
Biocompatibility and Osteogenic Potential of Calcium Silicate-Based Cement Combined with Enamel Matrix Derivative: Effects on Human Bone Marrow-Derived Stem Cells



Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Bone Marrow-Derived Stem Cells (hBMSCs)
2.2. Production of Retrograde Filling Materials Disks
2.3. Classification of the Groups
2.4. Cell Viability Measurement
2.5. Cell Migration Assay
2.6. Alkaline Phosphatase (ALP) Activity
2.7. Alizarin Red S (ARS) Staining Assay
2.8. Statistical Analysis
3. Results
3.1. Cell Viability Measurement
3.2. Cell Migration Assay
3.3. Alkaline Phosphatase (ALP) Activity
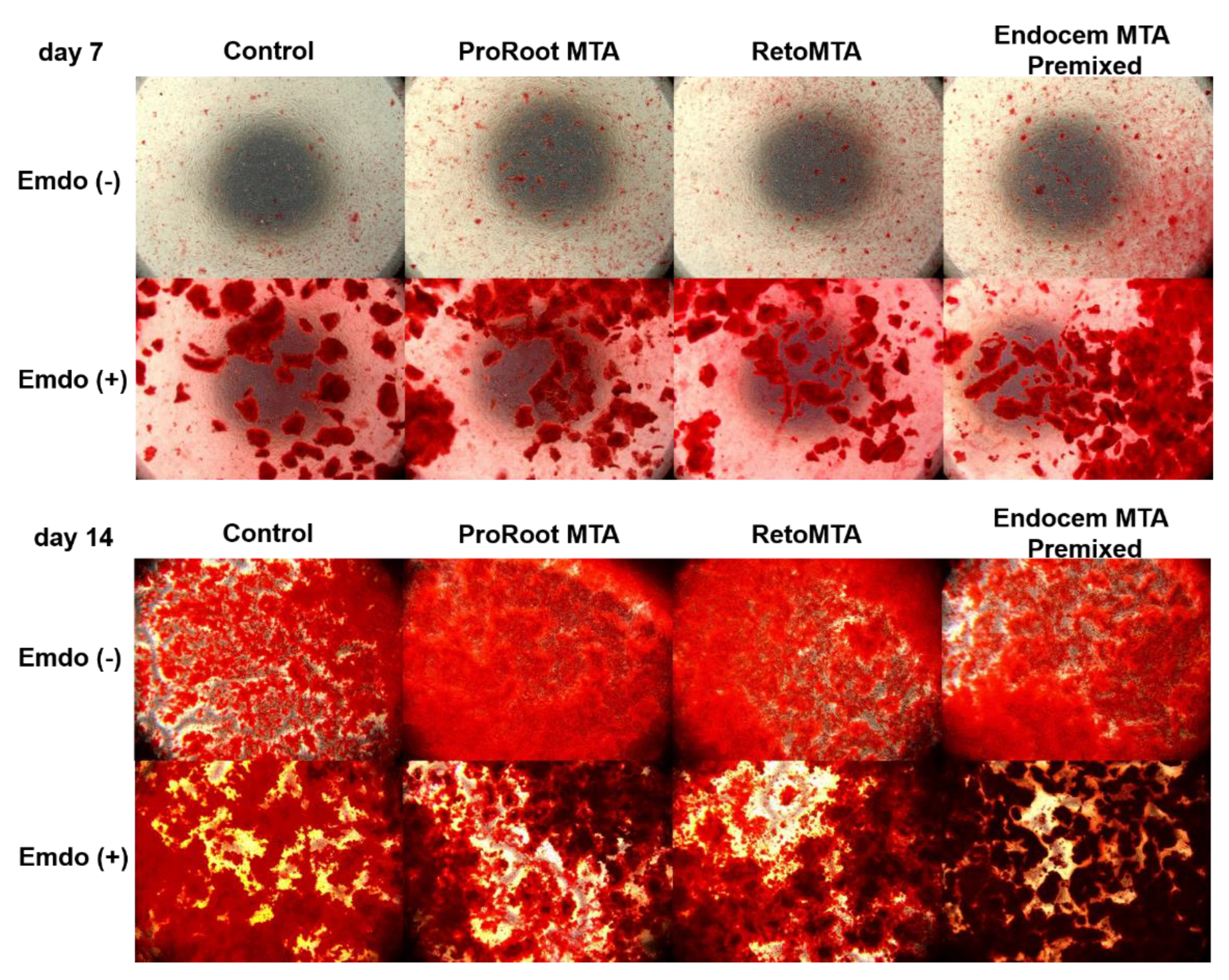
3.4. Alizarin Red-S (ARS) Staining Assay
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.; Kratchman, S. Modern endodontic surgery concepts and practice: A review. J. Endod. 2006, 32, 601–623. [Google Scholar] [CrossRef]
- Kang, S.; Ha, S.W.; Kim, U.; Kim, S.; Kim, E. A One-Year Radiographic Healing Assessment after Endodontic Microsurgery Using Cone-Beam Computed Tomographic Scans. J. Clin. Med. 2020, 9, 3714. [Google Scholar] [CrossRef]
- Schloss, T.; Sonntag, D.; Kohli, M.R.; Setzer, F.C. A Comparison of 2- and 3-dimensional Healing Assessment after Endodontic Surgery Using Cone-beam Computed Tomographic Volumes or Periapical Radiographs. J. Endod. 2017, 43, 1072–1079. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part I: Chemical, physical, and antibacterial properties. J. Endod. 2010, 36, 16–27. [Google Scholar] [CrossRef] [PubMed]
- D’Antò, V.; Di Caprio, M.P.; Ametrano, G.; Simeone, M.; Rengo, S.; Spagnuolo, G. Effect of mineral trioxide aggregate on mesenchymal stem cells. J. Endod. 2010, 36, 1839–1843. [Google Scholar] [CrossRef] [PubMed]
- Ber, B.S.; Hatton, J.F.; Stewart, G.P. Chemical modification of proroot mta to improve handling characteristics and decrease setting time. J. Endod. 2007, 33, 1231–1234. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Noula, G.; Lambrianidis, T. Ex vivo study of the efficiency of two techniques for the removal of mineral trioxide aggregate used as a root canal filling material. J. Endod. 2008, 34, 1239–1242. [Google Scholar] [CrossRef]
- Chng, H.K.; Islam, I.; Yap, A.U.; Tong, Y.W.; Koh, E.T. Properties of a new root-end filling material. J. Endod. 2005, 31, 665–668. [Google Scholar] [CrossRef]
- Cummings, G.; Torabinejad, M. RS 53 Mineral trioxide aggregate (MTA) as an isolating barrier for internal bleaching. J. Endod. 1995, 4, 228. [Google Scholar] [CrossRef]
- Dominguez, M.S.; Witherspoon, D.E.; Gutmann, J.L.; Opperman, L.A. Histological and scanning electron microscopy assessment of various vital pulp-therapy materials. J. Endod. 2003, 29, 324–333. [Google Scholar] [CrossRef]
- Torabinejad, M.; Hong, C.; McDonald, F.; Ford, T.P. Physical and chemical properties of a new root-end filling material. J. Endod. 1995, 21, 349–353. [Google Scholar] [CrossRef]
- Chen, I.; Karabucak, B.; Wang, C.; Wang, H.G.; Koyama, E.; Kohli, M.R.; Nah, H.D.; Kim, S. Healing after root-end microsurgery by using mineral trioxide aggregate and a new calcium silicate-based bioceramic material as root-end filling materials in dogs. J. Endod. 2015, 41, 389–399. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.J.; Shen, Z.S.; Qin, W.; Lin, Z. A comparison of the sealing abilities between Biodentine and MTA as root-end filling materials and their effects on bone healing in dogs after periradicular surgery. J. Appl. Oral Sci. 2019, 27, e20180693. [Google Scholar] [CrossRef] [PubMed]
- Sluyk, S.; Moon, P.; Hartwell, G. Evaluation of setting properties and retention characteristics of mineral trioxide aggregate when used as a furcation perforation repair material. J. Endod. 1998, 24, 768–771. [Google Scholar] [CrossRef]
- Malkondu, Ö.; Karapinar Kazandağ, M.; Kazazoğlu, E. A review on biodentine, a contemporary dentine replacement and repair material. Biomed. Res. Int. 2014, 2014, 160951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Chang, J.; Hu, S. A study on the sealing ability and antibacterial activity of Ca3SiO5/CaCl2 composite cement for dental applications. Dent. Mater. J. 2012, 31, 617–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Shen, Y.; Stojicic, S.; Haapasalo, M. Biocompatibility of two novel root repair materials. J. Endod. 2011, 37, 793–798. [Google Scholar] [CrossRef]
- Sarkar, N.K.; Caicedo, R.; Ritwik, P.; Moiseyeva, R.; Kawashima, I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J. Endod. 2005, 31, 97–100. [Google Scholar] [CrossRef]
- Chung, C.J.; Kim, E.; Song, M.; Park, J.W.; Shin, S.J. Effects of two fast-setting calcium-silicate cements on cell viability and angiogenic factor release in human pulp-derived cells. Odontology 2016, 104, 143–151. [Google Scholar] [CrossRef]
- Wongwatanasanti, N.; Jantarat, J.; Sritanaudomchai, H.; Hargreaves, K.M. Effect of Bioceramic Materials on Proliferation and Odontoblast Differentiation of Human Stem Cells from the Apical Papilla. J. Endod. 2018, 44, 1270–1275. [Google Scholar] [CrossRef]
- MTA Mall. Available online: http://www.mtamall.com/product/detail.html?product_no=181&cate_no=24&display_group=1 (accessed on 22 October 2021).
- Chung, H.; Yang, W.; Kim, M.; Ko, H. Comparison of the effects of enamel matrix derivative and mineral trioxide aggregate on the mineralization potential of human cementum-derived cells. J. Dent. Sci. 2011, 6, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Matarasso, M.; Iorio-Siciliano, V.; Blasi, A.; Ramaglia, L.; Salvi, G.E.; Sculean, A. Enamel matrix derivative and bone grafts for periodontal regeneration of intrabony defects. A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1581–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aimetti, M.; Ferrarotti, F.; Mariani, G.M.; Romano, F. A novel flapless approach versus minimally invasive surgery in periodontal regeneration with enamel matrix derivative proteins: A 24-month randomized controlled clinical trial. Clin. Oral Investig. 2017, 21, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Lossdörfer, S.; Sun, M.; Götz, W.; Dard, M.; Jäger, A. Enamel matrix derivative promotes human periodontal ligament cell differentiation and osteoprotegerin production in vitro. J. Dent. Res. 2007, 86, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.-R.; Emara, R.; Taher, M.M.; Al-Allaf, F.A.; Almalki, M.; Almasri, M.A.; Siddiqui, S.S. Effects of mineral trioxide aggregate, calcium hydroxide, biodentine and Emdogain on osteogenesis, Odontogenesis, angiogenesis and cell viability of dental pulp stem cells. BMC Oral Health 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Scarparo, R.K.; Dondoni, L.; Böttcher, D.E.; Grecca, F.S.; Figueiredo, J.A.; Batista, E.L., Jr. Apical periodontium response to enamel matrix derivative as an intracanal medication in rat immature teeth with pulp necrosis: Radiographic and histologic findings. J. Endod. 2012, 38, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Sarmast, N.D.; Shadmehr, E.; Angelov, N.; Shabahang, S.; Torabinejad, M. Application of enamel matrix derivative (Emdogain) in endodontic therapy: A comprehensive literature review. J. Endod. 2018, 44, 1066–1079. [Google Scholar] [CrossRef]
- Fransson, H.; Petersson, K.; Davies, J. Dentine sialoprotein and Collagen I expression after experimental pulp capping in humans using Emdogain® Gel. Int. Endod. J. 2011, 44, 259–267. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, Y.; Ge, L. Effects of the enamel matrix derivative on the proliferation and odontogenic differentiation of human dental pulp cells. J. Dent. 2014, 42, 53–59. [Google Scholar] [CrossRef]
- Riss, T.L.; Moravec, R.A.; Niles, A.L.; Duellman, S.; Benink, H.A.; Worzella, T.J.; Minor, L. Cell viability assays. In Assay Guidance Manual; Eli Lilly & Company and the National Center for Advancing Translational Sciences: Bethesda, MD, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK144065/ (accessed on 22 October 2021).
- Gorduysus, M.; Avcu, N.; Gorduysus, O.; Pekel, A.; Baran, Y.; Avcu, F.; Ural, A.U. Cytotoxic effects of four different endodontic materials in human periodontal ligament fibroblasts. J. Endod. 2007, 33, 1450–1454. [Google Scholar] [CrossRef] [PubMed]
- Jafarnia, B.; Jiang, J.; He, J.; Wang, Y.-H.; Safavi, K.E.; Zhu, Q. Evaluation of cytotoxicity of MTA employing various additives. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Hirschman, W.R.; Wheater, M.A.; Bringas, J.S.; Hoen, M.M. Cytotoxicity comparison of three current direct pulp-capping agents with a new bioceramic root repair putty. J. Endod. 2012, 38, 385–388. [Google Scholar] [CrossRef]
- Wei, W.; Qi, Y.-P.; Nikonov, S.Y.; Niu, L.-N.; Messer, R.L.; Mao, J.; Primus, C.M.; Pashley, D.H.; Tay, F.R. Effects of an experimental calcium aluminosilicate cement on the viability of murine odontoblast-like cells. J. Endod. 2012, 38, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Dojindo Molecular Technologies. Available online: https://dojindo.com/product/cell-counting-kit-8/ (accessed on 22 October 2021).
- Luo, J.; Xu, J.; Cai, J.; Wang, L.; Sun, Q.; Yang, P. The in vitro and in vivo osteogenic capability of the extraction socket-derived early healing tissue. J. Periodontol. 2016, 87, 1057–1066. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, D.; Kim, H.-M.; Kye, M.; Kim, S.-Y. Biological Characteristics and Odontogenic Differentiation Effects of Calcium Silicate-Based Pulp Capping Materials. Materials 2021, 14, 4661. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, D.; Song, D.; Kim, H.-M.; Kim, S.-Y. Biocompatibility and bioactivity of set direct pulp capping materials on human dental pulp stem cells. Materials 2020, 13, 3925. [Google Scholar] [CrossRef]
- Bortoluzzi, E.A.; Niu, L.-N.; Palani, C.D.; El-Awady, A.R.; Hammond, B.D.; Pei, D.-D.; Tian, F.-C.; Cutler, C.W.; Pashley, D.H.; Tay, F.R. Cytotoxicity and osteogenic potential of silicate calcium cements as potential protective materials for pulpal revascularization. Dent. Mater. 2015, 31, 1510–1522. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.G.; Ciapetti, G.; Taddei, P.; Perut, F.; Tinti, A.; Cardoso, M.V.; Van Meerbeek, B.; Prati, C. Apatite formation on bioactive calcium-silicate cements for dentistry affects surface topography and human marrow stromal cells proliferation. Dent. Mater. 2010, 26, 974–992. [Google Scholar] [CrossRef]
- Matsuya, S.; Takagi, S.; Chow, L.C. Effect of mixing ratio and pH on the reaction between Ca4(PO4)2O and CaHPO4. J. Mater. Sci. Mater. Med. 2000, 11, 305–311. [Google Scholar] [CrossRef]
- Santiago, M.C.; Gomes-Cornélio, A.L.; de Oliveira, L.A.; Tanomaru-Filho, M.; Salles, L.P. Calcium silicate-based cements cause environmental stiffness and show diverse potential to induce osteogenesis in human osteoblastic cells. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Rathinam, E.; Govindarajan, S.; Rajasekharan, S.; Declercq, H.; Elewaut, D.; De Coster, P.; Martens, L.; Leybaert, L. The calcium dynamics of human dental pulp stem cells stimulated with tricalcium silicate-based cements determine their differentiation and mineralization outcome. Sci. Rep. 2021, 11, 1–13. [Google Scholar]
- Mladenović, Ž.; Johansson, A.; Willman, B.; Shahabi, K.; Björn, E.; Ransjö, M. Soluble silica inhibits osteoclast formation and bone resorption in vitro. Acta Biomater. 2014, 10, 406–418. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Siboni, F.; Botero, T.; Bossù, M.; Riccitiello, F.; Prati, C. Calcium silicate and calcium hydroxide materials for pulp capping: Biointeractivity, porosity, solubility and bioactivity of current formulations. J. Appl. Biomater. Funct. Mater. 2015, 13, 43–60. [Google Scholar] [CrossRef]
- Yuan, W.; He, X.; Zhang, J.; Chen, Y.; Gong, T.; Zhu, Y. Calcium phosphate silicate and calcium silicate cements suppressing osteoclasts activity through cytokine regulation. J. Nanosc. Nanotechnol. 2018, 18, 6799–6804. [Google Scholar] [CrossRef]
- Ishizaki, N.T.; Matsumoto, K.; Kimura, Y.; Wang, X.; Yamashita, A. Histopathological study of dental pulp tissue capped with enamel matrix derivative. J. Endod. 2003, 29, 176–179. [Google Scholar] [CrossRef]
- Guven, E.P.; Yalvac, M.E.; Sahin, F.; Yazici, M.M.; Rizvanov, A.A.; Bayirli, G. Effect of dental materials calcium hydroxide-containing cement, mineral trioxide aggregate, and enamel matrix derivative on proliferation and differentiation of human tooth germ stem cells. J. Endod. 2011, 37, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Boyan, B.D.; Weesner, T.; Lohmann, C.; Andreacchio, D.; Carnes, D.; Dean, D.; Cochran, D.; Schwartz, Z. Porcine fetal enamel matrix derivative enhances bone formation induced by demineralized freeze dried bone allograft in vivo. J. Periodontol. 2000, 71, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Kawase, T.; Okuda, K.; Momose, M.; Kato, Y.; Yoshie, H.; Burns, D.M. Enamel matrix derivative (EMDOGAIN®) rapidly stimulates phosphorylation of the MAP kinase family and nuclear accumulation of smad2 in both oral epithelial and fibroblastic human cells. J. Periodontal Res. 2001, 36, 367–376. [Google Scholar] [CrossRef]
- Kawase, T.; Okuda, K.; Yoshie, H.; Burns, D.M. Anti-TGF-β antibody blocks enamel matrix derivative-induced upregulation of p21WAF1/cip1 and prevents its inhibition of human oral epithelial cell proliferation. J. Periodontal Res. 2002, 37, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Kémoun, P.; Gronthos, S.; Snead, M.L.; Rue, J.; Courtois, B.; Vaysse, F.; Salles, J.-P.; Brunel, G. The role of cell surface markers and enamel matrix derivatives on human periodontal ligament mesenchymal progenitor responses in vitro. Biomaterials 2011, 32, 7375–7388. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Manufacturer | Composition | Batch Number |
|---|---|---|---|
| ProRoot MTA | Dentsply Tulsa Dental Specialties, Tulsa, OK, USA | Portland cement (tricalcium silicate, dicalcium silicate, and tricalcium aluminate) 75% Calcium sulfate dihydrate (gypsum) 5% Bismuth oxide 20% | 0000186484 |
| RetroMTA | BioMTA, Seoul, Korea | Calcium carbonate 60–80% Silicon dioxide 5–15% Aluminum oxide 5–10% Calcium zirconia complex 20–30% | RM1810D14 |
| Endocem MTA Premixed | Maruchi, Wonju, Korea | Natural pure cement Bismuth trioxide | C2304160716 |
| Emdogain Gel | Straumann, Basel, Switzerland | Amelogenin 90% The remainder is proline-rich nonamelogenin, tuftelins, tuft proteins, ameloblastin, and amelins | ISO 15223-1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-M.; Lee, D.; Kim, S.-Y. Biocompatibility and Osteogenic Potential of Calcium Silicate-Based Cement Combined with Enamel Matrix Derivative: Effects on Human Bone Marrow-Derived Stem Cells. Materials 2021, 14, 7750. https://doi.org/10.3390/ma14247750
Kim H-M, Lee D, Kim S-Y. Biocompatibility and Osteogenic Potential of Calcium Silicate-Based Cement Combined with Enamel Matrix Derivative: Effects on Human Bone Marrow-Derived Stem Cells. Materials. 2021; 14(24):7750. https://doi.org/10.3390/ma14247750
Chicago/Turabian StyleKim, Hye-Min, Donghee Lee, and Sin-Young Kim. 2021. "Biocompatibility and Osteogenic Potential of Calcium Silicate-Based Cement Combined with Enamel Matrix Derivative: Effects on Human Bone Marrow-Derived Stem Cells" Materials 14, no. 24: 7750. https://doi.org/10.3390/ma14247750
APA StyleKim, H. -M., Lee, D., & Kim, S. -Y. (2021). Biocompatibility and Osteogenic Potential of Calcium Silicate-Based Cement Combined with Enamel Matrix Derivative: Effects on Human Bone Marrow-Derived Stem Cells. Materials, 14(24), 7750. https://doi.org/10.3390/ma14247750