Breast Milk Content of Vitamin A and E from Early- to Mid-Lactation Is Affected by Inadequate Dietary Intake in Brazilian Adult Women

 and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Experimental Design and Recruitment of Volunteers
2.2. Data Collection and Qualification of Lactation Practices
2.3. Assessment of Dietary Intake
2.4. Collection and Processing of Biological Samples
2.5. Determination of Hematocrit and Hemoglobin, and Triglycerides and Cholesterol in Blood
2.6. Breast Milk Macronutrient Composition
2.7. Determination of Retinol, Carotenoids and Tocopherols by HPLC in Breast Milk, Whole Blood Serum, and Lipoprotein Fractions
2.8. Statistical Analyses
3. Results
3.1. General Characteristics of Lactating Women
3.2. Dietary Intake of Vitamin A and E Were Inadequate throughout Lactation
3.3. Serum Vitamin A and E Were Not Associated with Their Changes in Breast Milk Concentration throughout Lactation
3.4. Breast Milk Concentration of Fat-Soluble Vitamins from Early- to Mid-Lactation Is Associated with Dietary Vitamin A, Serum β-Carotene and Tocopherols
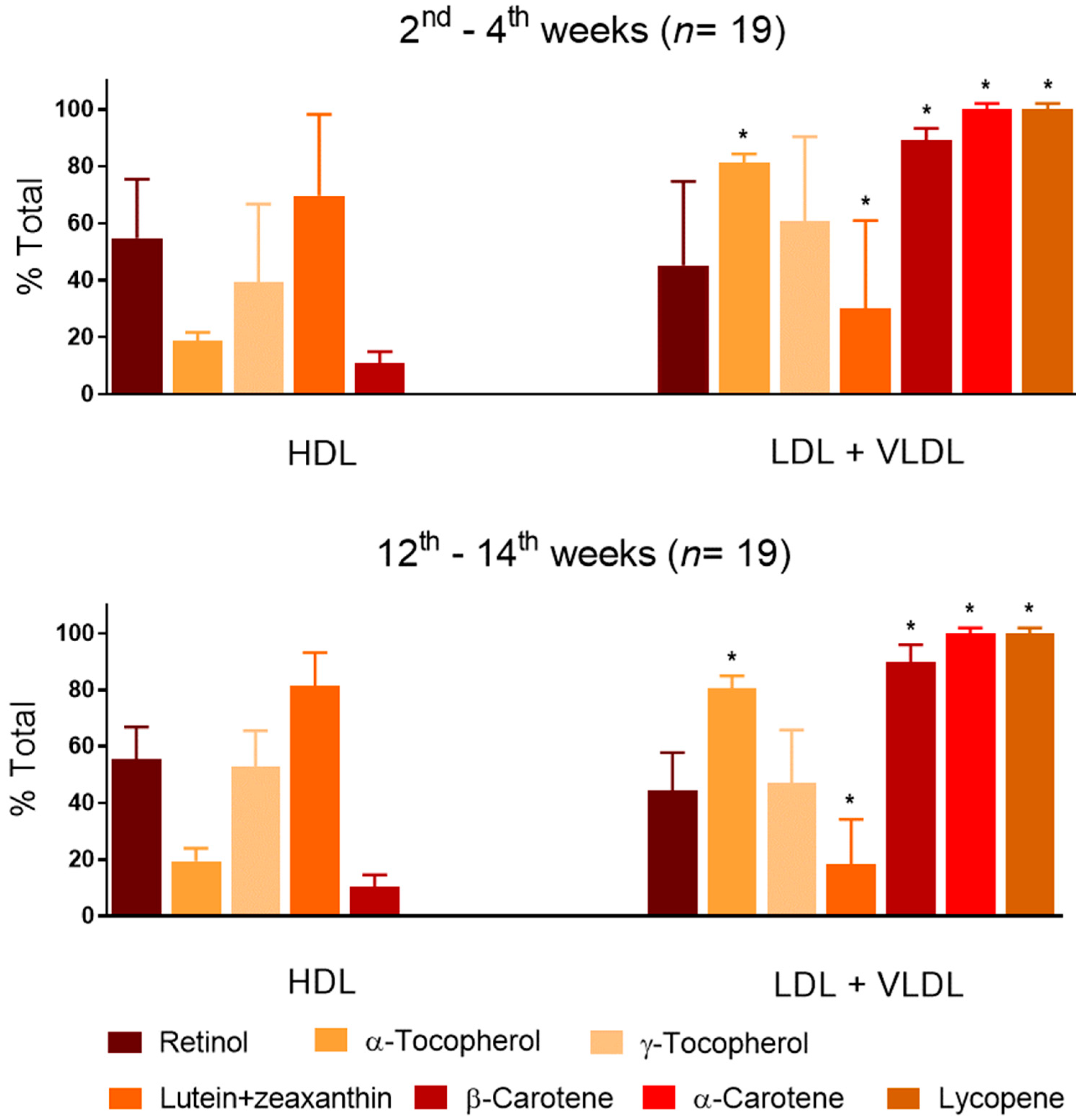
3.5. Vitamin A and E and Carotenoids Distributed Differently in Lipoprotein Fractions during Lactation
4. Discussion
4.1. Dietary Intake, Nutritional Status and Milk Transfer of Vitamin A and E, and Carotenoids
4.2. Vitamin A and E, and Carotenoids Distribution among Serum Lipoprotein Fractions Was Stable from Early- to Mid-Lactation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005; WHO: Geneva, Switzerland, 2009; pp. 9–18. [Google Scholar]
- Ribeiro, K.D.S.; Lima, M.S.R.; Medeiros, J.F.P.; Rebouças, A.S.; Dantas, R.C.S.; Bezerra, D.S.; Osório, M.M.; Dimenstein, R. Association between maternal vitamin E status and alpha-tocopherol levels in the newborn and colostrum. Matern. Child Nutr. 2016, 12, 801–807. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.Y.; Pundir, S.; Mckenzie, E.; Keijer, J.; Kussmann, M. Maternal circulating vitamin status and colostrum vitamin composition in healthy lactating women—A systematic approach. Nutrients 2018, 28, 687. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.G.C.L.; Rebouças, A.S.; Mendonça, B.M.A.; Silva, D.C.N.; Dimenstein, R.; Ribeiro, K.D.S. Relationship between the dietary intake, serum, and breast milk concentrations of vitamin A and vitamin E in a cohort of women over the course of lactation. Matern. Child Nutr. 2019, 22, e12772. [Google Scholar] [CrossRef] [PubMed]
- Grilo, E.C.; Medeiros, W.F.; Silva, A.G.A.; Gurgel, C.S.S.; Ramalho, H.M.M.; Dimenstein, R. Maternal supplementation with a megadose of vitamin A reduces colostrum level of α-tocopherol: A randomized controlled trial. J. Hum. Nutr. Diet. 2016, 29, 652–661. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Harttig, U.; Haubrock, J.; Knüppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Sartorelli, D.S.; Barbieri, P.; Perdona, G.C. Fried food intake estimated by the multiple source method is associated with gestational weight gain. Nutr. Res. 2014, 34, 667–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 25. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/nutrient-data-laboratory/docs/sr25-home-page/ (accessed on 20 July 2016).
- University of Campinas (UNICAMP)—Core Centre for Research in Food (NEPA). Brazilian Food Composition Table, Taco, 4th ed.; NEPA/UNICAMP: Campinas, Brazil, 2011; pp. 1–161. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes Research Synthesis: Workshop Summary; National Academy Press: Washington, DC, USA, 2007; pp. 127–150. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids; National Academy Press: Washington, DC, USA, 2000; pp. 186–283. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academy Press: Washington, DC, USA, 2001; pp. 82–161. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes—Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academy Press: Washington, DC, USA, 2002; pp. 936–967. [Google Scholar]
- Lopes-Virella, M.F.; Stone, P.; Ellis, S.; Colwell, J.A. Cholesterol determination in high-density lipoproteins separated by three different methods. Clin. Chem. 1977, 23, 882–884. [Google Scholar] [PubMed]
- Lucas, A.; Gibbs, J.A.; Lyster, R.L.; Baum, J.D. Creamatocrit: Simple clinical technique for estimating fat concentration and energy value of human milk. Br. Med. J. 1978, 1, 1018–1020. [Google Scholar] [CrossRef]
- Perry, N.A.; Doan, F.J. A picric acid method for the simultaneous determination of lactose and sucrose in dairy products. J. Dairy Sci. 1950, 33, 176–185. [Google Scholar] [CrossRef]
- Costa, T.H.M.; Dorea, J.G. Concentration of fat, protein, lactose and energy in milk of mothers using hormonal contraceptives. Ann. Trop. Pediatr. 1992, 12, 203–209. [Google Scholar] [CrossRef]
- Lowry, O.H.; Rosebrough, N.; Farr, A.L.; Randall, R.J. Protein measurement with the Folin phenol reagent. J. Biol. Chem. 1951, 193, 265–275. [Google Scholar] [PubMed]
- Trugo, N.M.F.; Donangelo, C.M.; Koury, J.C.; Silva, M.I.; Freitas, L.A. Concentration and distribution pattern of selected micronutrients in preterm and term milk from urban Brazilian mothers during early lactation. Eur. J. Clin. Nutr. 1988, 42, 497–507. [Google Scholar] [PubMed]
- Meneses, F.; Trugo, N.M.F. Retinol, β-carotene, and lutein+zeaxanthin in the milk of Brazilian nursing women: Associations with plasma concentrations and influences of maternal characteristics. Nutr. Res. 2005, 25, 443–451. [Google Scholar] [CrossRef]
- Hass, D.; Keller, H.E.; Oberlin, B.; Bonfanti, R.; Schüep, W. Simultaneous determination of retinol, tocopherols, carotenes and lycopene in plasma by means of High-Performance Liquid-Chromatography on reversed phase. Int. J. Vitam. Nutr. Res. 1991, 61, 232–238. [Google Scholar]
- Liu, Y.; Xu, M.J.; Canfield, L.M. Enzymatic hydrolysis, extraction, and quantitation of retinol and major carotenoids in mature human milk. J. Nutr. Biochem. 1998, 9, 178–183. [Google Scholar] [CrossRef]
- Silva, L.O.; Castelo-Branco, V.N.; Carvalho, A.G.A.; Monteiro, M.C.; Perrone, D.; Torres, A.G. Ethanol extraction renders a phenolic compounds-enriched and highly stable jussara fruit (Euterpe edulis M.) oil. Eur. J. Lipid Sci. Technol. 2017, 119, e201700200. [Google Scholar] [CrossRef]
- Rodriguez-Amaya, D.B.; Kimura, M. Harvest Plus Handbook for Carotenoid Analysis; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2004; pp. 1–57. [Google Scholar]
- World Health Organization (WHO). Prevention and Control of Iron Deficiency Anaemia in Women and Children; United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 1999; pp. 17–30. [Google Scholar]
- Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Joint FAO/WHO Expert Consultation on Human Vitamin and Mineral Requirements (FAO/WHO). Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; WHO: Geneva, Switzerland, 2004; pp. 1–362. [Google Scholar]
- Deminice, T.M.M.; Ferraz, I.S.; Monteiro, J.P.; Jordão, A.A.; Ambrósio, L.M.C.S.; Almeida, C.A.N. Vitamin A intake of Brazilian mothers and retinol concentrations in maternal blood, human milk, and the umbilical cord. Nutr. Res. Pract. 2018, 46, 1555–1569. [Google Scholar] [CrossRef]
- Lira, L.Q.; De Souza, A.F.; Amâncio, A.M.; Bezerra, C.G.; Pimentel, J.B.; Moia, M.N.; Dimenstein, R. Retinol and betacarotene status in mother-infant dyads and associations between them. Ann. Nutr. Metab. 2018, 72, 50–56. [Google Scholar] [CrossRef]
- Kim, H.; Jung, B.; Lee, B.; Kim, Y.; Jung, J.A.; Chang, N. Retinol, α-tocopherol, and selected minerals in breast milk of lactating women with full-term infants in South Korea. Nutr. Res. Pract. 2017, 11, 64–69. [Google Scholar] [CrossRef]
- Ministry of Health, Brazil; National Sanitary Surveillance Agency (ANVISA). Resolution RDC Nº 269, Technical Regulation on Recommended Daily Intake (IDR) of Protein, Vitamins and Minerals; ANVISA: Brasilia, DF, Brazil, 2005; pp. 1–6.
- Garretto, D.; Kim, Y.-K.; Quadro, L.; Rhodas, R.R.; Pimentel, V.; Crnosija, N.A.; Nie, L.; Bernstein, P.; Tropper, P.; Neal-Perry, G.S. Vitamin A and β-carotene in pregnant and breastfeeding post-bariatric women in an urban population. J. Perinat. Med. 2019, 47, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhao, X.; Berde, Y.; Low, Y.; Kuchan, M. Milk and plasma lutein and zeaxanthin concentrations in Chinese breast-feeding mother-infant dyads with healthy maternal fruit and vegetable intake. J. Am. Coll. Nutr. 2019, 38, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, M.; Hamulka, J.; Wesolowska, A. Carotenoid content in breastmilk in the 3rd and 6th month of lactation and its associations with maternal dietary intake and anthropometric characteristics. Nutrients 2019, 11, 193. [Google Scholar] [CrossRef] [PubMed]
- Xavier, A.A.O.; Diaz-Salido, E.; Arenilla-Velez, I.; Aguayo-Maldonado, J.; Garrido-Fernandez, J.; Fontecha, J.; Sanchez-Garcia, A.; Perez-Galvez, A. Carotenoid content in human colostrum is associated to preterm/full-term birth condition. Nutrients 2018, 10, 1654. [Google Scholar] [CrossRef] [PubMed]
- Schweigert, F.J.; Bathe, K.; Chen, F.; Büscher, U.; Dudenhausen, J.W. Effect of the stage of lactation in humans on carotenoid levels in milk, blood plasma and plasma lipoprotein fractions. Eur. J. Nutr. 2004, 43, 39–44. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Lactation Period | p | Recommended Value or Range 1 | |
|---|---|---|---|---|
| Early Lactation 2nd–4th Week | Mid-Lactation 12th–14th Week | |||
| Body mass index (kg/m2) | 25.9 ± 4.0 | 25.3 ± 4.2 | 0.068 * | 18–24.9 [6] |
| Hemoglobin (g/dL) | 11.6 ± 1.7 | 12.5± 1.6 | 0.029 * | ≥12.0 [26] |
| Hematocrit (%) | 39.2 ± 3.5 | 37.8 ± 3.5 | 0.131 | ≥36 [26] |
| Triglycerides (mg/dL) | 74.7 ± 21.4 | 57.0 ± 21.2 | 0.007 * | <150 [27] |
| Total cholesterol (mg/dL) | 190.2 ± 41.9 | 182.2 ± 41.0 | 0.219 | <200 [27] |
| LDL-c (mg/dL) | 156.0 ± 44.1 | 146.6 ± 35.9 | 0.164 | 100–129 [27] |
| HDL-c (mg/dL) | 34.2 ± 6.2 | 35.6 ± 9.4 | 0.601 | >60 [27] |
| Energy and Nutrients | Intake (24hR-MSM) | Inadequacy (%) 3 | Nutrient Intake Adequacy | |
|---|---|---|---|---|
| Reference Value (Daily Intake) 4 | Method [Ref.] | |||
| Energy (kcal) | 1577 ± 164 1 | 53 | — | BMI distribution [14] |
| Carbohydrate (en%) | 51.2 ± 7.7 1 | 21 | 160 g 5 | EAR cut-off [14] |
| Protein (en%) | 17.7 ± 3.1 1 | 47 | 1.05 g/kg 5 | EAR cut-off [14] |
| Total lipids (en%) | 31.1 ± 0.52 1 | 26 | 20 to 35 | AMDR [14] |
| Vitamin A (μg RE) | 824.7 ± 21.8 1 | 74 | 900 | EAR cut-off [13] |
| β-Carotene (μg) | 3249 (1408–6707) 2 | — | 3000–6000 [12] | — |
| α-Carotene (μg) | 1053 (56–3712) 2 | — | — | — |
| Lycopene (μg) | 1854 (302–6472) 2 | — | ≥5000 [12] | — |
| Lutein + zeaxanthin (μg) | 2446 (872–4873) 2 | — | — | — |
| Vitamin E (mg) | 4.4 ± 0.9 1 | 100 | 16 | EAR cut-off [12] |
| Vitamin | Serum | Breast Milk | ||||||
|---|---|---|---|---|---|---|---|---|
| Lactation Period | Undernutrition Cut-Off Value | Lactation Period | Inadequacy Cut-Off Value | |||||
| 2nd–4th Week | 12th–14th Week | p | 2nd–4th Week | 12th–14th Week | p | |||
| Retinol | 1.50 ± 0.30 | 1.48 ± 0.31 | 0.913 | 0.7 [28] | 2.3 ± 0.78 | 2.0 ± 0.72 | 0.013 * | 1.05 [1,28] |
| β-Carotene | 0.61 ± 0.07 | 0.59 ± 0.05 | 0.628 | — | 0.17 ± 0.02 | 0.14 ± 0.3 | 0.001 * | — |
| α-Carotene | 0.43 ± 0.09 | 0.44 ± 0.08 | 0.720 | — | 0.04 ± 0.01 | 0.03 ± 0.01 | 0.304 | — |
| Lycopene | 0.20 ± 0.03 | 0.18 ± 0.04 | 0.530 | — | 0.04 ± 0.01 | 0.04 ± 0.00 | 1.000 | — |
| Lutein + zeaxanthin | 0.24 ± 0.04 | 0.23 ± 0.07 | 0.633 | — | 0.07 ± 0.02 | 0.06 ± 0.01 | 0.026 * | — |
| α-Tocopherol | 11.1 ± 1.11 | 10.1 ± 1.23 | 0.089 | 11.6 [12] | 1.29 ± 0.25 | 1.07 ± 0.13 | 0.001 * | 7.4 [28] |
| γ-Tocopherol | 0.76 ± 0.15 | 0.75 ± 0.13 | 0.896 | — | 0.38 ± 0.04 | 0.35 ± 0.04 | 0.436 | — |
| Model N | Dependent Variable Breast Milk 2 | Independent Variables Serum A and Diet B | Coefficients | Weight in the Model 3 | Adj. R 2 | Error (%) 4 | p5 | |
|---|---|---|---|---|---|---|---|---|
| Value | p | |||||||
| Early-Lactation: 2nd–4th Week | ||||||||
| 1 | Retinol | Vitamin A B | 5.33 × 10−3 | <0.0001 | 100% | 94.9 | 9% | <0.0001 |
| 2 | β-Carotene | β-Carotene A | 2.25 × 10−1 | 0.0045 | 63% | 87.7 | 14% | <0.0001 |
| β-Carotene B | 2.52 × 10−5 | 0.0430 | 37% | |||||
| 3 | α-Tocopherol | α-Tocopherol A | 1.24 | <0.0001 | 100% | 96.2 | 18% | <0.0001 |
| Mid-Lactation: 12th–14th Week | ||||||||
| 4 | Retinol | Vitamin A B | 4.79 × 10−3 | <0.0001 | 100% | 94.7 | 14% | <0.0001 |
| 5 | β-Carotene | β-Carotene A | 2.34 × 10−1 | <0.0001 | 100% | 78.4 | 17% | <0.0001 |
| 6 | α-Tocopherol | α-Tocopherol A | 1.03 | <0.0001 | 100% | 97.9 | 12% | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, M.R.; Kamp, F.; Nunes, J.C.; El-Bacha, T.; Torres, A.G. Breast Milk Content of Vitamin A and E from Early- to Mid-Lactation Is Affected by Inadequate Dietary Intake in Brazilian Adult Women. Nutrients 2019, 11, 2025. https://doi.org/10.3390/nu11092025
Machado MR, Kamp F, Nunes JC, El-Bacha T, Torres AG. Breast Milk Content of Vitamin A and E from Early- to Mid-Lactation Is Affected by Inadequate Dietary Intake in Brazilian Adult Women. Nutrients. 2019; 11(9):2025. https://doi.org/10.3390/nu11092025
Chicago/Turabian StyleMachado, Michele R., Fernanda Kamp, Juliana C. Nunes, Tatiana El-Bacha, and Alexandre G. Torres. 2019. "Breast Milk Content of Vitamin A and E from Early- to Mid-Lactation Is Affected by Inadequate Dietary Intake in Brazilian Adult Women" Nutrients 11, no. 9: 2025. https://doi.org/10.3390/nu11092025
APA StyleMachado, M. R., Kamp, F., Nunes, J. C., El-Bacha, T., & Torres, A. G. (2019). Breast Milk Content of Vitamin A and E from Early- to Mid-Lactation Is Affected by Inadequate Dietary Intake in Brazilian Adult Women. Nutrients, 11(9), 2025. https://doi.org/10.3390/nu11092025