2015, 15, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Consolidated Guideline on Self-Care Interventions for Health: Sexual and Reproductive Health and Rights; WHO: Geneva, Switzerland, 2019; Volume 23, Available online: https://apps.who.int/iris/bitstream/handle/10665/325480/9789241550550-eng.pdf?ua=1 (accessed on 7 July 2021).
- Camara, H.; Zhang, Y.; Lafferty, L.; Vallely, A.J.; Guy, R.; Kelly-Hanku, A. Self-collection for HPV-based cervical screening: A qualitative evidence meta-synthesis. BMC Public Health 2021, 21, 1503. [Google Scholar] [CrossRef] [PubMed]
- Conner, M.; Norman, P. Reference Module in Neuroscience and Biobehavioral Psychology. In Health Behavior, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 1–33. [Google Scholar] [CrossRef]


{kind=link}
| Total | Not Willing 1 | Willing 2 | p Value | |
|---|---|---|---|---|
| 4945 | 2371 | 2574 | ||
| Median Age (interquartile range (IQR)) | 53.8 (45.4, 61.5) | 53.4 (45.0, 61.2) | 54.1 (45.9, 61.6) | 0.026 |
| Education Level | ||||
| Incomplete post-secondary or less | 1601 (32.4%) | 854 (36.0%) | 747 (29.0%) | <0.001 |
| Complete college or higher | 3308 (66.9%) | 1496 (63.1%) | 1812 (70.4%) | |
| Missing | 36 (0.7%) | 21 (0.9%) | 15 (0.6%) | |
| Marital Status | ||||
| Living without a partner | 1114 (22.5%) | 524 (22.1%) | 590 (22.9%) | 0.762 |
| Living with a partner | 3792 (76.7%) | 1829 (77.1%) | 1963 (76.3%) | |
| Missing | 39 (0.8%) | 18 (0.8%) | 21 (0.8%) | |
| Income | ||||
| Under or equal to $75,000 | 1498 (30.3%) | 735 (31.0%) | 763 (29.6%) | <0.001 |
| Over $75,000 | 3009 (60.8%) | 1380 (58.2%) | 1629 (63.3%) | |
| Missing | 438 (8.9%) | 256 (10.8%) | 182 (7.1%) | |
| I know more about HPV and cervical cancer now than I did before I participated in the study: | ||||
| Agree | 1672 (33.8%) | 766 (32.3%) | 906 (35.2%) | 0.071 |
| Disagree | 1458 (29.5%) | 688 (29.0%) | 770 (29.9%) | |
| Neutral | 1703 (34.4%) | 860 (36.3%) | 843 (32.8%) | |
| Not Sure | 98 (2.0%) | 51 (2.2%) | 47 (1.8%) | |
| Missing | 14 (0.3%) | 6 (0.3%) | 8 (0.3%) | |
| Having an HPV test to screen for cervical cancer instead of a Pap smear is acceptable to me: | ||||
| Agree | 3107 (62.8%) | 1379 (58.2%) | 1728 (67.1%) | <0.001 |
| Disagree | 573 (11.6%) | 324 (13.7%) | 249 (9.7%) | |
| Don’t Know | 476 (9.6%) | 238 (10.0%) | 238 (9.2%) | |
| Neutral | 775 (15.7%) | 422 (17.8%) | 353 (13.7%) | |
| Missing | 14 (0.3%) | 8 (0.3%) | 6 (0.2%) | |
| Collecting my own sample for cervical cancer screening would be: Acceptable | ||||
| Acceptable | 3356 (67.9%) | 996 (42.0%) | 2360 (91.7%) | <0.001 |
| Unacceptable | 1416 (28.6%) | 1256 (53.0%) | 160 (6.2%) | |
| Missing | 173 (3.5%) | 119 (5.0%) | 54 (2.1%) | |
| Adjusted Odds Ratio (OR) | 95% Confidence Interval (CI) | |
|---|---|---|
| Median Age | 1.01 * | 1.00, 1.02 |
| Education Level | ||
| Incomplete post-secondary or less | Reference | |
| Complete college or higher | 1.31 ** | 1.12, 1.54 |
| Marital Status | ||
| Living without a partner | Reference | |
| Living with a partner | 0.93 | 0.77, 1.12 |
| Income | ||
| Under or equal to $75,000 | Reference | |
| Over $75,000 | 1.09 | 0.92, 1.29 |
| I know more about HPV and cervical cancer now than I did before I participated in the study: | ||
| Disagree | Reference | |
| Agree | 0.98 | 0.82, 1.18 |
| Neutral | 0.83 * | 0.69, 0.99 |
| Not Sure | 0.80 | 0.47, 1.37 |
| Having an HPV test to screen for cervical cancer instead of a Pap smear is acceptable to me: | ||
| Disagree | Reference | |
| Agree | 1.45 * | 1.15, 1.82 |
| Don’t Know | 1.30 | 0.95, 1.78 |
| Neutral | 0.96 | 0.73, 1.26 |
| Collecting my own sample for cervical cancer screening would be: Acceptable | ||
| Unacceptable | Reference | |
| Acceptable | 17.9 ** | 14.9, 21.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lesack, A.; Smith, L.W.; Racey, C.S.; Gondara, L.; Krajden, M.; Lee, M.; Martin, R.E.; Stuart, G.; Peacock, S.; Franco, E.L.; et al. Willingness to Self-Collect a Sample for HPV-Based Cervical Cancer Screening in a Well-Screened Cohort: HPV FOCAL Survey Results. Curr. Oncol. 2022, 29, 3860-3869. https://doi.org/10.3390/curroncol29060308
Lesack A, Smith LW, Racey CS, Gondara L, Krajden M, Lee M, Martin RE, Stuart G, Peacock S, Franco EL, et al. Willingness to Self-Collect a Sample for HPV-Based Cervical Cancer Screening in a Well-Screened Cohort: HPV FOCAL Survey Results. Current Oncology. 2022; 29(6):3860-3869. https://doi.org/10.3390/curroncol29060308
Chicago/Turabian StyleLesack, Anne, Laurie W. Smith, C. Sarai Racey, Lovedeep Gondara, Mel Krajden, Marette Lee, Ruth Elwood Martin, Gavin Stuart, Stuart Peacock, Eduardo L. Franco, and et al. 2022. "Willingness to Self-Collect a Sample for HPV-Based Cervical Cancer Screening in a Well-Screened Cohort: HPV FOCAL Survey Results" Current Oncology 29, no. 6: 3860-3869. https://doi.org/10.3390/curroncol29060308
APA StyleLesack, A., Smith, L. W., Racey, C. S., Gondara, L., Krajden, M., Lee, M., Martin, R. E., Stuart, G., Peacock, S., Franco, E. L., van Niekerk, D., & Ogilvie, G. S. (2022). Willingness to Self-Collect a Sample for HPV-Based Cervical Cancer Screening in a Well-Screened Cohort: HPV FOCAL Survey Results. Current Oncology, 29(6), 3860-3869. https://doi.org/10.3390/curroncol29060308