

Photobiomodulation in Alzheimer’s Disease—A Complementary Method to State-of-the-Art Pharmaceutical Formulations and Nanomedicine?




Abstract
:1. Introduction
2. Pathophysiological Mechanisms in Alzheimer’s Disease
3. State-of-the-Art Pharmaceutical Formulations and Nanomedicine Applied in Alzheimer’s Disease
3.1. Cholinesterase Inhibitors
3.2. Antagonists of N-Methyl-d-Aspartate Receptors
3.3. Anti-Amyloid Monoclonal Antibodies Used in Alzheimer’s Disease
3.3.1. Aducanumab
3.3.2. Lecanemab
3.4. Side Effects of Drugs Approved for the Therapy of Alzheimer’s Disease
3.5. BBB and Types of Drug Carrier Systems in Alzheimer’s Disease
4. Light and Lasers in Medicine—A Brief Overview
5. Photobiomodulation of the Brain and the Treatment of Alzheimer’s Disease
6. Concluding Remarks and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Acetylcholine | (ACh) |
| Acetylcholinesterase | (AchE) |
| Acetylcholinesterase inhibitor | (AChEI) |
| AD assessment scale-cognitive subscale | (ADAS—cog) |
| Adenosine diphosphate | (ADP) |
| Adenosine triphosphate | (ATP) |
| Advanced Tomo Area Analysis | (ATAA) |
| Alpha (Greek letter, lowercase alpha) | (α) |
| Alzheimer’s Disease | (AD) |
| Alzheimer’s Disease-related dementias | (ADRD) |
| Alzheimer’s Disease Neuroimaging Initiative | (ADNI) |
| Amyloid beta | (Aβ) |
| Amyloid precursor protein | (APP) |
| Amyloid-related imaging abnormalities | (ARIAs) |
| Amyloid-related imaging abnormalities of effusion | (ARIA-E) |
| Amyloid-related imaging abnormalities of hemorrhagic | (ARIA-H) |
| Antibody | (Ab) |
| 3D6 antibody fragments | (3D6-Fab) |
| Antigen presenting cell | (APC) |
| Auditory-immediate verbal learning test 1 | (A.V.L.T.-1) |
| Auditory-immediate verbal learning test 2 | (A.V.L.T.-2) |
| Automated Neuropsychological Assessment Metrics | (ANAM) |
| Aβ oligomers | (AβOs) |
| Beck Anxiety Inventory | (BAI) |
| Beta tubulin III | (Tuj-1) |
| Blood–brain barrier | (BBB) |
| Body mass index | (BMI) |
| Boston Naming Test | (BNT) |
| Brain extracellular space | (ECS) |
| Brain interstitial fluid | (ISF) |
| Brain-derived neurotrophic factor | (BDNF) |
| Broadband near-infrared spectroscopy | (bbNIRS) |
| Butyrylcholinesterase | (BChE) |
| Carboxy-terminal fragment | (CTF) |
| Category Fluency Test | (CFT) |
| CD4+ T lymphocytes | (CD4+) |
| CD8+ T lymphocytes | (CD8+) |
| Central nervous system | (CNS) |
| Cerebral blood flow | (CBF) |
| Cerebrospinal fluid | (CSF) |
| Chinese version of the Dementia Rating Scale | (CDRS) |
| Chinese version of the Geriatric Depression Scale | (CGDS) |
| Chinese version of the Geriatric Depression Scale—Short Form | (CGDS-SF) |
| Cholinesterase | (ChE) |
| Cholinesterase inhibitors | (ChEIs) |
| Clinical Dementia Rating Scale | (CDR) |
| Clinical Global Impressions Improvement subscale | (CGI- I) |
| Clinical Global Impressions-Severity | (CGI-S) |
| Clock copy test | (CPT) |
| Clock drawing test | (CDT) |
| Computed tomography | (CT) |
| Concentration changes of oxidized CCO | (Δ[CCO]) |
| Concentration changes of deoxygenated hemoglobin | (Δ[Hb]) |
| Concentration changes of oxygenated hemoglobin | (Δ[HbO]) |
| Continuous wave | (CW) |
| Continuous tPBM | (c-tPBM) |
| Cyclic adenosine monophosphate | (cAMP) |
| Cytochrome c oxidase | (CCO) |
| Decrease | (↓) |
| Delayed match-to-sample task | (DMS) |
| Deoxyribonucleic acid | (DNA) |
| Diffuse correlation spectroscopy | (DCS) |
| Diffusion rate in ECS-mapping or Diffusion rate in brain extracellular space | (DECS-mapping) |
| Digit span backward | (DSB) |
| Digit span forward | (DSF) |
| Direction of paracellular transport | ↓↓ |
| Donepezil | (DP) |
| Drug delivery | (DD) |
| Drug delivery systems | (DDSs) |
| Electroencephalogram | (EEG) |
| Electron transport chain | (ETC) |
| Erythrocyte | (E) |
| European Medicines Agency | (EMA) |
| Excitatory field potentials/field excitatory postsynaptic potentials | (fEPSPs) |
| Extended release | (ER) |
| Flavin mononucleotide | (FMN) |
| Flavin-adenosine-dinucleotides | (FADs) |
| U.S. Food and Drug Administration | (FDA) |
| Functional Activities Questionnaire | (FAQ) |
| Functional near-infrared spectroscopy | (fNIRS) |
| Galantamine | (GAL) |
| Galantamine nanoparticles | (G-NPs) |
| Generalized anxiety disorder | (GAD) |
| Geriatric Anxiety Scale-10-item Version | (GAS -10) |
| Geriatric Depression Scale | (GDS) |
| Gold nanoparticles | (AuNPs) |
| Granulocyte-macrophage colony stimulating factor | (GM-CSF) |
| Hamilton Anxiety Scale | (SIGH-A) |
| Hamilton Depression Rating Scale | (HDRS-17) |
| Hamilton Depression Rating Scale (modified) | (HAM-D17) |
| Hong Kong List Learning Test | HKLLT |
| Human acetylcholinesterase | (hAChE/huAChE) |
| Hydrogel-loaded NP systems | (NLH) |
| Hydrogen peroxide | (H2O2) |
| Increase | (↑) |
| Insulin-like growth factors-1 | (IGF-1) |
| Interferon-γ | (IFN-γ) |
| Interleukin 1-beta | (IL-1β) |
| IL2 signal sequence | (IL2ss) |
| Interleukin-6 | (IL-6) |
| Interleukin-10 | (IL-10) |
| Janus kinase inhibitor | (JAK) |
| Light Amplification by Stimulated Emission of Radiation | (LASER) |
| Light emitting diode | (LED) |
| Logical Memory Test—Immediate Recall | (LMT-I) |
| Logical Memory Test—Delayed Recall | (LMT-II) |
| Long-term depression | (LTD) |
| Long-term potentiation | (LTP) |
| Lower generation PAMAM and lactoferrin conjugate | (PAMAM-Lf) |
| Low-level laser (or light) therapy | (LLLT) |
| CD4+ T lymphocytes | (CD4+) |
| CD8+ T lymphocytes | (CD8+) |
| Activated or healing macrophage of the M2 type | (M2) |
| Magnetic resonance angiography | (MRA) |
| Magnetic resonance imaging | (MRI) |
| Major depressive disorder | (MDD) |
| Memantine | (MEM) |
| Messenger ribonucleic acid | (m)RNA |
| Methoxy poly(ethylene glycol)-co-poly(ε-caprolactone) | (mPEG-PCL) |
| Microwave Amplification by Stimulated Emission of Radiation | (MASER) |
| Mild cognitive impairment | (MCI) |
| Mini mental state examination | (MMSE) |
| Mitochondria/mitochondrial | mt |
| Mitochondrial membrane potential | (MMP) |
| Modification of the Hamilton Depression Rating) | (HAM-D17) |
| Monoamine oxidase-B | (MAO-B) |
| Monoamine oxygenase | (MAO) |
| Monocyte | (Mo) |
| Montreal Cognitive Assessment Scale | (MoCa—B basic) |
| Morris Water Maze | (MWM) |
| Multi-gated angiography cerebral | (MUGA) |
| Multi-target-directed ligands | (MTDLs) |
| Multi-target-directed ligands | (MTDLs) |
| NAD(P)H quinone oxidoreductase 1 | (NQO1) |
| Nanoemulsion | (NE) |
| Nanoparticle | (NP) |
| Nanostructured lipid carriers | (NLC) |
| Natural Killer cell | (NK cell) |
| Near-infrared | (NIR) |
| Neural Stem Cells | (NSCs) |
| Neurofibrillary structures/tangles | (NFTs) |
| Neuropsychiatric Inventory | (NPI) |
| Nitric oxide | (NO) |
| N-methyl-d-aspartate receptors | (NMDARs) |
| NPs-loaded hydrogel | (NLH) |
| Oligomers Tau | (TauOs) |
| Oxidized CCO | (oxCCO) |
| Oxygenated hemoglobin | (HbO) |
| Paired pulse facilitation | (PPF) |
| Parkinson’s disease | (PD) |
| Phosphorylated tau | (P-tau) |
| Photobiomodulation | (PBM) |
| Transcatheter Intracerebral PBM | (PBMT) |
| Photodynamic inactivation | (PDI) |
| Photodynamic therapy | (PDT) |
| Photoneuromodulation | (PNM) |
| Photosensitizer | (PS) |
| Photothermal therapy | (PTT) |
| Picosecond | (ps) |
| Pittsburgh Sleep Quality Index | (PSQI) |
| Poly(amidoamine) | (PAMAM) |
| Poly(d,l-lactide-co-glycolide) (50:50)-b-poly(ethylene glycol) | [PLGA-b-PEG] |
| Polymorphonuclear neutrophil | (PMN) |
| Positron emission tomography | (PET) |
| Postsynaptic density protein 95 | (PSD-95) |
| Prefrontal cortex | (PFC) |
| Presenilin-1 | (PSEN-1) |
| Presenilin-2 | (PSEN-2) |
| Psychomotor vigilance task | (PVT) |
| Pulsed tPBM | (p-tPBM) |
| Quantitative EEG | (QEEG) |
| Quick Inventory of Depressive Symptomatology-Clinician Rating | (QIDS-C) |
| Reactive oxygen species | (ROS) |
| Red | (R) |
| Red-light treatment | (RLT) |
| Rey–Osterrieth complex figure test | (Rey–O) |
| Rheoencephalography | (REG) |
| Rivastigmine | (RSM) |
| Scanning electron microscopy | (SEM) |
| Scintigraphy | (SG) |
| Self-Administered Gerocognitive Exam | (SAGE) |
| Sham tPBM | (s-tPBM) |
| Signal transducer and activator of transcription 4 | (STAT4) |
| Signal transducer and activator of transcription 5 | (STAT5) |
| Silver nanoparticles | (AgNPs) |
| Single-chain variable fragment | (scFv) |
| Soluble amyloid precursor protein α | (sAPPα) |
| Soluble amyloid precursor protein β | (sAPPβ) |
| Synaptic plasticity | (SP) |
| Tacrine | (TAC) |
| Theta (Greek letter, lowercase theta) | (θ) |
| Tight junction | (TJ) |
| Tomography Dementia Rating | (TDR) |
| Total tau | (T-tau) |
| Transcranial infrared laser stimulation | (TILS) |
| Transcranial light therapy | (TLTC) |
| Transcranial near-infrared | (tNIR) |
| Transcranial PBM | (tPBM) |
| Transcutaneous radial artery PBM | (tc-RA-PBM) |
| Transforming growth factor-β1 | (TGFβ1) |
| Tumor necrosis factor alpha | (TNF-α) |
| Ultraviolet A | (UVA) |
| Ultraviolet B | (UVB) |
| van der Waals | vdW |
| Waist–hip ratio | (WHR) |
| Wild-type | (WT) |
| Wisconsin Card Sorting Test | (WCST) |
| World Health Organization | (WHO) |
References
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Primers. 2021, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.P.; Xie, Y.; Meng, X.Y.; Kang, J.S. History and progress of hypotheses and clinical trials for Alzheimer’s disease. Signal Transduct. Target. Ther. 2019, 4, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barthélemy, N.R.; Li, Y.; Joseph-Mathurin, N.; Gordon, B.A.; Hassenstab, J.; Benzinger, T.L.S.; Buckles, V.; Fagan, A.M.; Perrin, R.J.; Goate, A.M.; et al. Dominantly Inherited Alzheimer Network. A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzheimer’s disease. Nat. Med. 2020, 26, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Busche, M.A.; Hyman, B.T. Synergy between amyloid-β and tau in Alzheimer’s disease. Nat. Neurosci. 2020, 23, 1183–1193. [Google Scholar] [CrossRef]
- The World Health Organization. The Top 10 Causes of Death. 9 December 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 7 December 2022).
- Alzheimer’s Association. 2022 Alzheimer’s Disease Facts and Figures Special Report More Than Normal Aging: Understanding Mild Cognitive Impairmen. 2022 Alzheimer’s Disease Facts and Figures. Alzheimers Dement. 2022, 18, 700–789. Available online: https://www.alz.org/media/documents/alzheimers-facts-and-figures.pdf (accessed on 7 December 2022).
- Karran, E.; De Strooper, B. The amyloid hypothesis in Alzheimer disease: New insights from new therapeutics. Nat. Rev. Drug Discov. 2022, 21, 306–318. [Google Scholar] [CrossRef]
- The World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 7 December 2022).
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef]
- Li, X.; Feng, X.; Sun, X.; Hou, N.; Han, F.; Liu, Y. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2019. Front. Aging Neurosci. 2022, 14, 937486. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Yaari, R.; Fleisher, A.S.; Tariot, P.N. Updates to diagnostic guidelines for Alzheimer’s disease. Prim Care Companion CNS Disord. 2011, 13, 26971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiđemet-Piskač, S.; Babić Leko, M.; Blažeković, A.; Langer Horvat, L.; Klepac, N.; Sonicki, Z.; Kolenc, D.; Hof, P.R.; Boban, M.; Mimica, N.; et al. Evaluation of cerebrospinal fluid phosphorylated tau231 as a biomarker in the differential diagnosis of Alzheimer’s disease and vascular dementia. CNS Neurosci. Ther. 2018, 24, 734–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wattmo, C.; Blennow, K.; Hansson, O. Cerebro-spinal fluid biomarker levels: Phosphorylated tau (T) and total tau (N) as markers for rate of progression in Alzheimer’s disease. BMC Neurol. 2020, 20, 10. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fariat, A.V.; Liang, Z.; Miller, M.I.; Mori, S. Brain MRI pattern recognition translated to clinical scenarios. Front. Neurosci. 2017, 11, 578. [Google Scholar] [CrossRef]
- Mori, S.; Onda, K.; Fujita, S.; Suzuki, T.; Ikeda, M.; Zay Yar Myint, K.; Hikage, J.; Abe, O.; Tomimoto, H.; Oishi, K.; et al. Brain atrophy in middle age using magnetic resonance imaging scans from Japan’s health screening programme. Brain Commun. 2022, 4, fcac211. [Google Scholar] [CrossRef]
- Ju, Y.; Tam, K.Y. Pathological mechanisms and therapeutic strategies for Alzheimer’s disease. Neural Regen. Res. 2022, 17, 543. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019, 57, 87–105. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.V.F.; Loures, C.M.G.; Alves, L.C.V.; de Souza, L.C.; Borges, K.B.G.; Carvalho, M.D.G. Alzheimer’s disease: Risk factors and potentially protective measures. J. Biomed. Sci. 2019, 26, 33. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Lee, V.M.; Hur, S.K. Manipulation of the diet-microbiota-brain axis in Alzheimer’s disease. Front. Neurosci. 2022, 16, 1042865. [Google Scholar] [CrossRef]
- Princiotta Cariddi, L.; Mauri, M.; Cosentino, M.; Versino, M.; Marino, F. Alzheimer’s Disease: From Immune Homeostasis to Neuroinflammatory Condition. Int. J. Mol. Sci. 2022, 23, 13008. [Google Scholar] [CrossRef]
- Bellenguez, C.; Küçükali, F.; Jansen, I.E.; Kleineidam, L.; Moreno-Grau, S.; Amin, N.; Naj, A.C.; Campos-Martin, R.; Grenier-Boley, B.; Andrade, V.; et al. New insights into the genetic etiology of Alzheimer’s disease and related dementias. Nat. Genet. 2022, 54, 412–436. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.S. Amyloid-β and tau: The trigger and bullet in Alzheimer disease pathogenesis. JAMA Neurol. 2014, 71, 505–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovais, M.; Zia, N.; Ahmad, I.; Khalil, A.T.; Raza, A.; Ayaz, M.; Sadiq, A.; Ullah, F.; Shinwari, Z.K. Phyto-Therapeutic and Nanomedicinal Approaches to Cure Alzheimer’s Disease: Present Status and Future Opportunities. Front. Aging Neurosci. 2018, 10, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiwari, S.; Atluri, V.; Kaushik, A.; Yndart, A.; Nair, M. Alzheimer’s disease: Pathogenesis, diagnostics, and therapeutics. Int. J. Nanomed. 2019, 14, 5541–5554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigneswaran, J.; Muthukumar, S.A.; Shafras, M.; Geetika, P. An insight into Alzheimer’s disease and its on-setting novel genes. Egypt J. Neurol. Psychiatry Neurosurg. 2021, 57, 160. [Google Scholar] [CrossRef]
- Abubakar, M.B.; Sanusi, K.O.; Ugusman, A.; Mohamed, W.; Kamal, H.; Ibrahim, N.H.; Khoo, C.S.; Kumar, J. Alzheimer’s Disease: An Update and Insights Into Pathophysiology. Front. Aging Neurosci. 2022, 14, 742408. [Google Scholar] [CrossRef]
- Priller, C.; Bauer, T.; Mitteregger, G.; Krebs, B.; Kretzschmar, H.A.; Herms, J. Synapse formation and function is modulated by the amyloid precursor protein. J. Neurosci. 2006, 26, 7212–7221. [Google Scholar] [CrossRef] [Green Version]
- Marin, M.A.; Ziburkus, J.; Jankowsky, J.; Rasband, M.N. Amyloid-β plaques disrupt axon initial segments. Exp. Neurol. 2016, 281, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos Picanco, L.C.; Ozela, P.F.; de Fatima de Brito Brito, M.; Pinheiro, A.A.; Padilha, E.C.; Braga, F.S.; de Paula da Silva, C.H.T.; Dos Santos, C.B.R.; Rosa, J.M.C.; da Silva Hage-Melim, L.I. Alzheimer’s Disease: A Review from the Pathophysiology to Diagnosis, New Perspectives for Pharmacological Treatment. Curr. Med. Chem. 2018, 25, 3141–3159. [Google Scholar] [CrossRef]
- Butterfield, D.A. Amyloid beta-peptide (1-42)-induced oxidative stress and neurotoxicity: Implications for neurodegeneration in Alzheimer’s disease brain. A review. Free Radic. Res. 2002, 36, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Chow, V.W.; Mattson, M.P.; Wong, P.C.; Gleichmann, M. An overview of APP processing enzymes and products. Neuromol. Med. 2010, 12, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’brien, R.J.; Wong, P.C. Amyloid precursor protein processing and Alzheimer’s disease. Annu. Rev. Neurosci. 2011, 34, 185–204. [Google Scholar] [CrossRef] [Green Version]
- Koss, D.J.; Jones, G.; Cranston, A.; Gardner, H.; Kanaan, N.M.; Platt, B. Soluble pre-fibrillar tau and β-amyloid species emerge in early human Alzheimer’s disease and track disease progression and cognitive decline. Acta Neuropathol. 2016, 132, 875–895. [Google Scholar] [CrossRef] [Green Version]
- Kametani, F.; Hasegawa, M. Reconsideration of amyloid hypothesis and tau hypothesis in Alzheimer’s disease. Front. Neurosci. 2018, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, M.S. Substrate recognition and processing by γ-secretase. Biochim. Biophys. Acta Biomembr. 2020, 1862, 183016. [Google Scholar] [CrossRef]
- Mansor, N.I.; Ntimi, C.M.; Abdul-Aziz, N.M.; Ling, K.H.; Adam, A.; Rosli, R.; Hassan, Z.; Nordin, N. Asymptomatic neurotoxicity of amyloid β-peptides (Aβ1-42 and Aβ25-35) on mouse embryonic stem cell-derived neural cells. Bosn. J. Basic Med. Sci. 2021, 21, 98–110. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.P.; de Castro, A.A.; Soares, F.V.; da Cunha, E.F.F.; Ramalho, T.C. Future Therapeutic Perspectives into the Alzheimer’s Disease Targeting the Oxidative Stress Hypothesis. Molecules 2019, 24, 4410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.D.; Junaid, M.; Shan, X.; Wang, Y.; Wang, X.; Khan, A.; Wei, D.Q. Effect of Cholesterol on C99 Dimerization: Revealed by Molecular Dynamics Simulations. Front. Mol. Biosci. 2022, 9, 872385. [Google Scholar] [CrossRef]
- Chen, X.Q.; Mobley, W.C. Alzheimer Disease Pathogenesis: Insights from Molecular and Cellular Biology Studies of Oligomeric Aβ and Tau Species. Front. Neurosci. 2019, 13, 659. [Google Scholar] [CrossRef]
- Huang, Y.R.; Liu, R.T. The Toxicity and Polymorphism of β-Amyloid Oligomers. Int. J. Mol. Sci. 2020, 21, 4477. [Google Scholar] [CrossRef]
- Michaels, T.C.T.; Šarić, A.; Curk, S.; Bernfur, K.; Arosio, P.; Meisl, G.; Dear, A.J.; Cohen, S.I.A.; Dobson, C.M.; Vendruscolo, M. Dynamics of oligomer populations formed during the aggregation of Alzheimer’s Aβ42 peptide. Nat. Chem. 2020, 12, 445–451, Erratum in Nat Chem. 2020, 12, 497. [Google Scholar] [CrossRef] [PubMed]
- Fontana, I.C.; Zimmer, A.R.; Rocha, A.S.; Gosmann, G.; Souza, D.O.; Lourenco, M.V.; Ferreira, S.T.; Zimmer, E.R. Amyloid-β oligomers in cellular models of Alzheimer’s disease. J. Neurochem. 2020, 155, 348–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mroczko, B.; Groblewska, M.; Litman-Zawadzka, A.; Kornhuber, J.; Lewczuk, P. Cellular Receptors of Amyloid β Oligomers (AβOs) in Alzheimer’s Disease. Int. J. Mol. Sci. 2018, 19, 1884. [Google Scholar] [CrossRef] [Green Version]
- Gotz, J.; Halliday, G.; Nisbet, R.M. Molecular Pathogenesis of the Tauopathies. Annu. Rev. Pathol. 2019, 14, 239–261. [Google Scholar] [CrossRef]
- Penke, B.; Szűcs, M.; Bogár, F. Oligomerization and Conformational Change Turn Monomeric β-Amyloid and Tau Proteins Toxic: Their Role in Alzheimer’s Pathogenesis. Molecules 2020, 25, 1659. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wu, K.M.; Yang, L.; Dong, Q.; Yu, J.T. Tauopathies: New perspectives and challenges. Mol. Neurodegener. 2022, 17, 28. [Google Scholar] [CrossRef]
- Huang, W.J.; Zhang, X.; Chen, W.W. Role of oxidative stress in Alzheimer’s disease. Biomed. Rep. 2016, 4, 519–522. [Google Scholar] [CrossRef] [Green Version]
- Swerdlow, R.H. Mitochondria and mitochondrial cascades in Alzheimer’s disease. J. Alzheimers Dis. 2018, 62, 1403–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, R.Z.; Jiang, S.; Zhang, L.; Yu, Z.B. Mitochondrial electron transport chain, ROS generation and uncoupling (Review). Int. J. Mol. Med. 2019, 44, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Shen, X.; Sun, P.; Zhang, H.; Yang, H. Mitochondrial quality control in the brain: The physiological and pathological roles. Front. Neurosci. 2022, 16, 1075141. [Google Scholar] [CrossRef]
- Cai, Z. Monoamine oxidase inhibitors: Promising therapeutic agents for Alzheimer’s disease (Review). Mol. Med. Rep. 2014, 9, 1533–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzoor, S.; Hoda, N.A. Comprehensive review of monoamine oxidase inhibitors as Anti-Alzheimer’s disease agents: A review. Eur. J. Med. Chem. 2020, 206, 112787. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Kaur, D.; Sehgal, A.; Singh, S.; Sharma, N.; Zengin, G.; Andronie-Cioara, F.L.; Toma, M.M.; Bungau, S.; Bumbu, A.G. Role of Monoamine Oxidase Activity in Alzheimer’s Disease: An Insight into the Therapeutic Potential of Inhibitors. Molecules 2021, 26, 3724. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.S.; Koh, S.H. Neuroinflammation in neurodegenerative disorders: The roles of microglia and astrocytes. Transl. Neurodegener. 2020, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- La Barbera, L.; Mauri, E.; D’Amelio, M.; Gori, M. Functionalization strategies of polymeric nanoparticles for drug delivery in Alzheimer’s disease: Current trends and future perspectives. Front. Neurosci. 2022, 16, 939855. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Deng, M.; Hu, G.; Li, N.; Yuan, H.; Zhou, Y. New Insights into Microglial Mechanisms of Memory Impairment in Alzheimer’s Disease. Biomolecules 2022, 12, 1722. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Wang, H.; Yin, Y. Microglia Polarization From M1 to M2 in Neurodegenerative Diseases. Front. Aging Neurosci. 2022, 14, 815347. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Mesulam, M.M.; Cuello, A.C.; Farlow, M.R.; Giacobini, E.; Grossberg, G.T.; Khachaturian, A.S.; Vergallo, A.; Cavedo, E.; Snyder, P.J.; et al. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain 2018, 141, 1917–1933. [Google Scholar] [CrossRef]
- Chen, X.Q.; Mobley, W.C. Exploring the Pathogenesis of Alzheimer Disease in Basal Forebrain Cholinergic Neurons: Converging Insights from Alternative Hypotheses. Front. Neurosci. 2019, 13, 446. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Kaminga, A.C.; Jia, P.; Wen, S.W.; Acheampong, K.; Liu, A. Catecholamines in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Front. Aging Neurosci. 2020, 12, 184. [Google Scholar] [CrossRef] [PubMed]
- Abduljawad, A.A.; Elawad, M.A.; Elkhalifa, M.E.M.; Ahmed, A.; Hamdoon, A.A.E.; Salim, L.H.M.; Ashraf, M.; Ayaz, M.; Hassan, S.S.U.; Bungau, S. Alzheimer’s Disease as a Major Public Health Concern: Role of Dietary Saponins in Mitigating Neurodegenerative Disorders and Their Underlying Mechanisms. Molecules 2022, 27, 6804. [Google Scholar] [CrossRef] [PubMed]
- Henjum, K.; Watne, L.O.; Godang, K.; Halaas, N.B.; Eldholm, R.S.; Blennow, K.; Zetterberg, H.; Saltvedt, I.; Bollerslev, J.; Knapskog, A.B. Cerebrospinal fluid catecholamines in Alzheimer’s disease patients with and without biological disease. Transl. Psychiatry 2022, 12, 151. [Google Scholar] [CrossRef]
- Wang, R.; Reddy, P.H. Role of glutamate and NMDA receptors in Alzheimer’s disease. J. Alzheimers Dis. 2017, 57, 1041–1048. [Google Scholar] [CrossRef] [Green Version]
- Kodis, E.J.; Choi, S.; Swanson, E.; Ferreira, G.; Bloom, G.S. N-methyl-D-aspartate receptor-mediated calcium influx connects amyloid-β oligomers to ectopic neuronal cell cycle reentry in Alzheimer’s disease. Alzheimers Dement. 2018, 14, 1302–1312. [Google Scholar] [CrossRef]
- Liu, J.; Chang, L.; Song, Y.; Li, H.; Wu, Y. The Role of NMDA Receptors in Alzheimer’s Disease. Front. Neurosci. 2019, 13, 43. [Google Scholar] [CrossRef] [Green Version]
- Bukke, V.N.; Archana, M.; Villani, R.; Romano, A.D.; Wawrzyniak, A.; Balawender, K.; Orkisz, S.; Beggiato, S.; Serviddio, G.; Cassano, T. The Dual Role of Glutamatergic Neurotransmission in Alzheimer’s Disease: From Pathophysiology to Pharmacotherapy. Int. J. Mol. Sci. 2020, 21, 7452. [Google Scholar] [CrossRef]
- Lituma, P.J.; Kwon, H.B.; Alviña, K.; Luján, R.; Castillo, P.E. Presynaptic NMDA receptors facilitate short-term plasticity and BDNF release at hippocampal mossy fiber synapses. eLife 2021, 10, e66612. [Google Scholar] [CrossRef]
- Fish, P.V.; Steadman, D.; Bayle, E.D.; Whiting, P. New Approaches for the Treatment of Alzheimer’s Disease. Bioorg. Med. Chem. Lett. 2019, 29, 125–133. [Google Scholar] [CrossRef]
- Sharma, K. Cholinesterase inhibitors as Alzheimer’s therapeutics (Review). Mol. Med. Rep. 2019, 20, 1479–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stage, E.; Svaldi, D.; Sokolow, S.; Risacher, S.L.; Marosi, K.; Rotter, J.I.; Saykin, A.J.; Apostolova, L.G. Prescribing cholinesterase inhibitors in mild cognitive impairment—Observations from the Alzheimer’s Disease Neuroimaging Initiative. Alzheimers Dement. 2021, 7, e12168. [Google Scholar] [CrossRef] [PubMed]
- F.D.A. Approves New Treatment for Early Alzheimer’s. Available online: https://www.nytimes.com/2023/01/06/health/alzheimers-drug-leqembi-lecanemab.html (accessed on 11 January 2023).
- Rogers, S.L.; Friedhoff, L.T. The efficacy and safety of donepezil in patients with Alzheimer’s disease: Results of a US Multicentre, Randomized, Double-Blind, Placebo-Controlled Trial. The Donepezil Study Group. Dementia 1996, 7, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.; Fox, N. Defining Disease Modifying Therapy for Alzheimer’s Disease. J. Prev. Alzheimer’s Dis. 2017, 4, 109. [Google Scholar] [CrossRef]
- Nguyen, K.; Hoffman, H.; Chakkamparambil, B.; Grossberg, G.T. Evaluation of rivastigmine in Alzheimer’s disease. Neurodegener. Dis. Manag. 2021, 11, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.; Rawashdeh, O.; Kasas, L.; Milne, M.R.; Garner, N.; Sankorrakul, K.; Marks, N.; Dean, M.W.; Kim, P.R.; Sharma, A.; et al. Cholinergic basal forebrain degeneration due to sleep-disordered breathing exacerbates pathology in a mouse model of Alzheimer’s disease. Nat. Commun. 2022, 13, 6543. [Google Scholar] [CrossRef]
- Noetzli, M.; Eap, C.B. Pharmacodynamic, pharmacokinetic and pharmacogenetic aspects of drugs used in the treatment of Alzheimer’s disease. Clin. Pharmacokinet. 2013, 52, 225–241. [Google Scholar] [CrossRef]
- Marucci, G.; Buccioni, M.; Ben, D.D.; Lambertucci, C.; Volpini, R.; Amenta, F. Efficacy of acetylcholinesterase inhibitors in Alzheimer’s disease. Neuropharmacology 2021, 190, 108352. [Google Scholar] [CrossRef]
- León, R.; Garcia, A.G.; Marco-Contelles, J. Recent advances in the multitarget-directed ligands approach for the treatment of Alzheimer’s disease. Med. Res. Rev. 2013, 33, 139–189. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.; Kaur, M.; Chadha, N.; Silakari, O. Hybrids: A new paradigm to treat Alzheimer’s disease. Mol. Divers. 2016, 20, 271–297. [Google Scholar] [CrossRef]
- Mishra, P.; Kumar, A.; Panda, G. Anti-cholinesterase hybrids as multi-target-directed ligands against Alzheimer’s disease (1998–2018). Bioorg. Med. Chem. 2019, 27, 895–930. [Google Scholar] [CrossRef]
- Jana, A.; Bhattacharjee, A.; Das, S.S.; Srivastava, A.; Choudhury, A.; Bhattacharjee, R.; De, S.; Perveen, A.; Iqbal, D.; Gupta, P.K.; et al. Molecular Insights into Therapeutic Potentials of Hybrid Compounds Targeting Alzheimer’s Disease. Mol. Neurobiol. 2022, 59, 3512–3528. [Google Scholar] [CrossRef] [PubMed]
- Mao, F.; Li, J.; Wei, H.; Huang, L.; Li, X. Tacrine-propargylamine derivatives with improved acetylcholinesterase inhibitory activity and lower hepatotoxicity as a potential lead compound for the treatment of Alzheimer’s disease. J. Enzym. Inhib. Med. Chem. 2015, 30, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zenger, K.; Lupp, A.; Kling, B.; Heilmann, J.; Fleck, C.; Kraus, B.; Decker, M. Tacrine-silibinin codrug shows neuro- and hepatoprotective effects in vitro and pro-cognitive and hepatoprotective effects in vivo. J. Med. Chem. 2012, 55, 5231–5242. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Zhao, L.Z.; Zhao, H.T.; Huang, S.L.; Zhong, S.M.; Qin, J.K.; Chen, Z.F.; Huang, Z.S.; Liang, H. Hybrids of oxoisoaporphine-tacrine congeners: Novel acetylcholinesterase and acetylcholinesterase induced β-amyloid aggregation inhibitors. Eur. J. Med. Chem. 2011, 46, 4970–4979. [Google Scholar] [CrossRef]
- Milelli, A.; De Simone, A.; Ticchi, N.; Chen, H.H.; Betari, N.; Andrisano, V.; Tumiatti, V. Tacrine-based Multifunctional Agents in Alzheimer’s Disease: An Old Story in Continuous Development§. Curr. Med. Chem. 2017, 24, 3522–3546. [Google Scholar] [CrossRef]
- Przybyłowska, M.; Kowalski, S.; Dzierzbicka, K.; Inkielewicz-Stepniak, I. Therapeutic Potential of Multifunctional Tacrine Analogues. Curr. Neuropharmacol. 2019, 17, 472–490. [Google Scholar] [CrossRef]
- Cheong, S.L.; Tiew, J.K.; Fong, Y.H.; Leong, H.W.; Chan, Y.M.; Chan, Z.L.; Kong, E.W.J. Current Pharmacotherapy and Multi-Target Approaches for Alzheimer’s Disease. Pharmaceuticals 2022, 15, 1560. [Google Scholar] [CrossRef]
- Arce, M.P.; Rodríguez-Franco, M.I.; González-Muñoz, G.C.; Pérez, C.; López, B.; Villarroya, M.; López, M.G.; García, A.G.; Conde, S. Neuroprotective and cholinergic properties of multifunctional glutamic acid derivatives for the treatment of Alzheimer’s disease. J. Med. Chem. 2009, 52, 7249–7257. [Google Scholar] [CrossRef]
- Piemontese, L.; Tomás, D.; Hiremathad, A.; Capriati, V.; Candeias, E.; Cardoso, S.M.; Chavest, S.; Santos, M.A. Donepezil structure-based hybrids as potential multifunctional anti-Alzheimer’s drug candidates. J. Enzym. Inhib. Med. Chem. 2018, 33, 1212–1224. [Google Scholar] [CrossRef] [Green Version]
- Saeedi, M.; Felegari, P.; Iraji, A.; Hariri, R.; Rastegari, A.; Mirfazli, S.S.; Edraki, N.; Firuzi, O.; Mahdavi, M.; Akbarzadeh, T. Novel N-benzylpiperidine derivatives of 5-arylisoxazole-3-carboxamides as anti-Alzheimer’s agents. Arch. Pharm. 2021, 354, 2000258. [Google Scholar] [CrossRef]
- Xiao, G.; Li, Y.; Qiang, X.; Xu, R.; Zheng, Y.; Cao, Z.; Luo, L.; Yang, X.; Sang, Z.; Su, F.; et al. Design, synthesis and biological evaluation of 4’-aminochalcone-rivastigmine hybrids as multifunctional agents for the treatment of Alzheimer’s disease. Bioorg. Med. Chem. 2017, 25, 1030–1041. [Google Scholar] [CrossRef]
- Sang, Z.; Wang, K.; Shi, J.; Cheng, X.; Zhu, G.; Wei, R.; Ma, Q.; Yu, L.; Zhao, Y.; Tan, Z.; et al. Apigenin-rivastigmine hybrids as multi-target-directed liagnds for the treatment of Alzheimer’s disease. Eur. J. Med. Chem. 2020, 187, 111958. [Google Scholar] [CrossRef]
- Vicente-Zurdo, D.; Rosales-Conrado, N.; León-González, M.E.; Brunetti, L.; Piemontese, L.; Pereira-Santos, A.R.; Cardoso, S.M.; Madrid, Y.; Chaves, S.; Santos, M.A. Novel Rivastigmine Derivatives as Promising Multi-Target Compounds for Potential Treatment of Alzheimer’s Disease. Biomedicines 2022, 10, 1510. [Google Scholar] [CrossRef]
- Stavrakov, G.; Philipova, I.; Lukarski, A.; Atanasova, M.; Zheleva, D.; Zhivkova, Z.D.; Ivanov, S.; Atanasova, T.; Konstantinov, S.; Doytchinova, I. Galantamine-Curcumin Hybrids as Dual-Site Binding Acetylcholinesterase Inhibitors. Molecules 2020, 25, 3341. [Google Scholar] [CrossRef] [PubMed]
- Lazarova, M.I.; Tsekova, D.S.; Tancheva, L.P.; Kirilov, K.T.; Uzunova, D.N.; Vezenkov, L.T.; Tsvetanova, E.R.; Alexandrova, A.V.; Georgieva, A.P.; Gavrilova, P.T.; et al. New Galantamine Derivatives with Inhibitory Effect on Acetylcholinesterase Activity. J. Alzheimers Dis. 2021, 83, 1211–1220. [Google Scholar] [CrossRef]
- Mladenova, K.; Stavrakov, G.; Philipova, I.; Atanasova, M.; Petrova, S.; Doumanov, J.; Doytchinova, I. A Galantamine-Curcumin Hybrid Decreases the Cytotoxicity of Amyloid-Beta Peptide on SH-SY5Y Cells. Int. J. Mol. Sci. 2021, 22, 7592. [Google Scholar] [CrossRef]
- Jiang, N.; Ding, J.; Liu, J.; Sun, X.; Zhang, Z.; Mo, Z.; Li, X.; Yin, H.; Tang, W.; Xie, S.S. Novel chromanone-dithiocarbamate hybrids as multifunctional AChE inhibitors with β-amyloid anti-aggregation properties for the treatment of Alzheimer’s disease. Bioorg. Chem. 2019, 89, 103027. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Xu, A.; Cheng, M.; Wan, Y.; Wang, R.; Fang, Y.; Jin, Y.; Xie, S.S.; Liu, J. Design, Synthesis and Biological Evaluation of New 3,4-Dihydro-2(1H)-Quinolinone-Dithiocarbamate Derivatives as Multifunctional Agents for the Treatment of Alzheimer’s Disease. Drug Des. Dev. Ther. 2022, 16, 1495–1514. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Z.J.; Bian, H.L.; Wang, J.W.; Shan, W.G. Synthesis of physostigmine analogues and evaluation of their anticholinesterase activities. Bioorg. Med. Chem. Lett. 2010, 20, 1532–1534. [Google Scholar] [CrossRef]
- Vecchio, I.; Sorrentino, L.; Paoletti, A.; Marra, R.; Arbitrio, M. The State of The Art on Acetylcholinesterase Inhibitors in the Treatment of Alzheimer’s Disease. J. Cent. Nerv. Syst. Dis. 2021, 13, 1795735211029113. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, C.; Yang, W. Role of berberine in Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2016, 12, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Singh, S.K.; Nandi, M.K.; Mishra, G.; Maurya, A.; Rai, A.; Rai, G.K.; Awasthi, R.; Sharma, B.; Kulkarni, G.T. Berberine: A Plant-derived Alkaloid with Therapeutic Potential to Combat Alzheimer’s disease. Cent. Nerv. Syst. Agents Med. Chem. 2019, 19, 154–170. [Google Scholar] [CrossRef]
- Choi, E.Y.; Kang, S.S.; Lee, S.K.; Han, B.H. Polyphenolic Biflavonoids Inhibit Amyloid-Beta Fibrillation and Disaggregate Preformed Amyloid-Beta Fibrils. Biomol. Ther. 2020, 28, 145–151. [Google Scholar] [CrossRef]
- Windsor, P.K.; Plassmeyer, S.P.; Mattock, D.S.; Bradfield, J.C.; Choi, E.Y.; Miller, B.R., 3rd; Han, B.H. Biflavonoid-Induced Disruption of Hydrogen Bonds Leads to Amyloid-β Disaggregation. Int. J. Mol. Sci. 2021, 22, 2888. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Chen, Q.; Wen, B.; Wu, N.; He, B.; Chen, J. Berberine Reduces Aβ42 Deposition and Tau Hyperphosphorylation via Ameliorating Endoplasmic Reticulum Stress. Front. Pharmacol. 2021, 12, 640758. [Google Scholar] [CrossRef] [PubMed]
- Han, B.H.; Cofell, B.; Everhart, E.; Humpal, C.; Kang, S.S.; Lee, S.K.; Kim-Han, J.S. Amentoflavone Promotes Cellular Uptake and Degradation of Amyloid-Beta in Neuronal Cells. Int. J. Mol. Sci. 2022, 23, 5885. [Google Scholar] [CrossRef] [PubMed]
- Pallo, S.P.; DiMaio, J.; Cook, A.; Nilsson, B.; Johnson, G.V.W. Mechanisms of tau and Aβ-induced excitotoxicity. Brain Res. 2016, 1634, 119–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Li, P.; Feng, J.; Wu, M. Dysfunction of NMDA receptors in Alzheimer’s disease. Neurol. Sci. 2016, 37, 1039–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoicas, I.; Kornhuber, J. The Role of Metabotropic Glutamate Receptors in Social Behavior in Rodents. Int. J. Mol. Sci. 2019, 20, 1412. [Google Scholar] [CrossRef] [Green Version]
- Atri, A. Current and Future Treatments in Alzheimer’s Disease. Semin. Neurol. 2019, 39, 227–240. [Google Scholar] [CrossRef]
- Grossberg, G.T.; Manes, F.; Allegri, R.F.; Gutiérrez-Robledo, L.M.; Gloger, S.; Xie, L.; Jia, X.D.; Pejović, V.; Miller, M.L.; Perhach, J.L.; et al. The safety, tolerability, and efficacy of once-daily memantine (28 mg): A multinational, randomized, double-blind, placebo-controlled trial in patients with moderate-to-severe Alzheimer’s disease taking cholinesterase inhibitors. CNS Drugs. 2013, 27, 469–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauthier, S.; Molinuevo, J.L. Benefits of combined cholinesterase inhibitor and memantine treatment in moderate-severe Alzheimer’s disease. Alzheimers Dement. 2013, 9, 326–331. [Google Scholar] [CrossRef]
- Grossberg, G.T.; Alva, G.; Hendrix, S.; Ellison, N.; Kane, M.C.; Edwards, J. Memantine ER Maintains Patient Response in Moderate to Severe Alzheimer’s Disease: Post Hoc Analyses From a Randomized, Controlled, Clinical Trial of Patients Treated With Cholinesterase Inhibitors. Alzheimer Dis. Assoc. Disord. 2018, 32, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, Z.; Liu, R.; Huang, Y.; Zhang, N.; Zhang, R. Memantine, Donepezil, or Combination Therapy-What is the best therapy for Alzheimer’s Disease? A Network Meta-Analysis. Brain Behav. 2020, 10, e01831. [Google Scholar] [CrossRef] [PubMed]
- Owen, R.T. Memantine and donepezil: A fixed drug combination for the treatment of moderate to severe Alzheimer’s dementia. Drugs Today 2016, 52, 239–248. [Google Scholar] [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. A fixed-dose combination of memantine extended-release and donepezil in the treatment of moderate-to-severe Alzheimer’s disease. Drug Des. Dev. Ther. 2016, 10, 3267–3279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calhoun, A.; King, C.; Khoury, R.; Grossberg, G.T. An evaluation of memantine ER + donepezil for the treatment of Alzheimer’s disease. Expert. Opin. Pharmacother. 2018, 19, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Pardo-Moreno, T.; González-Acedo, A.; Rivas-Domínguez, A.; García-Morales, V.; García-Cozar, F.J.; Ramos-Rodríguez, J.J.; Melguizo-Rodríguez, L. Therapeutic Approach to Alzheimer’s Disease: Current Treatments and New Perspectives. Pharmaceutics 2022, 14, 1117. [Google Scholar] [CrossRef]
- Salloway, S.; Chalkias, S.; Barkhof, F.; Burkett, P.; Barakos, J.; Purcell, D.; Suhy, J.; Forrestal, F.; Tian, Y.; Umans, K.; et al. Amyloid-Related Imaging Abnormalities in 2 Phase 3 Studies Evaluating Aducanumab in Patients with Early Alzheimer Disease. JAMA Neurol. 2022, 79, 13–21. [Google Scholar] [CrossRef]
- Budd Haeberlein, S.; Aisen, P.S.; Barkhof, F.; Chalkias, S.; Chen, T.; Cohen, S.; Dent, G.; Hansson, O.; Harrison, K.; von Hehn, C.; et al. Two Randomized Phase 3 Studies of Aducanumab in Early Alzheimer’s Disease. J. Prev. Alzheimers Dis. 2022, 9, 197–210. [Google Scholar] [CrossRef]
- Vaz, M.; Silvestre, S. Alzheimer’s disease: Recent treatment strategies. Eur. J. Pharmacol. 2020, 887, 173554. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Banerjee, D. A Primer on the Evolution of Aducanumab: The First Antibody Approved for Treatment of Alzheimer’s Disease. J. Alzheimers Dis. 2021, 83, 1537–1552. [Google Scholar] [CrossRef]
- Nisticò, R.; Borg, J.J. Aducanumab for Alzheimer’s disease: A regulatory perspective. Pharmacol. Res. 2021, 171, 105754. [Google Scholar] [CrossRef]
- Vaz, M.; Silva, V.; Monteiro, C.; Silvestre, S. Role of Aducanumab in the Treatment of Alzheimer’s Disease: Challenges and Opportunities. Clin. Interv. Aging 2022, 17, 797–810. [Google Scholar] [CrossRef]
- Selkoe, D.J. Alzheimer disease and aducanumab: Adjusting our approach. Nat. Rev. Neurol. 2019, 15, 365–366. [Google Scholar] [CrossRef]
- Høilund-Carlsen, P.F.; Werner, T.J.; Alavi, A.; Revheim, M.E. Aducanumab-Related Amyloid-Related Imaging Abnormalities: Paean or Lament? Clin. Nucl. Med. 2022, 47, 625–626. [Google Scholar] [CrossRef]
- Wassef, H.R.; Colletti, P.M. Commentary: Aducanumab-Related ARIA: Paean or Lament? Clin. Nucl. Med. 2022, 47, 707–709. [Google Scholar] [CrossRef]
- Muralidharan, K.K.; Karumanchi, S.; Kowalski, K.G.; Burkett, P.; Chapel, S.; Rajagovindan, R.; Nestorov, I. A Time-to-Event Exposure-Response Model for Amyloid-Related Imaging Abnormalities Following Administration of Aducanumab to Subjects With Early Alzheimer Disease. J Clin Pharmacol. 2022, 62, 1030–1046. [Google Scholar] [CrossRef]
- Esang, M.; Gupta, M. Aducanumab as a Novel Treatment for Alzheimer’s Disease: A Decade of Hope, Controversies, and the Future. Cureus 2021, 13, e17591. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Ferrucci, L.; Kapogiannis, D. Effects of monoclonal antibodies against amyloid-β on clinical and biomarker outcomes and adverse event risks: A systematic review and meta-analysis of phase III RCTs in Alzheimer’s disease. Ageing Res. Rev. 2021, 68, 101339. [Google Scholar] [CrossRef]
- Tampi, R.R.; Forester, B.P.; Agronin, M. Aducanumab: Evidence from clinical trial data and controversies. Drugs Context. 2021, 10, 2021-7-3. [Google Scholar] [CrossRef]
- Haddad, H.W.; Malone, G.W.; Comardelle, N.J.; Degueure, A.E.; Poliwoda, S.; Kaye, R.J.; Murnane, K.S.; Kaye, A.M.; Kaye, A.D. Aduhelm, a novel anti-amyloid monoclonal antibody, for the treatment of Alzheimer’s Disease: A comprehensive review. Health Psychol. Res. 2022, 10, 37023. [Google Scholar] [CrossRef]
- Silvestro, S.; Valeri, A.; Mazzon, E. Aducanumab and Its Effects on Tau Pathology: Is This the Turning Point of Amyloid Hypothesis? Int. J. Mol. Sci. 2022, 23, 2011. [Google Scholar] [CrossRef]
- Singh, S.; Yang, F.; Sivils, A.; Cegielski, V.; Chu, X.P. Amylin and Secretases in the Pathology and Treatment of Alzheimer’s Disease. Biomolecules 2022, 12, 996. [Google Scholar] [CrossRef]
- Alzforum Networking for a Cure. Therapeutics. Leqembi. Available online: https://www.alzforum.org/therapeutics/leqembi (accessed on 11 January 2023).
- McDade, E.; Cummingsy, J.L.; Dhadda, S.; Swanson, C.J.; Reyderman, L.; Kanekiyo, M.; Koyama, A.; Irizarry, M.; Kramer, L.D.; Bateman, R.J. Lecanemab in patients with early Alzheimer’s disease: Detailed results on biomarker, cognitive, and clinical effects from the randomized and open-label extension of the phase 2 proof-of-concept study. Alzheimers Res. Ther. 2022, 14, 191. [Google Scholar] [CrossRef]
- Reardon, S. FDA approves Alzheimer’s drug lecanemab amid safety concerns. Nature 2023, 613, 227–228. [Google Scholar] [CrossRef]
- Tucker, S.; Möller, C.; Tegerstedt, K.; Lord, A.; Laudon, H.; Sjödahl, J.; Söderberg, L.; Spens, E.; Sahlin, C.; Waara, E.R.; et al. The murine version of BAN2401 (mAb158) selectively reduces amyloid-β protofibrils in brain and cerebrospinal fluid of tg-ArcSwe mice. J. Alzheimers Dis. 2015, 43, 575–588. [Google Scholar] [CrossRef]
- Söllvander, S.; Nikitidou, E.; Gallasch, L.; Zyśk, M.; Söderberg, L.; Sehlin, D.; Lannfelt, L.; Erlandsson, A. The Aβ protofibril selective antibody mAb158 prevents accumulation of Aβ in astrocytes and rescues neurons from Aβ-induced cell death. J. Neuroinflamm. 2018, 15, 98. [Google Scholar] [CrossRef]
- Alzforum Networking for a Cure. Finally: Big Win on All Outcomes for Lecanemab in Phase 3 Topline Results. Available online: https://www.alzforum.org/news/research-news/finally-big-win-all-outcomes-lecanemab-phase-3-topline-results (accessed on 11 January 2023).
- Alzforum Networking for a Cure. Should People on Blood Thinners Forego Leqembi? Available online: https://www.alzforum.org/news/research-news/should-people-blood-thinners-forego-leqembi (accessed on 11 January 2023).
- Swanson, C.J.; Zhang, Y.; Dhadda, S.; Wang, J.; Kaplow, J.; Lai, R.Y.K.; Lannfelt, L.; Bradley, H.; Rabe, M.; Koyama, A.; et al. A randomized, double-blind, phase 2b proof-of-concept clinical trial in early Alzheimer’s disease with lecanemab, an anti-Aβ protofibril antibody. Alzheimers Res. Therapy 2021, 13, 80, Erratum in Alzheimers Res. Ther. 2022, 14, 70. [Google Scholar] [CrossRef]
- Dhadda, S.; Kanekiyo, M.; Li, D.; Swanson, C.J.; Irizarry, M.; Berry, S.; Kramer, L.D.; Berry, D.A. (2022). Consistency of efficacy results across various clinical measures and statistical methods in the lecanemab phase 2 trial of early Alzheimer’s disease. Alzheimers Res. Ther. 2022, 14, 182. [Google Scholar] [CrossRef]
- Pereverzev, A.P.; Ostroumova, O.D.; Tkacheva, O.N.; Kotovskaya, Y.V. Safety of Cholinesterase Inhibitors and NMDA Receptors Antagonists for the Treatment of Patients with Dementia. Saf. Risk Pharmacother. 2019, 7, 190–199. (In Russian) [Google Scholar] [CrossRef]
- Colović, M.B.; Krstić, D.Z.; Lazarević-Pašti, T.D.; Bondžić, A.M.; Vasić, V.M. Acetylcholinesterase inhibitors: Pharmacology and toxicology. Curr. Neuropharmacol. 2013, 11, 315–335. [Google Scholar] [CrossRef] [Green Version]
- Ruangritchankul, S.; Chantharit, P.; Srisuma, S.; Gray, L.C. Adverse Drug Reactions of Acetylcholinesterase Inhibitors in Older People Living with Dementia: A Comprehensive Literature Review. Ther. Clin. Risk Manag. 2021, 17, 927–949. [Google Scholar] [CrossRef]
- Young, S.; Chung, E.; Chen, M.A. Cardiovascular Complications of Acetylcholinesterase Inhibitors in Patients with Alzheimer’s Disease: A Narrative Review. Ann. Geriatr. Med. Res. 2021, 25, 170–177. [Google Scholar] [CrossRef]
- Jones, R.W. A review comparing the safety and tolerability of memantine with the acetylcholinesterase inhibitors. Int. J. Geriatr. Psychiatry 2010, 25, 547–553. [Google Scholar] [CrossRef]
- Shi, X.; Lin, X.; Hu, R.; Sun, N.; Hao, J.; Gao, C. Toxicological Differences between NMDA Receptor Antagonists and Cholinesterase Inhibitors. Am. J. Alzheimers Dis. Other Demen. 2016, 31, 405–412. [Google Scholar] [CrossRef]
- Blanco-Silvente, L.; Capellà, D.; Garre-Olmo, J.; Vilalta-Franch, J.; Castells, X. Predictors of discontinuation, efficacy, and safety of memantine treatment for Alzheimer’s disease: Meta-analysis and meta-regression of 18 randomized clinical trials involving 5004 patients. BMC Geriatr. 2018, 18, 168. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, T.R.; Lopes, L.C.; Bergamaschi, C.C. Frequency and Severity of Adverse Drug Reactions to Medications Prescribed for Alzheimer’s Disease in a Brazilian City: Cross-Sectional Study. Front. Pharmacol. 2020, 11, 538095. [Google Scholar] [CrossRef]
- Barenholtz Levy, H. Accelerated Approval of Aducanumab: Where Do We Stand Now? Ann. Pharmacother. 2022, 56, 736–739. [Google Scholar] [CrossRef]
- Ebell, M.H.; Barry, H.C. Why Physicians Should Not Prescribe Aducanumab for Alzheimer Disease. Am. Fam. Physician 2022, 105, 353–354. Available online: https://www.aafp.org/pubs/afp/issues/2022/0400/p353.html (accessed on 26 February 2023).
- Filippi, M.; Cecchetti, G.; Spinelli, E.G.; Vezzulli, P.; Falini, A.; Agosta, F. Amyloid-Related Imaging Abnormalities and β-Amyloid–Targeting Antibodies: A Systematic Review. JAMA Neurol. 2022, 79, 291–304. [Google Scholar] [CrossRef]
- Chin, E.; Jaqua, E.; Safaeipour, M.; Ladue, T. Conventional Versus New Treatment: Comparing the Effects of Acetylcholinesterase Inhibitors and N-Methyl-D-Aspartate Receptor Antagonist with Aducanumab. Cureus 2022, 14, e31065. [Google Scholar] [CrossRef]
- van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 388, 9–21. [Google Scholar] [CrossRef] [PubMed]
- FDA Grants Accelerated Approval for Alzheimer’s Disease Treatment. Available online: https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-disease-treatment (accessed on 11 January 2023).
- Kroger, E.; Mouls, M.; Wilchesky, M.; Berkers, M.; Carmichael, P.H.; van Marum, R.; Souverein, P.; Egberts, T.; Laroche, M.L. Adverse drug reactions reported with cholinesterase inhibitors: An analysis of 16 years of individual case safety reports from VigiBase. Ann. Pharmacother. 2015, 49, 1197–1206. [Google Scholar] [CrossRef]
- Tariot, P.N.; Braeckman, R.; Oh, C. Comparison of Steady-State Pharmacokinetics of Donepezil Transdermal Delivery System with Oral Donepezil. J. Alzheimers Dis. 2022, 90, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Aricept Side Effects. Drugs.com. Available online: https://www.drugs.com/sfx/aricept-side-effects.html (accessed on 4 January 2023).
- Donepezil Prescribing Information. Drugs.com. Available online: https://www.drugs.com/pro/donepezil.html (accessed on 26 February 2023).
- Corium Launches ADLARITY® (Donepezil Transdermal System) for Patients with Alzheimer’s Dementia. Available online: https://www.prnewswire.com/news-releases/corium-launches-adlarity-donepezil-transdermal-system-for-patients-with-alzheimers-dementia-301636317.html (accessed on 4 January 2023).
- Khoury, R.; Rajamanickam, J.; Grossberg, G.T. An update on the safety of current therapies for Alzheimer’s disease: Focus on rivastigmine. Ther. Adv. Drug Saf. 2018, 9, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Haake, A.; Nguyen, K.; Friedman, L.; Chakkamparambil, B.; Grossberg, G.T. An update on the utility and safety of cholinesterase inhibitors for the treatment of Alzheimer’s disease. Expert Opin. Drug Saf. 2020, 19, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Schurad, B.; Koch, C.; Schug, B.; Morte, A.; Vaqué, A.; De la Torre, R.; Iniesta, M. Comparative Bioavailability Study of a Novel Multi-Day Patch Formulation of Rivastigmine (Twice Weekly) with Exelon® Transdermal Patch (Daily)—A Randomized Clinical Trial. Curr. Alzheimer Res. 2022, 19, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Morte, A.; Vaqué, A.; Iniesta, M.; Schug, B.; Koch, C.; De la Torre, R.; Schurad, B. Bioavailability Study of a Transdermal Patch Formulation of Rivastigmine Compared with Exelon in Healthy Subjects. Eur. J. Drug Metab. Pharmacokinet. 2022, 47, 567–578. [Google Scholar] [CrossRef]
- Rivastigmine Prescribing Information. Drugs.com. Available online: https://www.drugs.com/pro/rivastigmine.html (accessed on 26 February 2023).
- Yang, Z.Z.; Zhang, Y.Q.; Wang, Z.Z.; Wu, K.; Lou, J.N.; Qi, X.R. Enhanced brain distribution and pharmacodynamics of rivastigmine by liposomes following intranasal administration. Int. J. Pharm. 2013, 452, 344–354. [Google Scholar] [CrossRef]
- Rompicherla, S.K.L.; Arumugam, K.; Bojja, S.L.; Kumar, N.; Rao, C.M. Pharmacokinetic and pharmacodynamic evaluation of nasal liposome and nanoparticle based rivastigmine formulations in acute and chronic models of Alzheimer’s disease. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2021, 394, 1737–1755. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Almalki, W.H.; Afzal, O.; Panda, S.K.; Kazmi, I.; Alrobaian, M.; Katouah, H.A.; Altamimi, A.S.A.; Al-Abbasi, F.A.; Alshehri, S.; et al. Systematic development of lectin conjugated microspheres for nose-to-brain delivery of rivastigmine for the treatment of Alzheimer’s disease. Biomed. Pharmacother. 2021, 141, 11829. [Google Scholar] [CrossRef] [PubMed]
- Cunha, S.; Swedrowska, M.; Bellahnid, Y.; Xu, Z.; Sousa Lobo, J.M.; Forbes, B.; Silva, A.C. Thermosensitive in situ hydrogels of rivastigmine-loaded lipid-based nanosystems for nose-to-brain delivery: Characterisation, biocompatibility, and drug deposition studies. Int. J. Pharm. 2022, 620, 121720. [Google Scholar] [CrossRef] [PubMed]
- Salimi, A.; Gobadian, H.; Sharif Makhmalzadeh, B. Dermal pharmacokinetics of rivastigmine-loaded liposomes: An ex vivo-in vivo correlation study. J. Liposome Res. 2021, 31, 246–254. [Google Scholar] [CrossRef]
- Mohamadpour, H.; Azadi, A.; Rostamizadeh, K.; Andalib, S.; Saghatchi Zanjani, M.R.; Hamidi, M. Preparation, Optimization, and Evaluation of Methoxy Poly (ethylene glycol)-co-Poly(ε-caprolactone) Nanoparticles Loaded by Rivastigmine for Brain Delivery. ACS Chem. Neurosci. 2020, 11, 783–795. [Google Scholar] [CrossRef]
- Cacabelos, R. Pharmacogenetic considerations when prescribing cholinesterase inhibitors for the treatment of Alzheimer’s disease. Expert Opin. Drug Metab. Toxicol. 2020, 16, 673–701. [Google Scholar] [CrossRef]
- Takeda, M.; Tanaka, T.; Okochi, M. Editorial: New drugs for Alzheimer’s disease in Japan. Psychiatry Clin. Neurosci. 2011, 65, 399–404. [Google Scholar] [CrossRef]
- Razadyne. Drugs.com. Available online: https://www.drugs.com/mtm/razadyne.html (accessed on 24 January 2023).
- Sunena Singh, S.K.; Mishra, D.N. Nose to Brain Delivery of Galantamine Loaded Nanoparticles: In-vivo Pharmacodynamic and Biochemical Study in Mice. Curr.Drug Deliv. 2019, 16, 51–58. [Google Scholar] [CrossRef]
- El-Ganainy, S.O.; Gowayed, M.A.; Agami, M.; Mohamed, P.; Belal, M.; Farid, R.M.; Hanafy, A.S. Galantamine nanoparticles outperform oral galantamine in an Alzheimer’s rat model: Pharmacokinetics and pharmacodynamics. Nanomedicine 2021, 16, 1281–1296. [Google Scholar] [CrossRef]
- Dou, K.X.; Tan, M.S.; Tan, C.C.; Cao, X.P.; Hou, X.H.; Guo, Q.H.; Tan, L.; Mok, V.; Yu, J.T. Comparative safety and effectiveness of cholinesterase inhibitors and memantine for Alzheimer’s disease: A network meta-analysis of 41 randomized controlled trials. Alzheimers Res. Ther. 2018, 10, 126. [Google Scholar] [CrossRef] [Green Version]
- McShane, R.; Westby, M.J.; Roberts, E.; Minakaran, N.; Schneider, L.; Farrimond, L.E.; Maayan, N.; Ware, J.; Debarros, J. Memantine for dementia. Cochrane Database Syst. Rev. 2019, 3, CD003154. [Google Scholar] [CrossRef]
- Schneider, L.S.; Dagerman, K.S.; Higgins, J.P.; McShane, R. Lack of evidence for the efficacy of memantine in mild Alzheimer disease. Arch. Neurol. 2011, 68, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Namzaric FDA Approval History. Drugs.com. Available online: https://www.drugs.com/history/namzaric.html# (accessed on 26 February 2023).
- U.S. Food and Drug Administration. Drug Approval Package: Aduhelm (Aducanumab-Avwa). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/761178Orig1s000TOC.cfm (accessed on 5 January 2023).
- Nunes, D.; Loureiro, J.A.; Pereira, M.C. Drug Delivery Systems as a Strategy to Improve the Efficacy of FDA-Approved Alzheimer’s Drugs. Pharmaceutics 2022, 14, 2296. [Google Scholar] [CrossRef] [PubMed]
- Lecanemab Confirmatory Phase 3 Clarity Ad Study Met Primary Endpoint, Showing Highly Statistically Significant Reduction of Clinical Decline in Large Global Clinical Study of 1795 Paticipants with Erly Alzheimer’s Disase. Eisai and Biogen. 28 September 2022. Available online: https://www.eisai.com/news/2022/news202271.html (accessed on 18 January 2023).
- Abbott, N.J.; Patabendige, A.A.; Dolman, D.E.; Yusof, S.R.; Begley, D.J. Structure and function of the blood-brain barrier. Neurobiol. Dis. 2010, 37, 13–25. [Google Scholar] [CrossRef]
- Tumani, H.; Huss, A.; Bachhuber, F. The cerebrospinal fluid and barriers—Anatomic and physiologic considerations. Handb. Clin. Neurol. 2017, 146, 21–32. [Google Scholar] [CrossRef]
- Ghersi-Egea, J.F.; Strazielle, N.; Catala, M.; Silva-Vargas, V.; Doetsch, F.; Engelhardt, B. Molecular anatomy and functions of the choroidal blood-cerebrospinal fluid barrier in health and disease. Acta Neuropathol. 2018, 135, 337–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solár, P.; Zamani, A.; Kubíčková, L.; Dubový, P.; Joukal, M. Choroid plexus and the blood–cerebrospinal fluid barrier in disease. Fluids Barriers CNS 2020, 17, 35. [Google Scholar] [CrossRef]
- Abbas, M. Potential Role of Nanoparticles in Treating the Accumulation of Amyloid-Beta Peptide in Alzheimer’s Patients. Polymers 2021, 13, 1051. [Google Scholar] [CrossRef]
- Cohen-Kashi-Malina, K.; Cooper, I.; Teichberg, V.I. Mechanisms of glutamate efflux at the blood-brain barrier: Involvement of glial cells. J. Cereb. Blood Flow Metab. 2012, 32, 177–189. [Google Scholar] [CrossRef]
- Sharif, Y.; Jumah, F.; Coplan, L.; Krosser, A.; Sharif, K.; Tubbs, R.S. Blood brain barrier: A review of its anatomy and physiology in health and disease. Clin. Anat. 2018, 31, 812–823. [Google Scholar] [CrossRef]
- Zaragozá, R. Transport of Amino Acids Across the Blood-Brain Barrier. Front. Physiol. 2020, 11, 973. [Google Scholar] [CrossRef]
- Segarra, M.; Aburto, M.R.; Acker-Palmer, A. Blood-Brain Barrier Dynamics to Maintain Brain Homeostasis. Trends Neurosci. 2021, 44, 393–405. [Google Scholar] [CrossRef]
- Knox, E.G.; Aburto, M.R.; Clarke, G.; Cryan, J.F.; O’Driscoll, C.M. The blood-brain barrier in aging and neurodegeneration. Mol. Psychiatry 2022, 27, 2659–2673. [Google Scholar] [CrossRef]
- Commission Recommendation of 18 October 2011 on the Definition of Nanomaterial (Text with EEA Relevance). Available online: https://op.europa.eu/en/publication-detail/-/publication/17af73d9-da70-4a46-a421-c62e3d1df6ce/language-en (accessed on 11 January 2023).
- Pokropivny, V.V.; Skorokhod, V.V. Classification of nanostructures by dimensionality and concept of surface forms engineering in nanomaterial science. Mater. Sci. Eng. C 2007, 27, 990–993. [Google Scholar] [CrossRef]
- Soares, S.; Sousa, J.; Pais, A.; Vitorino, C. Nanomedicine: Principles, Properties, and Regulatory Issues. Front. Chem. 2018, 6, 360. [Google Scholar] [CrossRef]
- Wang, Z.; Hu, T.; Liang, R.; Wei, M. Application of Zero-Dimensional Nanomaterials in Biosensing. Front. Chem. 2020, 8, 320. [Google Scholar] [CrossRef]
- Khan, N.H.; Mir, M.; Ngowi, E.E.; Zafar, U.; Khakwani, M.M.A.K.; Khattak, S.; Zhai, Y.K.; Jiang, E.S.; Zheng, M.; Duan, S.F.; et al. Nanomedicine: A Promising Way to Manage Alzheimer’s Disease. Front. Bioeng. Biotechnol. 2021, 9, 630055. [Google Scholar] [CrossRef]
- Joudeh, N.; Linke, D. Nanoparticle classification, physicochemical properties, characterization, and applications: A comprehensive review for biologists. J. Nanobiotechnol. 2022, 20, 262. [Google Scholar] [CrossRef]
- Byakodi, M.; Shrikrishna, N.S.; Sharma, R.; Bhansali, S.; Mishra, Y.; Kaushik, A.; Gandhi, S. Emerging 0D, 1D, 2D, and 3D nanostructures for efficient point-of-care biosensing. Biosens. Bioelectron. X 2022, 12, 100284. [Google Scholar] [CrossRef]
- Baranowska-Wójcik, E.; Szwajgier, D. Alzheimer’s disease: Review of current nanotechnological therapeutic strategies. Expert Rev. Neurother. 2020, 20, 271–279. [Google Scholar] [CrossRef]
- Ling, T.S.; Chandrasegaran, S.; Xuan, L.Z.; Suan, T.L.; Elaine, E.; Nathan, D.V.; Chai, Y.H.; Gunasekaran, B.; Salvamani, S. The Potential Benefits of Nanotechnology in Treating Alzheimer’s Disease. Biomed. Res. Int. 2021, 2021, 5550938. [Google Scholar] [CrossRef] [PubMed]
- Chopra, H.; Bibi, S.; Singh, I.; Kamal, M.A.; Islam, F.; Alhumaydhi, F.A.; Emran, T.B.; Cavalu, S. Nanomedicines in the Management of Alzheimer’s Disease: Current View and Future Prospects. Front. Aging Neurosci. 2022, 14, 879114. [Google Scholar] [CrossRef]
- Lin, P.; Sun, J.; Cheng, Q.; Yang, Y.; Cordato, D.; Gao, J. The Development of Pharmacological Therapies for Alzheimer’s Disease. Neurol. Ther. 2021, 10, 609–626. [Google Scholar] [CrossRef] [PubMed]
- Faiyaz, M.; Ganayee, M.A.; Akhtar, S.; Krishnan, S.; Flora, B.; Dogra, D.; Jha, N.K.; Chellappan, D.K.; Negi, P.; Dua, K.; et al. Nanomaterials in Alzheimer’s disease treatment: A comprehensive review. Front. Biosci. 2021, 26, 851–865. [Google Scholar] [CrossRef]
- Shankar, R.; Joshi, M.; Pathak, K. Lipid Nanoparticles: A Novel Approach for Brain Targeting. Pharm. Nanotechnol. 2018, 6, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Otte, A.; Park, K. Evolution of drug delivery systems: From 1950 to 2020 and beyond. J. Control. Release 2022, 342, 53–65. [Google Scholar] [CrossRef]
- Harish, V.; Tewari, D.; Gaur, M.; Yadav, A.B.; Swaroop, S.; Bechelany, M.; Barhoum, A. Review on Nanoparticles and Nanostructured Materials: Bioimaging, Biosensing, Drug Delivery, Tissue Engineering, Antimicrobial, and Agro-Food Applications. Nanomaterials 2022, 12, 457. [Google Scholar] [CrossRef]
- Paramasivam, G.; Palem, V.V.; Sundaram, T.; Sundaram, V.; Kishore, S.C.; Bellucci, S. Nanomaterials: Synthesis and Applications in Theranostics. Nanomaterials 2021, 11, 3228. [Google Scholar] [CrossRef]
- Maiti, D.; Tong, X.; Mou, X.; Yang, K. Carbon-Based Nanomaterials for Biomedical Applications: A Recent Study. Front. Pharmacol. 2019, 9, 1401. [Google Scholar] [CrossRef] [Green Version]
- Gupta, T.K.; Budarapu, P.R.; Chappidi, S.R.; Sudhir Sastry, Y.B.; Paggi, M.; Bordas, S.P. Advances in Carbon Based Nanomaterials for Bio-Medical Applications. Curr. Med. Chem. 2019, 26, 6851–6877. [Google Scholar] [CrossRef]
- Khan, I.; Saeed, K.; Khan, I. Nanoparticles: Properties, applications and toxicities. Arab. J. Chem. 2019, 12, 908–931. [Google Scholar] [CrossRef]
- Nascimento, M.A.; Cruz, J.C.; Rodrigues, G.D.; de Oliveira, A.F.; Lopes, R.P. Synthesis of polymetallic nanoparticles from spent lithium-ion batteries and application in the removal of reactive blue 4 dye. J. Clean. Prod. 2018, 202, 264–272. [Google Scholar] [CrossRef]
- Bhatti, R.; Shakeel, H.; Malik, K.; Qasim, M.; Khan, M.A.; Ahmed, N.; Jabeen, S. Inorganic Nanoparticles: Toxic Effects, Mechanisms of Cytotoxicity and Phytochemical Interactions. Adv. Pharm. Bull. 2022, 12, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Sumbal Nadeem, A.; Naz, S.; Ali, J.S.; Mannan, A.; Zia, M. Synthesis, characterization and biological activities of monometallic and bimetallic nanoparticles using Mirabilis jalapa leaf extract. Biotechnol. Rep. 2019, 22, e00338. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.C.; Harshita Mishra, P.K.; Talegaonkar, S. Ceramic Nanoparticles: Fabrication Methods and Applications in Drug Delivery. Curr. Pharm. Des. 2015, 21, 6165–6188. [Google Scholar] [CrossRef]
- Bhatia, R.; Sharma, A.; Narang, R.K.; Rawal, R.K. Recent Nanocarrier Approaches for Targeted Drug Delivery in Cancer Therapy. Curr. Mol. Pharmacol. 2021, 14, 350–366. [Google Scholar] [CrossRef] [PubMed]
- Dantas, K.C.F.; Rosário, J.D.S.; Silva-Caldeira, P.P. Polymeric Nanosystems Applied for Metal-Based Drugs and Photosensitizers Delivery: The State of the Art and Recent Advancements. Pharmaceutics 2022, 14, 1506. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Buchman, J.T.; Rodriguez, R.S.; Ring, H.L.; He, J.; Bantz, K.C.; Haynes, C.L. Stabilization of Silver and Gold Nanoparticles: Preservation and Improvement of Plasmonic Functionalities. Chem. Rev. 2019, 119, 664–699. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Malviya, R. Understanding and advancement in gold nanoparticle targeted photothermal therapy of cancer. Biochim. Biophys. Acta Rev. Cancer 2021, 1875, 188532. [Google Scholar] [CrossRef]
- Odion, R.A.; Liu, Y.; Vo-Dinh, T. Plasmonic Gold Nanostar-Mediated Photothermal Immunotherapy. IEEE J. Sel. Top. Quantum Electron. 2021, 27, 4800109. [Google Scholar] [CrossRef]
- Ross, C.; Taylor, M.; Fullwood, N.; Allsop, D. Liposome delivery systems for the treatment of Alzheimer’s disease. Int. J. Nanomed. 2018, 13, 8507–8522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baysal, I.; Ucar, G.; Gultekinoglu, M.; Ulubayram, K.; Yabanoglu-Ciftci, S. Donepezil loaded PLGA-b-PEG nanoparticles: Their ability to induce destabilization of amyloid fibrils and to cross blood brain barrier in vitro. J. Neural Transm. 2017, 124, 33–45. [Google Scholar] [CrossRef]
- Çınar, E.; Mutluay, S.U.; Baysal, İ.; Gültekinoğlu, M.; Ulubayram, K.; Çiftçi, S.Y.; Tel, B.C.; Uçar, G. Donepezil-loaded PLGA-b-PEG Nanoparticles Enhance the Learning and Memory Function of Beta-Amyloid Rat Model of Alzheimer’s Disease. Arch. Oneuropsychiatry 2022, 59, 281–289. [Google Scholar] [CrossRef]
- Kaur, A.; Nigam, K.; Bhatnagar, I.; Sukhpal, H.; Awasthy, S.; Shankar, S.; Tyagi, A.; Dang, S. Treatment of Alzheimer’s diseases using donepezil nanoemulsion: An intranasal approach. Drug Deliv. Transl. Res. 2020, 10, 1862–1875. [Google Scholar] [CrossRef]
- Ahlawat, J.; Henriquez, G.; Narayan, M. Enhancing the delivery of chemotherapeutics: Role of biodegradable polymeric nanoparticles. Molecules 2018, 23, 215. [Google Scholar] [CrossRef] [Green Version]
- Manek, E.; Darvas, F.; Petroianu, G.A. Use of Biodegradable, Chitosan-Based Nanoparticles in the Treatment of Alzheimer’s Disease. Molecules 2020, 25, 4866. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-López, E.; Ettcheto, M.; Egea, M.A.; Espina, M.; Cano, A.; Calpena, A.C.; Camins, A.; Carmona, N.; Silva, A.M.; Souto, E.B.; et al. Memantine loaded PLGA PEGylated nanoparticles for Alzheimer’s disease: In vitro and in vivo characterization. J. Nanobiotechnol. 2018, 27, 32. [Google Scholar] [CrossRef]
- Gothwal, A.; Kumar, H.; Nakhate, K.T.; Ajazuddin Dutta, A.; Borah, A.; Gupta, U. Lactoferrin Coupled Lower Generation PAMAM Dendrimers for Brain Targeted Delivery of Memantine in Aluminum-Chloride-Induced Alzheimer’s Disease in Mice. Bioconjug. Chem. 2019, 30, 2573–2583. [Google Scholar] [CrossRef]
- Ordóñez-Gutiérrez, L.; Wandosell, F. Nanoliposomes as a Therapeutic Tool for Alzheimer’s Disease. Front. Synaptic Neurosci. 2020, 12, 20. [Google Scholar] [CrossRef]
- Perche, F.; Uchida, S.; Akiba, H.; Lin, C.Y.; Ikegami, M.; Dirisala, A.; Nakashima, T.; Itaka, K.; Tsumoto, K.; Kataoka, K. Improved Brain Expression of Anti-Amyloid β scFv by Complexation of mRNA Including a Secretion Sequence with PEG-based Block Catiomer. Curr. Alzheimer Res. 2017, 14, 295–302. [Google Scholar] [CrossRef]
- Xie, J.; Gonzalez-Carter, D.; Tockary, T.A.; Nakamura, N.; Xue, Y.; Nakakido, M.; Akiba, H.; Dirisala, A.; Liu, X.; Toh, K.; et al. Dual-Sensitive Nanomicelles Enhancing Systemic Delivery of Therapeutically Active Antibodies Specifically into the Brain. ACS Nano 2020, 14, 6729–6742. [Google Scholar] [CrossRef]
- Gonzalez-Carter, D.; Liu, X.; Tockary, T.A.; Dirisala, A.; Toh, K.; Anraku, Y.; Kataoka, K. Targeting nanoparticles to the brain by exploiting the blood-brain barrier impermeability to selectively label the brain endothelium. Proc. Natl. Acad. Sci. USA 2020, 117, 19141–19150. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.; Geetha, K.M. Neurotherapeutic applications of nanomedicine for treating Alzheimer’s disease. J. Control. Release 2020, 325, 25–37. [Google Scholar] [CrossRef]
- Thapa, R.K.; Kim, J.O. Nanomedicine-based commercial formulations: Current developments and future prospects. J. Pharm. Investig. 2023, 53, 19–33. [Google Scholar] [CrossRef]
- Hamblin, M.R. Shining light on the head: Photobiomodulation for brain disorders. BBA Clin. 2016, 6, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Ailioaie, L.M.; Ailioaie, C.; Litscher, G. Latest Innovations and Nanotechnologies with Curcumin as a Nature-Inspired Photosensitizer Applied in the Photodynamic Therapy of Cancer. Pharmaceutics 2021, 13, 1562. [Google Scholar] [CrossRef]
- Tretkoff, E. This Month in Physics History: Einstein Predicts Stimulated Emission. Am. Phys. Soc. News 2005, 14, 8. Available online: https://www.aps.org/publications/apsnews/200508/history.cfm# (accessed on 21 December 2022).
- The Nobel Prize in Physics 1964. Award Ceremony Speech. Presentation Speech by Professor B. Edlén, Member of the Nobel Committee for Physics. Available online: https://www.nobelprize.org/prizes/physics/1964/ceremony-speech/ (accessed on 21 December 2022).
- Ailioaie, L.M.; Litscher, G. Photobiomodulation and Sports: Results of a Narrative Review. Life 2021, 11, 1339. [Google Scholar] [CrossRef] [PubMed]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef]
- Glass, G.E. Photobiomodulation: The Clinical Applications of Low-Level Light Therapy. Aesthetic Surg. J. 2021, 41, 723–738. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Wang, J.; Liu, L. Alzheimer’s Therapeutic Strategy: Photoactive Platforms for Suppressing the Aggregation of Amyloid β Protein. Front. Chem. 2020, 8, 509. [Google Scholar] [CrossRef]
- Han, J.; Du, Z.; Lim, M.H. Mechanistic Insight into the Design of Chemical Tools to Control Multiple Pathogenic Features in Alzheimer’s Disease. Acc. Chem. Res. 2021, 54, 3930–3940. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Y.; Chen, A.C.; Carroll, J.D.; Hamblin, M.R. Biphasic dose response in low level light therapy. Dose-Response 2009, 7, 358–383. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, J.T.; Huang, Y.Y.; Osmani, B.Z.; Sharma, S.K.; Naeser, M.A.; Hamblin, M.R. Role of low-level laser therapy in neurorehabilitation. PM&R 2010, 2, S292–S305. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-Y.; Sharma, S.K.; Carroll, J.; Hamblin, M.R. Biphasic dose response in low-level light therapy—An update. Dose-Response 2011, 9, 358–383. [Google Scholar] [CrossRef] [PubMed]
- Blivet, G.; Meunier, J.; Roman, F.J.; Touchon, J. Neuroprotective effect of a new photobiomodulation technique against Aβ25-35 peptide-induced toxicity in mice: Novel hypothesis for therapeutic approach of Alzheimer’s disease suggested. Alzheimers Dement. 2018, 4, 54–63. [Google Scholar] [CrossRef]
- Sutherland, J.C. Biological effects of polychromatic light. Photochem. Photobiol. 2002, 76, 164–170. [Google Scholar] [CrossRef]
- Caldieraro, M.A.; Laufer-Silva, T.; Cassano, P. Dosimetry and Clinical Efficacy of Transcranial Photobiomodulation for Major Depression Disorder: Could they Guide Dosimetry for Alzheimer’s Disease? J. Alzheimers Dis. 2021, 83, 1453–1469. [Google Scholar] [CrossRef]
- Farivar, S.; Malekshahabi, T.; Shiari, R. Biological effects of low level laser therapy. J. Lasers Med. Sci. 2014, 5, 58–62. [Google Scholar]
- De Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [Green Version]
- Ailioaie, L.M.; Litscher, G. Curcumin and Photobiomodulation in Chronic Viral Hepatitis and Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 7150. [Google Scholar] [CrossRef]
- Hamblin, M.R. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef]
- Mewies, M.; McIntire, W.S.; Scrutton, N.S. Covalent attachment of flavin adenine dinucleotide (FAD) and flavin mononucleotide (FMN) to enzymes: The current state of affairs. Protein Sci. 1998, 7, 7–20. [Google Scholar] [CrossRef] [Green Version]
- Melin, F.; Hellwig, P. Redox Properties of the Membrane Proteins from the Respiratory Chain. Chem. Rev. 2020, 120, 10244–10297. [Google Scholar] [CrossRef] [PubMed]
- Lienhart, W.D.; Gudipati, V.; Macheroux, P. The human flavoproteome. Arch. Biochem. Biophys. 2013, 535, 150–162. [Google Scholar] [CrossRef] [Green Version]
- Panja, S.; Siegel, D.; Camandola, S.; de Cabo, R.; Ross, D.; Mallela, K.M.G. FAD-deficient P187S mutation of NAD(P)H:quinone oxidoreductase 1 (NQO1*2) binds and accelerates β-amyloid aggregation. Biosci. Rep. 2022, 42, BSR20220643. [Google Scholar] [CrossRef]
- Pruitt, T.; Carter, C.; Wang, X.; Wu, A.; Liu, H. Photobiomodulation at Different Wavelengths Boosts Mitochondrial Redox Metabolism and Hemoglobin Oxygenation: Lasers vs. Light-Emitting Diodes In Vivo. Metabolites 2022, 12, 103. [Google Scholar] [CrossRef] [PubMed]
- Karu, T. Primary and secondary mechanisms of action of visible to near-IR radiation on cells. J. Photochem. Photobiol. B 1999, 49, 1–17. [Google Scholar] [CrossRef]
- Karu, T.; Kolyakov, S.F. Exact Action Spectra for Cellular Responses Relevant to Phototherapy. Photomed. Laser Surg. 2005, 23, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karu, T.I.; Pyatibrat, L.V.; Kolyakov, S.F.; Afanasyeva, N.I. Absorption measurements of a cell monolayer relevant to phototherapy: Reduction of cytochrome c oxidase under near IR radiation. J. Photochem. Photobiol. B 2005, 81, 98–106. [Google Scholar] [CrossRef]
- Karu, T.I. Mitochondrial signaling in mammalian cells activated by red and near-IR radiation. Photochem. Photobiol. 2008, 84, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Lunova, M.; Smolková, B.; Uzhytchak, M.; Janoušková, K.Ž.; Jirsa, M.; Egorova, D.; Kulikov, A.; Kubinová, Š.; Dejneka, A.; Lunov, O. Light-induced modulation of the mitochondrial respiratory chain activity: Possibilities and limitations. Cell. Mol. Life Sci. 2020, 77, 2815–2838. [Google Scholar] [CrossRef]
- Hamblin, M.R. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochem. Photobiol. 2018, 94, 199–212. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Zhou, T.; Liu, L.; Ohulchanskyy, T.Y.; Qu, J. Dose–effect relationships for PBM in the treatment of Alzheimer’s disease. J. Phys. D Appl. Phys. 2021, 54, 353001. [Google Scholar] [CrossRef]
- Karu, T.I. Multiple roles of cytochrome c oxidase in mammalian cells under action of red and IR-A radiation. IUBMB Life 2010, 62, 607–610. [Google Scholar] [CrossRef]
- Slater, E.C. Peter Dennis Mitchell, 29 September 1920–10 April 1992. Biogr. Mem. Fellows R. Soc. 1994, 40, 283–305. [Google Scholar] [CrossRef]
- Mills, E.L.; Kelly, B.; Logan, A.; Costa, A.S.; Varma, M.; Bryant, C.E.; Tourlomousis, P.; Däbritz, J.H.M.; Gottlieb, E.; Latorre, I.; et al. Succinate Dehydrogenase Supports Metabolic Repurposing of Mitochondria to Drive Inflammatory Macrophages. Cell 2016, 167, 457–470. [Google Scholar] [CrossRef] [Green Version]
- Poderoso, J.J.; Helfenberger, K.; Poderoso, C. The effect of nitric oxide on mitochondrial respiration. Nitric Oxide 2019, 88, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Passarella, S.; Karu, T. Absorption of monochromatic and narrow band radiation in the visible and near IR by both mitochondrial and non-mitochondrial photoacceptors results in photobiomodulation. J. Photochem. Photobiol. B Biol. 2014, 140, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.P. Mitochondrial cytochrome c oxidase is not the primary acceptor for near infrared light-it is mitochondrial bound water: The principles of low-level light therapy. Ann. Transl. Med. 2019, 7, S13. [Google Scholar] [CrossRef]
- Liebert, A.; Capon, W.; Pang, V.; Vila, D.; Bicknell, B.; McLachlan, C.; Kiat, H. Photophysical Mechanisms of Photobiomodulation Therapy as Precision Medicine. Biomedicines 2023, 11, 237. [Google Scholar] [CrossRef]
- Bathini, M.; Raghushaker, C.R.; Mahato, K.K. The Molecular Mechanisms of Action of Photobiomodulation against Neurodegenerative Diseases: A Systematic Review. Cell. Mol. Neurobiol. 2022, 42, 955–971. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Yang, L.; Feng, S.; Zhu, L.; Yang, L.; Liu, T.C.; Duan, R. Therapeutic non-invasive brain treatments in Alzheimer’s disease: Recent advances and challenges. Inflamm. Regen. 2022, 42, 31. [Google Scholar] [CrossRef] [PubMed]
- Ambrosetti, A.; Umari, P.; Silvestrelli, P.L.; Elliott, J.; Tkatchenko, A. Optical van-der-Waals forces in molecules: From electronic Bethe-Salpeter calculations to the many-body dispersion model. Nat. Commun. 2022, 13, 813. [Google Scholar] [CrossRef]
- Taboada, L.D.; Yu, J.; El-Amouri, S.; Gattoni-Celli, S.; Richieri, S.; McCarthy, T.; Streeter, J.; Kindy, M.S. Transcranial Laser Therapy Attenuates Amyloid-β Peptide Neuropathology in Amyloid-β Protein Precursor Transgenic Mice. J. Alzheimer’s Dis. 2011, 23, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Purushothuman, S.; Johnstone, D.M.; Nandasena, C.; Mitrofanis, J.; Stone, J. Photobiomodulation with near infrared light mitigates Alzheimer’s disease related pathology in cerebral cortex—Evidence from two transgenic mouse models. Alzheimer’s Res. Ther. 2014, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, T.H.; Wider, J.M.; Lee, I.; Reynolds, C.A.; Liu, J.; Lepore, B.; Tousignant, R.; Bukowski, M.J.; Johnston, H.; Fite, A.; et al. Inhibitory modulation of cytochrome c oxidase activity with specific near-infrared light wavelengths attenuates brain ischemia/reperfusion injury. Sci. Rep. 2018, 8, 3481. [Google Scholar] [CrossRef] [Green Version]
- Enengl, J.; Hamblin, M.R.; Dungel, P. Photobiomodulation for Alzheimer’s disease: Translating basic research to clinical application. J. Alzheimers Dis. 2020, 75, 1073–1082. [Google Scholar] [CrossRef]
- Gomez, A.; Sainbhi, A.S.; Froese, L.; Batson, C.; Alizadeh, A.; Mendelson, A.A.; Zeiler, F.A. Near infrared spectroscopy for high-temporal resolution cerebral physiome characterization in TBI: A narrative review of techniques, applications, and future directions. Front. Pharmacol. 2021, 12, 719501. [Google Scholar] [CrossRef]
- Li, Q.; Peng, J.; Luo, Y.; Zhou, J.; Li, T.; Cao, L.; Peng, S.; Zuo, Z.; Wang, Z. Far infrared light irradiation enhances Aβ clearance via increased exocytotic microglial ATP and ameliorates cognitive deficit in Alzheimer’s disease-like mice. J. Neuroinflamm. 2022, 19, 145. [Google Scholar] [CrossRef]
- Nizamutdinov, D.; Ezeudu, C.; Wu, E.; Huang, J.H.; Yi, S.S. Transcranial near-infrared light in treatment of neurodegenerative diseases. Front. Pharmacol. 2022, 13, 965788. [Google Scholar] [CrossRef] [PubMed]
- Huynh, Q.-S.; Elangovan, S.; Holsinger, R.M.D. Non-Pharmacological Therapeutic Options for the Treatment of Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 23, 11037. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, J.; Romani, M.; Bernardo, G.; Popa, T.; Ziviani, E.; Hummel, F.C.; Sorrentino, V.; Millet, G.P. Boosting mitochondrial health to counteract neurodegeneration. Prog. Neurobiol. 2022, 215, 102289. [Google Scholar] [CrossRef] [PubMed]
- Blanco, N.J.; Maddox, W.T.; Gonzalez-Lima, F. Improving executive function using transcranial infrared laser stimulation. J. Neuropsychol. 2017, 11, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Saltmarche, A.E.; Naeser, M.A.; Ho, K.F.; Hamblin, M.R.; Lim, L. Significant Improvement in Cognition in Mild to Moderately Severe Dementia Cases Treated with Transcranial Plus Intranasal Photobiomodulation: Case Series Report. Photomed. Laser Surg. 2017, 35, 432–441. [Google Scholar] [CrossRef]
- Berman, M.H.; Halper, J.P.; Nichols, T.W.; Jarrett, H.; Lundy, A.; Huang, J.H. Photobiomodulation with Near Infrared Light Helmet in a Pilot, Placebo Controlled Clinical Trial in Dementia Patients Testing Memory and Cognition. J. Neurol Neurosci. 2017, 8, 176. [Google Scholar] [CrossRef] [Green Version]
- Cassano, P.; Petriem, S.R.; Mischoulon, D.; Cusin, C.; Katnani, H.; Yeung, A.; De Taboada, L.; Archibald, A.; Bui, E.; Baer, L.; et al. Transcranial Photobiomodulation for the Treatment of Major Depressive Disorder. The ELATED-2 Pilot Trial. Photomed. Laser Surg. 2018, 36, 634–646. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.S.; Lee, T.L.; Yeung, M.K.; Hamblin, M.R. Photobiomodulation improves the frontal cognitive function of older adults. Int. J. Geriatr. Psychiatry 2019, 34, 369–377. [Google Scholar] [CrossRef]
- Maiello, M.; Losiewicz, O.M.; Bui, E.; Spera, V.; Hamblin, M.R.; Marques, L.; Cassano, P. Transcranial Photobiomodulation with Near-Infrared Light for Generalized Anxiety Disorder: A Pilot Study. Photobiomodul. Photomed. Laser Surg. 2019, 37, 644–650. [Google Scholar] [CrossRef]
- Holmes, E.; Barrett, D.W.; Saucedo, C.L.; O’Connor, P.; Liu, H.; Gonzalez-Lima, F. Cognitive Enhancement by Transcranial Photobiomodulation Is Associated with Cerebrovascular Oxygenation of the Prefrontal Cortex. Front. Neurosci. 2019, 13, 1129. [Google Scholar] [CrossRef]
- Chan, A.S.; Lee, T.L.; Hamblin, M.R.; Cheung, M.C. Photobiomodulation Enhances Memory Processing in Older Adults with Mild Cognitive Impairment: A Functional Near-Infrared Spectroscopy Study. J. Alzheimers Dis. 2021, 83, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Lee, T.L.; Hamblin, M.R.; Cheung, M.C. Photoneuromodulation makes a difficult cognitive task less arduous. Sci. Rep. 2021, 11, 13688. [Google Scholar] [CrossRef] [PubMed]
- Dougal, G.; Ennaceur, A.; Chazot, P.L. Effect of Transcranial Near-Infrared Light 1068 nm Upon Memory Performance in Aging Healthy Individuals: A Pilot Study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Spera, V.; Sitnikova, T.; Ward, M.J.; Farzamt, P.; Hughes, J.; Gazecki, S.; Bui, E.; Maiello, M.; De Taboada, L.; Hamblin, M.R.; et al. Pilot Study on Dose-Dependent Effects of Transcranial Photobiomodulation on Brain Electrical Oscillations: A Potential Therapeutic Target in Alzheimer’s Disease. J. Alzheimers Dis. 2021, 83, 1481–1498. [Google Scholar] [CrossRef]
- Qi, X.; Nizamutdinov, D.; Berman, M.H.; Dougal, G.; Chazot, P.L.; Wu, E.; Stevens, A.B.; Yi, S.S.; Huang, J.H. Gender Differences of Dementia in Response to Intensive Self-Administered Transcranial and Intraocular Near-Infrared Stimulation. Cureus 2021, 13, e16188. [Google Scholar] [CrossRef] [PubMed]
- Nizamutdinov, D.; Qi, X.; Berman, M.H.; Dougal, G.; Dayawansa, S.; Wu, E.; Yi, S.S.; Stevens, A.B.; Huang, J.H. Transcranial Near Infrared Light Stimulations Improve Cognition in Patients with Dementia. Aging Dis. 2021, 12, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E.N.; Ali, A.Y.; Behiry, M.E.; Naguib, M.M.; Elsayed, M.M. Impact of Combined Photo-Biomodulation and Aerobic Exercise on Cognitive Function and Quality-of-Life in Elderly Alzheimer Patients with Anemia: A Randomized Clinical Trial. Int. J. Gen. Med. 2021, 14, 141–152. [Google Scholar] [CrossRef]
- Saucedo, C.L.; Courtois, E.C.; Wade, Z.S.; Kelley, M.N.; Kheradbin, N.; Barrett, D.W.; Gonzalez-Lima, F. Transcranial laser stimulation: Mitochondrial and cerebrovascular effects in younger and older healthy adults. Brain Stimul. 2021, 14, 440–449. [Google Scholar] [CrossRef]
- Iosifescu, D.V.; Norton, R.J.; Tural, U.; Mischoulon, D.; Collins, K.; McDonald, E.; De Taboada, L.; Foster, S.; Cusin, C.; Yeung, A.; et al. Very Low-Level Transcranial Photobiomodulation for Major Depressive Disorder: The ELATED-3 Multicenter, Randomized, Sham-Controlled Trial. J. Clin. Psychiatry 2022, 83, 42180. [Google Scholar] [CrossRef]
- Vrankic, M.; Vlahinić, S.; Šverko, Z.; Markovinović, I. EEG-Validated Photobiomodulation Treatment of Dementia—Case Study. Sensors 2022, 22, 7555. [Google Scholar] [CrossRef]
- Stephan, W.; Banas, L.J.; Hamblin, M.R. Treatment Efficacy of Photobiomodulation for Moderate and Advanced Dementia or Alzheimer’s Disease: Case Studies. Adv. Alzheimer’s Dis. 2022, 11, 39–47. [Google Scholar] [CrossRef]
- Wang, X.; Wanniarachchi, H.; Wu, A.; Liu, H. Combination of Group Singular Value Decomposition and eLORETA Identifies Human EEG Networks and Responses to Transcranial Photobiomodulation. Front. Hum. Neurosci. 2022, 16, 853909. [Google Scholar] [CrossRef] [PubMed]
- Maksimovich, I.V. Transcatheter Intracerebral Laser Photobiomodulation Therapy Reduces Dementia and Cognitive Impairment in Patients with various Stages of Alzheimer’s disease. Med. Res. Arch. 2022, 10. [Google Scholar] [CrossRef]
- Cheung, M.C.; Lee, T.L.; Sze, S.L.; Chan, A.S. Photobiomodulation improves frontal lobe cognitive functions and mental health of older adults with non-amnestic mild cognitive impairment: Case studies. Front. Psychol. 2023, 13, 1095111. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Vemireddy, V.; Cai, Q.; Xiong, H.; Kang, P.; Li, X.; Giannotta, M.; Hayenga, H.N.; Pan, E.; Sirsi, S.R.; et al. Reversibly Modulating the Blood-Brain Barrier by Laser Stimulation of Molecular-Targeted Nanoparticles. Nano Lett. 2021, 21, 9805–9815. [Google Scholar] [CrossRef]
- Ailioaie, L.M.; Ailioaie, C.; Litscher, G.; Chiran, D.A. Celiac Disease and Targeting the Molecular Mechanisms of Autoimmunity in COVID Pandemic. Int. J. Mol. Sci. 2022, 23, 7719. [Google Scholar] [CrossRef]




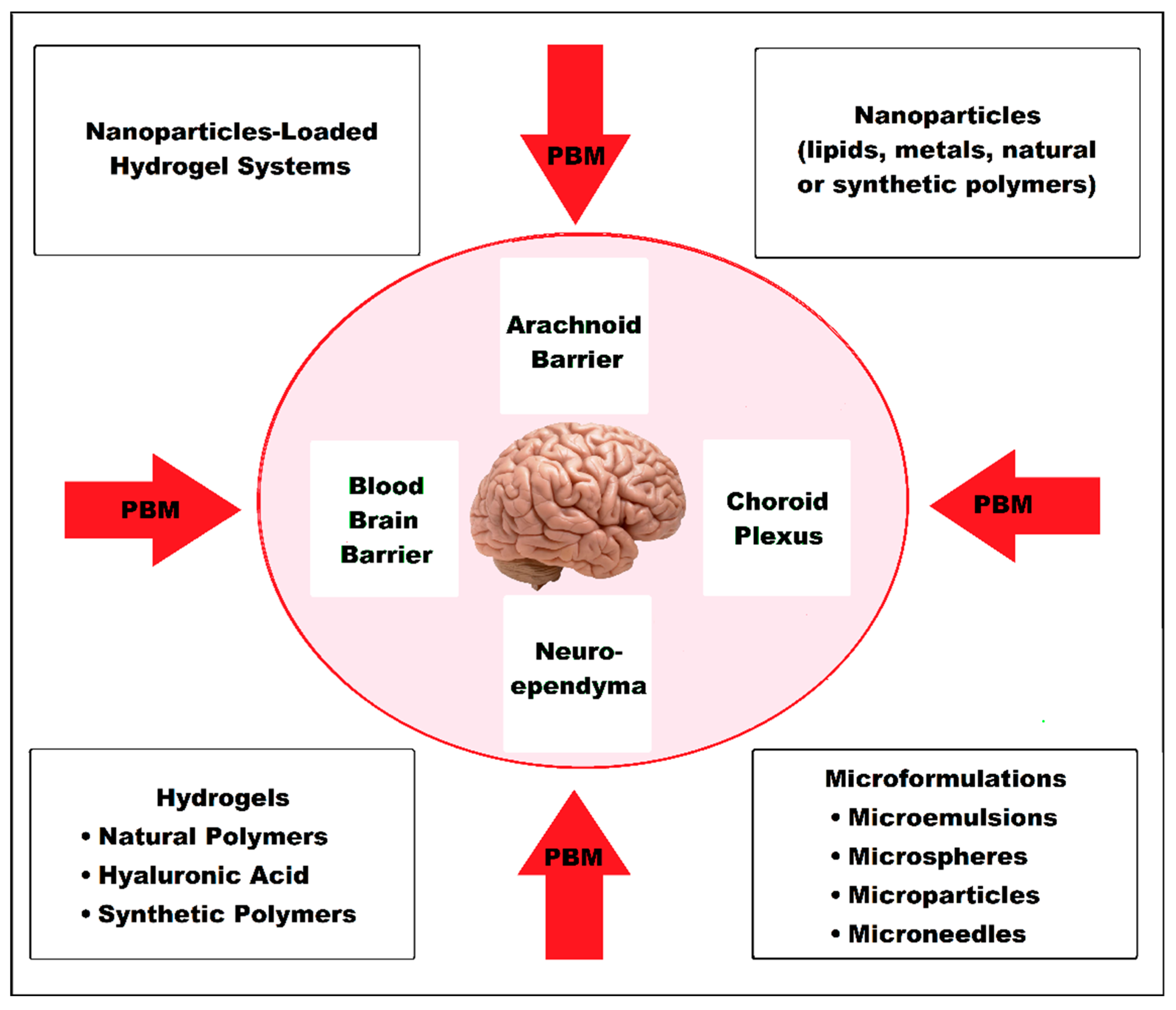{kind=link}
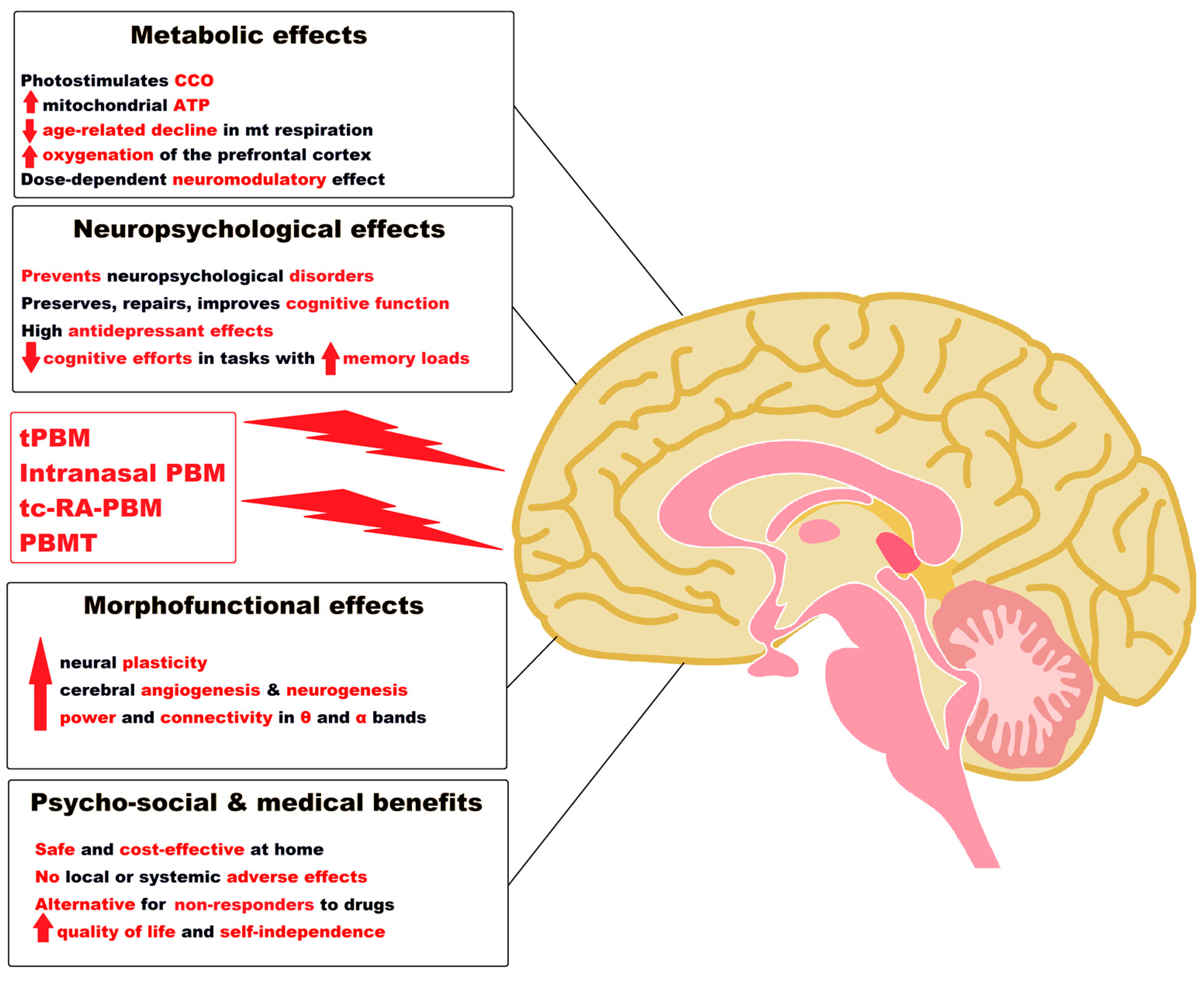{kind=link}
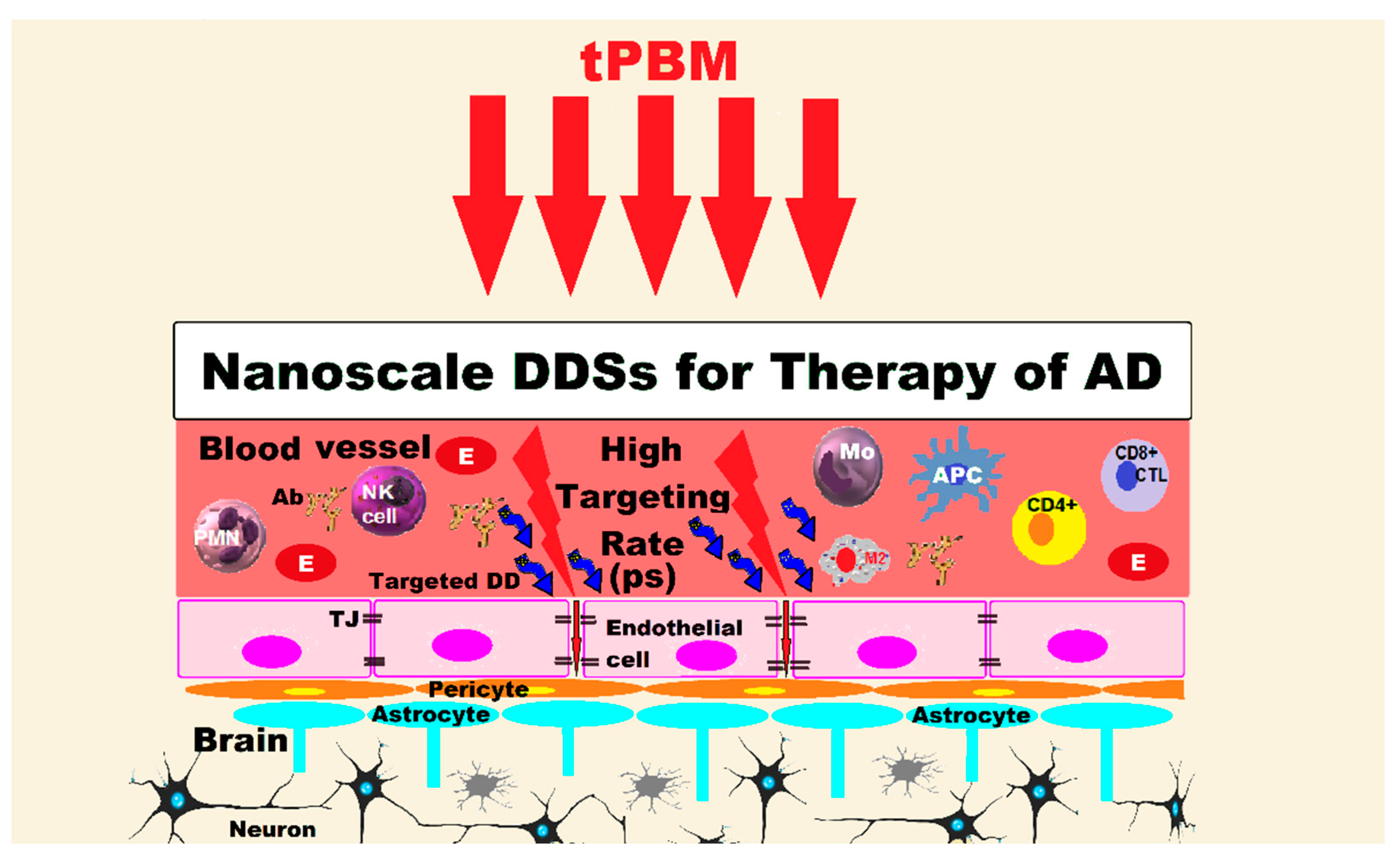{kind=link}
| Hybrid Compounds | Main Pharmacological Actions | References | ||||
|---|---|---|---|---|---|---|
| Donepezil-based hybrids | Selectively and reversibly inhibits the human AChE and BChE. | Strong inhibition of aggregation of the Aβ peptide. | Protect neurons from the damage due to mitochondrial free radicals and have antioxidant activity. | Metal chelating action. | Increased potential to infiltrate BBB and reduced neurotoxicity. | [91,92,93] |
| Rivastigmine-based hybrids | Dual inhibition of AChE and BChE; specific monoamine oxidase-B (MAO-B) inhibitor. | Inhibit Aβ 1-42 aggregation, induced by Cu2+. | Anti-oxidative activity with reduced hepatotoxicity | Bio- metal chelating properties. | Provide neuroprotection. Favorable for BBB infiltration in vitro. | [94,95,96] |
| Galantamine-based hybrids (tertiary alkaloid of natural origin) | Strongly inhibit AChE activity in the synapse. | Decrease Aβ plaques. | Antioxidant and anti-inflammatory action. | Metal chelating action. | Cross the BBB by passive diffusion, and appear free of neurotoxicity. | [97,98,99] |
| Carbamate-conjugated hybrids (It has superior chemical stability due to the carbamic group, and ability to increase the permeability of biological membranes.) | Compound 6 has highly selective BChE inhibitory activity. Compound 7 demonstrated the highest AChEI activity by reversible noncompetitive partial inhibition. | Anti-amyloidogenic effect. Compound 8 strongly inhibits Aβ aggregation. | Have antioxidant-mediated neuroprotective activities. | Ability to chelate specific metals. | Better BBB permeability. | [100,101] |
| Physostigmine-conjugated hybrids | Tolserine and phenserine derived from physostigmine (PSM), are some non-competitive, selective and long-acting AChEI chemicals. | Reduce amyloid precursor protein (APP). | Tolserine is 200 times more selective for human AChE than for human BChE. | Phenserine is a selective AChEI with reduced side effects if compared to traditional AChEIs. | Phenserine has ability to inhibit Aβ-aggregation and was used for the treatment of cognitive impairment induced by traumatic brain injury in experimental studies. | [84,102,103] |
| Rhein-Huprine-conjugated hybrids | hAChE and hBChE are inhibited by synthesized rhein-huprine hybrids | Compound 16 is a therapeutic anti-Alzheimer candidate because it has multiple actions on hAChE, hBChE, BACE-1 and the accumulation of Aβ42. | [84] | |||
| Novel Hybrid Therapeutic Compounds Targeting AD | Biflavonoids significantly inhibited Aβ 1-42 fibrillization. | Amentoflavone (AMF) appears to have the greatest effect in suppressing fibrillization and complete disaggregation of Aβ 1-42 fibrils in AD. | Compound 17 would stimulate neurorejuvenation and arrest neurodegeneration in AD. | AMF can reduce extracellular Aβ by increasing its cellular uptake and clearance. | Berberine (BB), an isoquinoline alkaloid, might interfere with the pathogenic processes in AD by decreasing the levels of Aβ, blocking the activity of secretases in the APP pathway, reducing oxidative stress, astrocytosis and neuronal degradation. | [104,105,106,107,108,109] |
| Generic Name and Year of Approval | Trade or Brand Names | Route of Administration and Doses | Clinical Benefits | Side Effects | References | |||
|---|---|---|---|---|---|---|---|---|
| Gastrointestinal | Neuropsychiatric | Allergic Reactions | Other Effects | |||||
| Mechanism of Action: Acetylcholinesterase Inhibitors (AChEIs) | ||||||||
| Donepezil 1996, FDA. 2022, FDA: first transdermal system (Adlarity®). | Aricept, Aricept ODT, Adlarity, others | Orally standard dose (5–10 mg); high dose (23 mg). Adlarity as one transdermal patch applied to the skin once weekly. | A small benefit in mental function and ability to function. | Nausea; vomiting; diarrhea; loss of appetite; signs of stomach bleeding, etc. | Insomnia, or feeling tired; depression; hallucinations; convulsions; painful or difficult urination, etc. | Hives; difficulty breathing; swelling of face, lips, tongue, or throat, etc. | Increased creatine phosphokinase; dehydration; hyperlipemia; diabetes mellitus, goiter, liver dysfunction, etc. | [75] [92] [117,118,119,120,149] [151,152,153,154] [161,162,163,164,165] |
| Rivastigmine 2000, FDA. | Exelon®,Prometax, others | Initial dose: 1.5 mg orally twice a day; can be increased to 3 mg twice a day; Transdermal patch: initial dose: 4.6 mg/24 h patch applied to the skin once daily; maximum dose: 13.3 mg/24 h. | Effective symptomatically in all types of dementia; allowing patients to be independent and “be themselves” for a long time. | Ulcer or stomach bleeding; vomiting; diarrhea; nausea etc. | Convulsions; tremors, jerky muscle movements in the eyes, tongue, jaw or neck. | Urticaria; difficult breathing; swelling of the face, lips, tongue or throat; severe skin redness, itching or irritation; asthma, etc. | Liver or kidney dysfunctions; dehydration symptoms. Heart and lung problems, etc. | [77] [94,95,96] [166,167,168,169] [170] [171,172,173,174] [175] [176] |
| Galantamine 2001, FDA; 2003, FDA: extended-release capsules. | Razadyne Razadyne ER, Reminyl® others | 8–24 mg per day divided into 2 doses. | Improves cognition, function and activities of daily living.Delays the development of behavioral disturbances and psychiatric symptoms. | Nausea; vomiting; diarrhea; loss of appetite; upper abdominal pain, etc. | Tiredness; itching; headache; dizziness; feeling very thirsty or hot, etc. | Skin rash; hot and dry skin; progressive red or purple rash that causes blisters and peeling, etc. | Dark urine; clay-colored stools; jaundice with yellowing of the skin or eyes; blood in urine; bloody or tarry stools, etc. | [97,98,99] [121,122,123] [167] [177,178,179] [180,181] |
| Mechanism of Action: NMDA Receptor Antagonist | ||||||||
| Memantine 2002, EMA. 2003, FDA. | Namenda Namenda XR, Axura, Ebixa, others | Standard doses: 10–20 mg/daily (divided into 2 doses). | Moderately improves cognition, mood, behavior and ability to perform daily activities. | Vomiting; abdominal pain; diarrhea; loss of appetite; constipation; pancreatitis, etc. | Dizziness; headache; confusion; fatigue; pain; pain in the joints; lower back or muscle pain or stiffness; hallucinations; confusion; aggressive behavior; suicidal ideation, etc. | Swelling of the tongue, lips, or face; shortness of breath; skin rash; urticaria, etc. | Cardiac disorders—congestive heart failure. Hepatobiliary disorders—hepatitis. Renal and urinary disorders. Musculoskeletaldisorders, etc. | [80] [114,115,116,117,118,119,120] [182] [183] [184] |
| Mechanism of Action: AChEI and NMDA Receptor Antagonist. Mixt Products. | ||||||||
| Memantine/Donepezil (Rx) 2014, FDA. | Namzaric® | Standard dose: 28 mg memantine/10 mg donepezil; once daily in the evening. 14 mg/10 mg for patients with severe renal impairment. | Namzaric may help improve cognition and global function in patients with moderate and severe forms of AD. | Vomiting; constipation; diarrhea; loss of appetite; abdominal pain; signs of stomach bleeding; severe heartburn or abdominal pain, bloody or tarry stools, etc. | Headache; dizziness; somnolence; anxiety; aggression; depression, etc. | Urticaria; difficult breathing; swelling of the face, lips, tongue, or throat, etc. | Cardiovascular disorders: slow heartbeats or chest pain; hypertension or hypotension; New or worsening breathing problems. Urinary incontinence. Bruises; coughing up blood, etc. | [118] [119] [120] [185] |
| Mechanism of Action: Anti-amyloid Monoclonal Antibodies for Alzheimer′s Disease | ||||||||
| Aducanumab 2021, FDA. EMA rejected it in 2021. | Aduhelm, Aducanumab-avwa, BIIB037, BIIB-037. | Administered standard as IV infusion 10 mg/kg every 4 weeks and at least 21 days apart. | It binds to Aβ oligomers and promotes their clearance, being able to reduce Aβ accumulation and slow the progression of cognitive impairment. A modest clinical benefit in AD, but significant adverse events (ARIA) and high cost. It has sparked benefit-risk controversies. | Nausea, diarrhea, etc. | Headache; vertigo; dizziness; altered mental status; confusion; incoherent talk; disorientation; seizures, etc. | Urticaria; difficulty breathing; swelling of the face, lips, tongue, or throat, etc. | Visual disturbances; ARIA-E: cerebral edema including greater sulcal effusion in carriers of apolipoprotein E4. ARIA-H: superficial siderosis; microhemorrhages, etc. | [121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137] [156] [186] [187] |
| Lecanemab (Rx) Accelerated approval on 6 January 2023 by the FDA. | Leqembi, Lecanemab-irmb, BAN2401, mAb158 | Intravenous infusion; 10 mg/kg IV once every 2 weeks. | Lecanemab led to a rapid and pronounced decrease in amyloid plaques as well as a delay in clinical decline. | Nausea, vomiting, diarrhea, etc. | Headache; postural instability; confusion; incoherent talk; disorientation, etc. | Infusion-related reactions. Fever. Flu-like symptoms (chills, generalized aches, feeling shaky, and joint pain). | Atrial fibrillation; Hypotension or hypertension, oxygen desaturation, cough. Lymphopenia. ARIA-E (edema/effusion, etc.). ARIA-H (combined cerebral microhemorrhages, cerebral macrohemorrhages and superficial siderosis). | [139] [142] [145] [159] [160] [188] [170] |
| Reference | Type of Study and Modality of Work | Protocol of the Study | Study Results | Conclusions |
|---|---|---|---|---|
| [291] | Placebo controlled study for 30 (13 female; 17 male) students, mean age 20.4 yrs. 15 participants received active tPBM, and the other half, placebo. tPBM session lasted 8 min, administered in 8 one-minute treatments alternating between two locations on the forehead, each location was 4 cm in diameter. To quantify the effects of tPBM, the neuropsychological Wisconsin Card Sorting Test (WCST) was used, which is the gold-standard of executive function, including attention and memory. | A 1064 nm laser, 250 mW/cm2 (3400 mW/13.6 cm2 = 250 mW/cm2) was used for 4 min (3.4 W × 240 s = 816 J/location), which corresponded to an energy density of 60 J/cm2 (0.25 W/cm2 × 240 s = 60 J/cm2). | Study demonstrated that tPBM can improve cognitive function in healthy young adults in only 8 min. | tPBM with 1064 nm has proven experimentally that it can photostimulate CCO, the enzyme that catalyses oxygen consumption for energy production metabolism. It improved cognitive functions and would have an interesting potential for therapy or prevention of deficits from neuropsychological disorders or due to the aging process. |
| [292] | Case Series Report 5 old patients with “mild to moderate-severe” dementia and AD received tPBM and intranasal PBM with 810 nm, 10 Hz pulsed LEDs (41 transcranial and 23 intranasal diodes), 25 min/session at home, for 12 weeks. | Patients kept a “Daily Home Treatment Journal”, and at the clinic; changes in memory, cognition, general health conditions and any adverse effects were noted. | Mini-Mental State Exam (MMSE) and Alzheimer’s Disease Assessment Scale (ADAS-cog) scores improved significantly after 12 weeks of tPBM and intranasal PBM. | tPBM and intranasal PBM applied at home demonstrated the potential of this therapy in a small group of patients with dementia and AD. |
| [293] | Double-blind, placebo-controlled trial on 11 subjects with dementia (age 40–85 yrs.) treated in 28 daily sessions with tPBM with an IR device (1060–1080 nm) that had 1100 LEDs set in 15 arrays of 70 LEDs/matrix, pulsed at 10 Hz with a duty cycle of 50%, for a time of 6 min/day. | Patients were evaluated by a mini mental state examination (MMSE), quantitative EEG (QEEG) and ADAS-cog before and 3 days after the completion of treatment. | The results show a slight improvement in executive functioning; clock drawing, immediate recall, praxis memory, visual attention and task switching, as well as improved EEG amplitude and connectivity measures. | As a small pilot clinical trial using tNIR to increase mitochondrial ATP and induce neuronal plasticity, it did not reach statistical significance due to the short duration of therapy and small number of participants. |
| [294] | Randomized controlled trial on 21 subjects divided into two groups: 10 received tPBM twice a week in the frontal region, bilaterally via near-infrared (NIR) light-emitting diodes (LEDs) for 8 weeks), and 11 received sham tPBM. | 28 LEDs [823 nm, CW; 28.7 × 2 cm2; 36.2 mW/cm2; up to 65.2 J/cm2; 20–30 min/session. Safety and efficacy were assessed using the modified Hamilton Depression Rating Scale (HAM-D17). | The study provided preliminary evidence for moderate to high antidepressant efficacy, as tested by the HAM-D17 total score, compared to the control group; tPBM was well tolerated, no serious adverse events. | tPBM with NIR light had a moderate to high antidepressant effect on the HAM-D17 scale. |
| [295] | 30 older adults (≥60 years) without dementia were randomly assigned to two groups. tPBM device contained 9 R diodes of 633 nm wavelength and 52 NIR diodes of 870 nm, incorporated in 3 separate LED cluster heads (633 nm and 870 nm), with a total surface of 22.48 cm2; total power of 999 mW; power density of 44.4 mW/cm2 and CW emission. The tPBM group received the dose of 20 J/cm2, in 7.5 min/session, with a total energy dose of 1349 J, applied to both sides of the frontal region and the posterior midline. | The participants performed cognitive performance tests of frontal function (modified Eriksen flanker test and category fluency tests) before and after real or sham tPBM. The investigated parameters included: (1) CDRS, which estimates the level of global cognitive functioning. (2) CGDS which measures the level of depressive symptoms. (3) Beck Anxiety Inventory (BAI), which measures the level of anxiety symptoms; and (4) the Hong Kong List Learning Test (HKLLT). | tPBM significantly improved the action selection, inhibition ability, and mental flexibility after procedures vs. before tPBM, compared to placebo group. | tPBM could be used as a potential neuroprotective agent for preserving or repairing cognitive function in older adults, in a safe and cost-effective manner. |
| [296] | 15 subjects (mean age 30–14 years; 67% women) suffering from generalized anxiety disorder (GAD) participated in an open-label 8-week study. Each participant self-administered t-PBM daily, for 20 min (CW; 830 nm; mean irradiance 30 mW/cm2; mean fluence 36 J/cm2; total energy delivered per session 2.9 kJ total output power; 2.4 W) on the forehead (total area 80 cm2) with an LED-cluster headband. | The monitored parameters included: the structured interview guide for The Hamilton Anxiety Scale (SIGH-A), Clinical Global Impressions-Severity (CGI-S) and—Improvement (CGI-I) subscales and the Pittsburgh Sleep Quality Index (PSQI). | tPBM had a significant effect in reducing the level of anxiety, with relatively few, mostly mild, and transient side effects. | tPBM could be an alternative therapy for patients with anxiety unresponsive to drugs or psychotherapy. |
| [297] | 34 healthy adults (16 males, 18 females; average age: 31) were included in a double-blind randomized controlled study: 18 participants (9 male, 9 female) received transcranial infrared laser stimulation (TILS) and completed all tasks, performing the cognitive tasks before and after TILS, with concomitant fNIRS recordings, to reflect the hemodynamic effects of TILS on cognitive performance. 16 participants (7 male, 9 female) were matched blind as sham controls (TILS with light off). | Collimated laser diode: 1064 nm; CW mode; average radiant power: 3400 mW; irradiance 250 mW/cm2; beam spot size at forehead target 13.6 cm2; exposure duration: 480 s; radiant exposure: 120 J/cm2; radiant energy: 1632 J; number of points irradiated: one, non-contact; one session in 8 min. Performance on the psychomotor vigilance task (PVT) and the delayed match-to-sample task (DMS) were measured pre- and post-TILS. Functional near-infrared spectroscopy (fNIRS) was used to measure hemodynamics: concentration changes in oxygenated and deoxygenated hemoglobin, total hemoglobin, and differential effects. | fNIRS showed highly significant effects on prefrontal oxygenation during cognitive enhancement post-TILS. | Authors considered their study to be the first demonstration that cognitive enhancement by TILS is associated with cerebrovascular oxygenation of the prefrontal cortex. |
| [298] | 22 elderly adults with mild cognitive impairment (MCI) were recruited through an online advertisement and divided into two groups. Inclusion criteria were no known history of head injury or epilepsy, psychological and/or neuropsychological disorders, or memory and/or other cognitive problem(s). They received tPBM in a single real or sham session. tPBM was administered to the forehead of each patient in the experimental and control group, respectively. For tPBM, a device with 16 probes, 9 LEDs with a wavelength of 810 nm, CW, irradiation power of 20 mW/cm2 was used, which was applied for 350 s, with a fluence of 7 J/cm2. | All subjects performed a visual memory test before and after tPBM measured with functional near-infrared spectroscopy (fNIRS). | tPBM improved the visual memory performance and decreased hemodynamic response during the tasks. tPBM may reduce the cognitive efforts needed to complete tasks that require high memory loads, and thus improved the cognitive performance. | tPBM can improve the cognitive performance of persons with MCI. |
| [299] | 33 young healthy adults (16 males), with mean age of 25.24 years (SD = 8.86 years) were recruited and randomly assigned to control and experimental groups. A single PNM stimulation was applied to the forehead in the experimental group, while a sham PNM for the control group. PNM was performed with a helmet device on the participant’s forehead containing 5 LED clusters each with a spot area of 1 cm2, the wavelength of 810 nm, a power of 20 mW/cm2, an energy density of 7 J/cm2 in 350 s. | Before and after the stimulation, all participants performed an n-back task with 0-and 3-back conditions to assess their working memory function, and the hemodynamic responses during the tasks were measured by fNIRS. The investigated parameters included: verbal working memory ability (HKLLT); visual working memory (Rey–O); BAI; Changes in oxy-Hb and deoxy-Hb were recorded using a 16-channel fNIRS recording arranged in an array on each participant’s forehead. | Visual and verbal memory skills assessed by Rey-O were significantly correlated with oxy-Hb changes. Subjects receiving PNM had a significant improvement in visual memory performance and a reduced hemodynamic response measured by fNIRS during the visual memory task. | PNM may reduce the cognitive efforts needed to complete tasks with high memory loads. If an individual exerts less effort in performing a cognitive task after receiving a single PNM session, the level of oxy-Hb during that cognitive task will be reduced accordingly. |
| [300] | 35 healthy participants over the age of 45 were recruited over two years, using age-matched participants (active group mean of age 57 ± 10 years; placebo group mean age of 57 ± 8 years). 27 participants completed the study. tPBM was performed at home for 6 min, 2 times a day. The helmet device was composed of 14 air cooled LED panel arrays with a wavelength of 1068 nm and a total average optical power output of 3.8 watts. | Computerized assessment of cognitive and motor activities was performed with the FDA-approved Automated Neuropsychological Assessment Metrics (ANAM) tool. | The results demonstrated a significant improvement in motor function, memory performance and processing speed compared to the placebo group. No adverse effects were reported. | tPBM may be the new method for improving memory in middle-aged people. |
| [301] | A single-blind, sham-controlled pilot study investigated the effect of continuous (c-tPBM), pulsed (p-tPBM), and sham (s-tPBM) transcranial photobiomodulation on EEG oscillations and CBF using diffuse correlation spectroscopy (DCS) for a sample of ten healthy subjects (6 F/4 M; mean age 28.6 ± 12.9 years). A NIR laser (830 nm; 54.8 mW/cm2; 65.8 J/cm2; 2.3 kJ) was used for c-tPBM and another for p-tPBM (830 nm; 10 Hz; 54.8 mW/cm2; 33%; 21.7 J/cm2); 0.8 kJ) were applied concurrently to the frontal areas by four LED clusters. | Simultaneous recordings of EEG and DCS were performed weekly before, during and after each tPBM session, as subjects rested (with no cognitive task). EEG was also recorded while participants performed a working memory (2-back) task: once at baseline, before the c-tPBM session, and after each tPBM session. | Use of c-tPBM significantly boosted gamma and beta EEG spectral powers in eyes-open recordings, and gamma power in eyes-closed recordings, with a widespread increase over frontal-central scalp regions. No significant effects of tPBM on CBF were found compared to sham. | The study results support the dose-dependent neuromodulatory effect of tPBM with NIR. |
| [302] | 60 subjects (aged 50 to 85 years) diagnosed with mild to moderate AD/Alzheimer’s disease-related dementias (ADRD) and their primary caregivers were enrolled in a randomized, double-blind, controlled study, at a 2:1 ratio to the active arm or the control arm (sham). Subjects received either an active wearable PBM unit or a sham wearable unit to be used at home twice a day for six minutes, for eight consecutive weeks. tPBM device contained 12 LED modules covering the skull and two retractable modules to provide intraocular stimulation. Each skull module had 70 LEDs and each eye module had 14 LEDs. The active PBM device emitted NIR light with a wavelength of 1060–1080 nm, 15,000 mW, 23.1 mW/cm2 irradiance and for a treatment area of ~650 cm2. | 2 neuropsychological assessments were conducted 8 weeks apart. Evaluation of cognitive function was carried out through: MMSE—which evaluates concentration, orientation, language, attention, memory and visual-spatial function; the clock drawing test (CDT); clock copy test (CPT); Logical Memory Test—Immediate Recall (LMT-I); Logical Memory Test—Delayed Recall (LMT-II); The route making test A; Trail Making Test B; Boston Naming Test (BNT), WAIS-R Digit Symbol Substitution Test. | The 39 randomized subjects in the active arm who remained in the study reported that their energy and mood increased, anxiety decreased, and they had a greater ability to participate physically and mentally in daily activities. | At the end of the study (8 weeks), all subjects remaining in the active arm, both men and women, showed better cognitive performance than those in the control arm. |
| [303] | 60 subjects (of whom 57 completed the study) with mild to moderate dementia were included in a placebo controlled, randomized, double-blinded trial for active treatment with low power NIR light radiation for 6 min twice a day for 8 consecutive weeks. Active and simulated headsets had 12 cranial modules with 70 LEDs/module and 2 foldable eye modules with 14 LEDs/module. The devices issued NIR light at the wavelength of 1060–1080 nm and power of 15,000 mW, the power density of 23.1 mW/cm2, ~650 cm2 per treatment area. | Neuropsychological monitoring was performed by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) test, MMSE, ADAS-cog, CDT, auditory-immediate verbal learning test (A.V.L.T.-1 and A.V.L.T.-2), digit span forward and backward (DSF and DSB), trail making tests A and B and WAIS-R test. | The results showed that this treatment improved cognitive functions, logical memory, auditory verbal learning, mood, sleep duration and daily routine energy in patients with dementia. | tPBM has confirmed the beneficial role in improving the quality of life and self-independence of patients with dementia, reducing the burden on family caregivers. tPBM had no local or systemic adverse effects. Much more studies are needed for the routine application of tPBM. |
| [304] | In a placebo-controlled clinical trial, 60 elderly patients with anemia and mild cognitive dysfunction received intranasal and transcutaneous radial artery PBM (tc-RA-PBM) with a 650-nm clock laser, acupuncture, and moderate-intensity aerobic exercise for 12 weeks. | Monitored parameters: Hb level, cognition by the Montreal Cognitive Assessment Scale (MoCa—B basic), Quality of Life for Alzheimer’s Disease scale and Berg Balance scale scores together, body mass index (BMI) and waist-to-hip ratio (WHR). | PBM showed more significant results compared to the control group in all the measured outcomes. | Intranasal PBM combined with wrist acupuncture and moderate-intensity aerobic exercise might be more effective in improving cognitive function and quality of life in AD patients. |
| [305] | 68 healthy subjects aged 18 to 85 years were included in a randomized, sham-controlled trial. Broadband near-infrared spectroscopy was used for the noninvasive quantification of bilateral cortical changes in oxidized cytochrome-c-oxidase and hemoglobin oxygenation before, during and after 1064-nm PBM (NIR-laser, area: 13.6 cm2, power density: 250 mW/cm2) or sham stimulation of the right anterior prefrontal cortex (Brodmann Area 10). | Montreal Cognitive Assessment (MoCA) measured global cognitive functioning. A non-invasive broadband NIRS (bbNIRS) system was customized to measure the concentration of oxidized CCO (Δ[CCO]), oxygenated hemoglobin (Δ[HbO]) and deoxygenated hemoglobin (Δ[Hb]) in the prefrontal cortex (PFC). | Results showed a significant increase in Δ[CCO] during laser stimulation, followed by a significant post-stimulation increase in Δ[HbO and a decrease in Δ[Hb]. No adverse effects of tPBM were found. | The findings support the use of tPBM for cerebral oxygenation and attenuating the age-related decline of mitochondrial respiration. |
| [306] | 54 subjects with major depressive disorder (MDD) were included in a 2-site, double-blind, sham-controlled study, conducted for adjunct tPBM in NIR (830 nm; CW; 35.8 cm2 treatment area; 54.8 mW/cm2 irradiance; 65.8 J/cm2 fluence, 20 min/session; ~2 W total power; 2.3 kJ total energy per session), delivered to the prefrontal cortex, bilaterally, twice a week for 6 weeks. 18 non-responders to sham in phase 1 (6 weeks) were re-randomized in phase 2. | Patients were assessed using the Hamilton Depression Rating Scale [HDRS-17] and the Quick Inventory of Depressive Symptomatology-Clinician Rating [QIDS-C] score. | In the primary outcome, results showed decreases in depression severity on the HDRS-17 scale and QIDS-C scores. | This study suggests the efficacy of tPBM for patients with MDD; but cannot specify the optimal effective dose. |
| [307] | A case study for an elderly person with a Self-Administered Gerocognitive Exam (SAGE) score indicating memory and thinking disorder. tPBM was administered by a 4-clusters of 3 IR LEDs (810 nm) and 4 levels of power. Stimulations were performed over a period of 35 days at a frequency of 10 Hz. In the first week, 3 sessions were performed at power level 2, then five sessions per week at power level 3, producing a power density of 4.2, respectively 12.7 mW/cm2 for each of the 3 clusters of LEDs. | EEG recorded for 10 min before tPBM in two conditions with eyes open and eyes closed for 5 min each; EEG during PBM and 10 min after stimulation. | PBM could have positive effects on brain activity in the theta and alpha bands for older people with memory and thinking disorders. | PBM has positive effects on brain activity, measured as improvement in power spectrum and connectivity in the theta and alpha bands for older people with memory and thinking disorders. |
| [308] | 4 Case Studies with dementia (two with mild to moderate dementia and two with more advanced symptoms), received tPBM at home. A high-powered super-pulsed laser with 5–905 nm (maximum 200 mW) and 4–660 nm (75 mW -max. 100 mW) diodes was used. Patients were treated three times over a five-day period. The energy delivered per site was 144 J, in 6 areas: four areas on the pre-frontal cortex and two areas on the mid-brain. The total energy delivered over all six sites was 864 J. | Response to tPBM was assessed by MMSE, except for cases with advanced dementia. | Results suggest that tPBM with a high-powered super-pulsed laser applied for three or four eight-minute treatments over a 5–7-day period when using super-pulsing technology could significantly improve cases of moderate and advanced dementia. | Super-pulsed laser devices with higher power could provide improvements in a shorter period of time in AD and dementia. This non-invasive, non-pharmaceutical, and safe treatment approach should be more widely adopted. |
| [309] | In a tPBM study (with a laser of 1064-nm or sham), the EEG data sets were recorded and analyzed from a total of 44 healthy human subjects on a 64-channel EEG before, during, and after 8-min, on the right-forehead tPBM application, and the data were processed with a novel methodology by combining group singular value decomposition (gSVD) with the exact low-resolution brain electromagnetic tomography (eLORETA), implemented and performed on the 64-channel noise-free EEG time series. The gSVD + eLORETA algorithm produced gSVD-derived principal components (PCs) projected in the 2D sensor and 3D source domain/space. Finally, baseline-normalized power changes of each EEG brain network in each EEG frequency band (delta, theta, alpha, beta and gamma) were quantified during the first 4-min, second 4-min, and post tPBM/sham periods, followed by comparisons of frequency-specific power changes between tPBM and sham conditions. | tPBM was conducted with a 1064-nm laser (illumination area of 13.6 cm2, power of 3.5 W, laser aperture diameter of ∼4.16 cm). Active optical energy (or dose) was 3.5 W × 480 s = 1680 J and energy density (or fluence) delivered to the forehead was 1680 J/(13.6 cm2) = 123.5 J/cm2, respectively. Active power density (irradiance) was 3.5 W/(13.6 cm2) = 257.4 mW/cm2. Power used for sham was set to be 0.1 W. | Results highlighted that 1064-nm tPBM applied on right-forehead, could neuromodulate the alpha and gamma powers on several of the gSVD-derived EEG brain networks, i.e., the well-defined (MRI-derived): default-mode network, frontalparietal network, and executive control network. | This study clearly proved mechanistic associations or causal effects of tPBM and modulated brain networks versus improved cognition outcomes. |
| [310] | Effect of PBM on regression of dementia and cognitive impairment in various AD stages was studied on 97 patients with previously diagnosed AD, aged 34–80 (mean age 67.5), divided into two groups: Test Group (G1)—48 patients, treated with Transcatheter Intracerebral PBM (PBMT), and Control Group (G2)—49 patients who underwent conservative treatment with Memantine and Rivastigmine. PBMT was administered with a 632.8 nm laser device; laser output power of 25–45 mW; fiber output power of 24–44 mW; stream duration of 1200–2400 s; diameter of the laser beam in the vessel of 1–2 mm, average dose of 29–106 J. | Examinations of patients were carried out as follows: the clinical severity of dementia was assessed using CDR, the cognitive impairment using MMSE, cerebral blood flow and cerebral microcirculation using SG in static and dynamic modes; cerebral perfusion blood filling with REG, and intracerebral vascular and capillary bed was evaluated by MUGA. Cerebral structural and morphological changes were assessed using CT and MRI performed upon the patients’ admission, then, at an interval of 6–12 months. Examinations were performed using the digital image processing program ATAA and digital morphometric scale TDR. | As a result of PBMT, involutive changes were reduced, the normal structure of the cerebral tissue was restored, and the volumes of the temporal and frontoparietal lobes increased. Decreased dementia severity and restoration of cognitive functions in AD patients were found in G1. Conservative treatment in the control group did not stimulate regenerative processes and did not improve microcirculation. | PBMT is an effective, physiologically based method of stimulating cerebral angiogenesis and neurogenesis. Tissue regeneration in G1 led to an increase in temporal and frontoparietal volume, a stable decrease in the level of dementia, restoring cognitive functions and improving patients’ quality of life. This clinical effect was maintained for many years. Treatment with Memantine and Rivastigmine was not effective. |
| [311] | Case studies. Three older adults with non-amnestic MCI received 18 sessions of tPBM stimulation over 9 weeks (i.e., twice per week). A device with 9 individual LED nodes of 1 cm2 size, were placed cranially in the frontal area. Each LED emits 810 nm light, at an irradiance of 20 mW/cm2, for 350 s, with a fluence of 7 J/cm2, total surface area of 9 cm2, energy delivered per session was 189 J and the total energy delivered for the 18 sessions was 3402 J. | Patients were assessed using CDRS, CDR, FAQ, HKLLT, Rey-O, CGDS-SF, GAS-10, CFT. | tPBM applied to the frontal lobe area during 18 sessions improved cognitive functions, depressive and anxiety symptoms in three elderly adults with MCI. | This study provided preliminary support for tPBM as a non-invasive intervention to improve cognitive functions and mental health in elderly people with MCI. Further investigation through larger randomized placebo-controlled studies is needed to confirm tPBM potential. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ailioaie, L.M.; Ailioaie, C.; Litscher, G. Photobiomodulation in Alzheimer’s Disease—A Complementary Method to State-of-the-Art Pharmaceutical Formulations and Nanomedicine? Pharmaceutics 2023, 15, 916. https://doi.org/10.3390/pharmaceutics15030916
Ailioaie LM, Ailioaie C, Litscher G. Photobiomodulation in Alzheimer’s Disease—A Complementary Method to State-of-the-Art Pharmaceutical Formulations and Nanomedicine? Pharmaceutics. 2023; 15(3):916. https://doi.org/10.3390/pharmaceutics15030916
Chicago/Turabian StyleAilioaie, Laura Marinela, Constantin Ailioaie, and Gerhard Litscher. 2023. "Photobiomodulation in Alzheimer’s Disease—A Complementary Method to State-of-the-Art Pharmaceutical Formulations and Nanomedicine?" Pharmaceutics 15, no. 3: 916. https://doi.org/10.3390/pharmaceutics15030916
APA StyleAilioaie, L. M., Ailioaie, C., & Litscher, G. (2023). Photobiomodulation in Alzheimer’s Disease—A Complementary Method to State-of-the-Art Pharmaceutical Formulations and Nanomedicine? Pharmaceutics, 15(3), 916. https://doi.org/10.3390/pharmaceutics15030916