Associating Intake Proportion of Carbohydrate, Fat, and Protein with All-Cause Mortality in Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
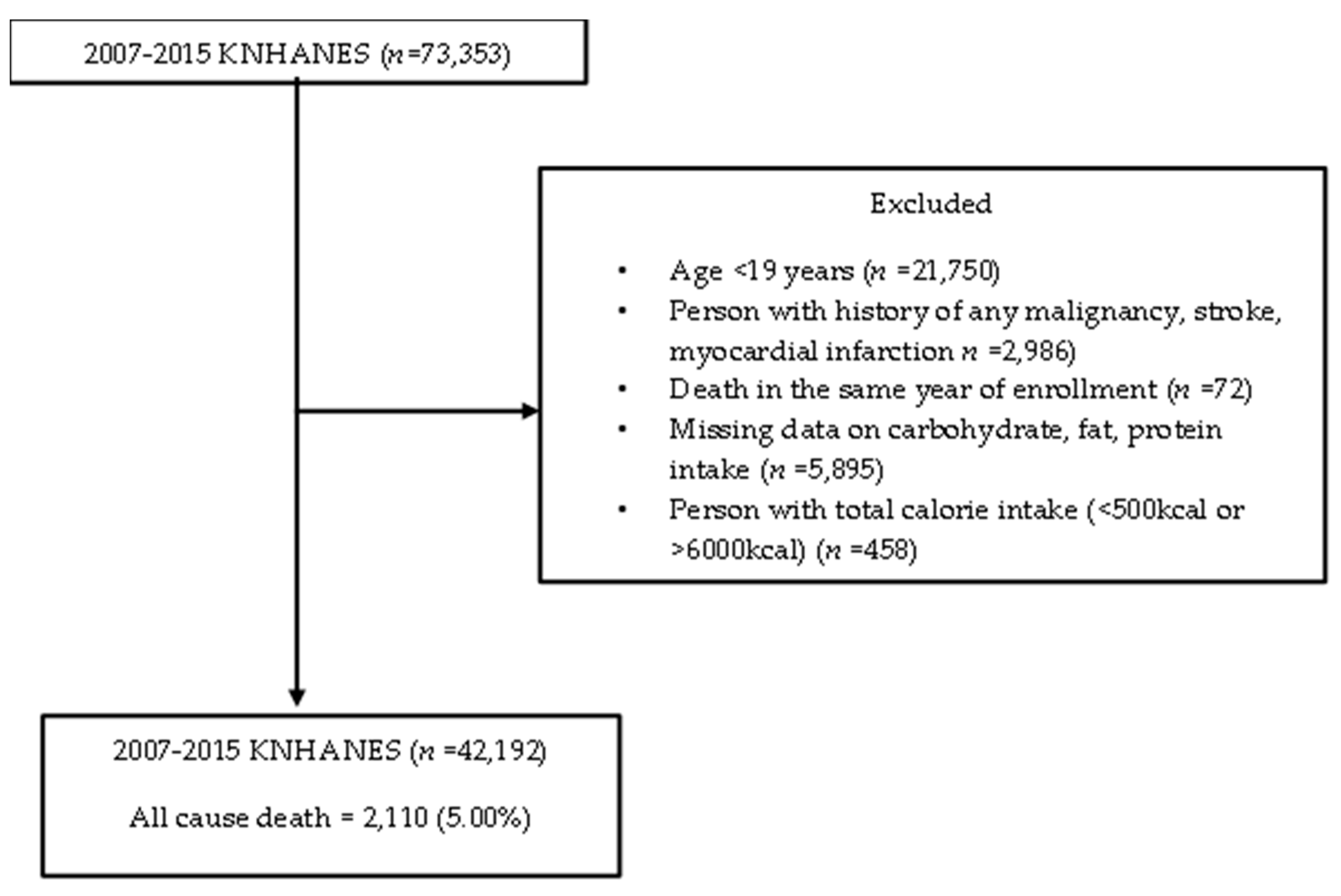
2.1. Study Population
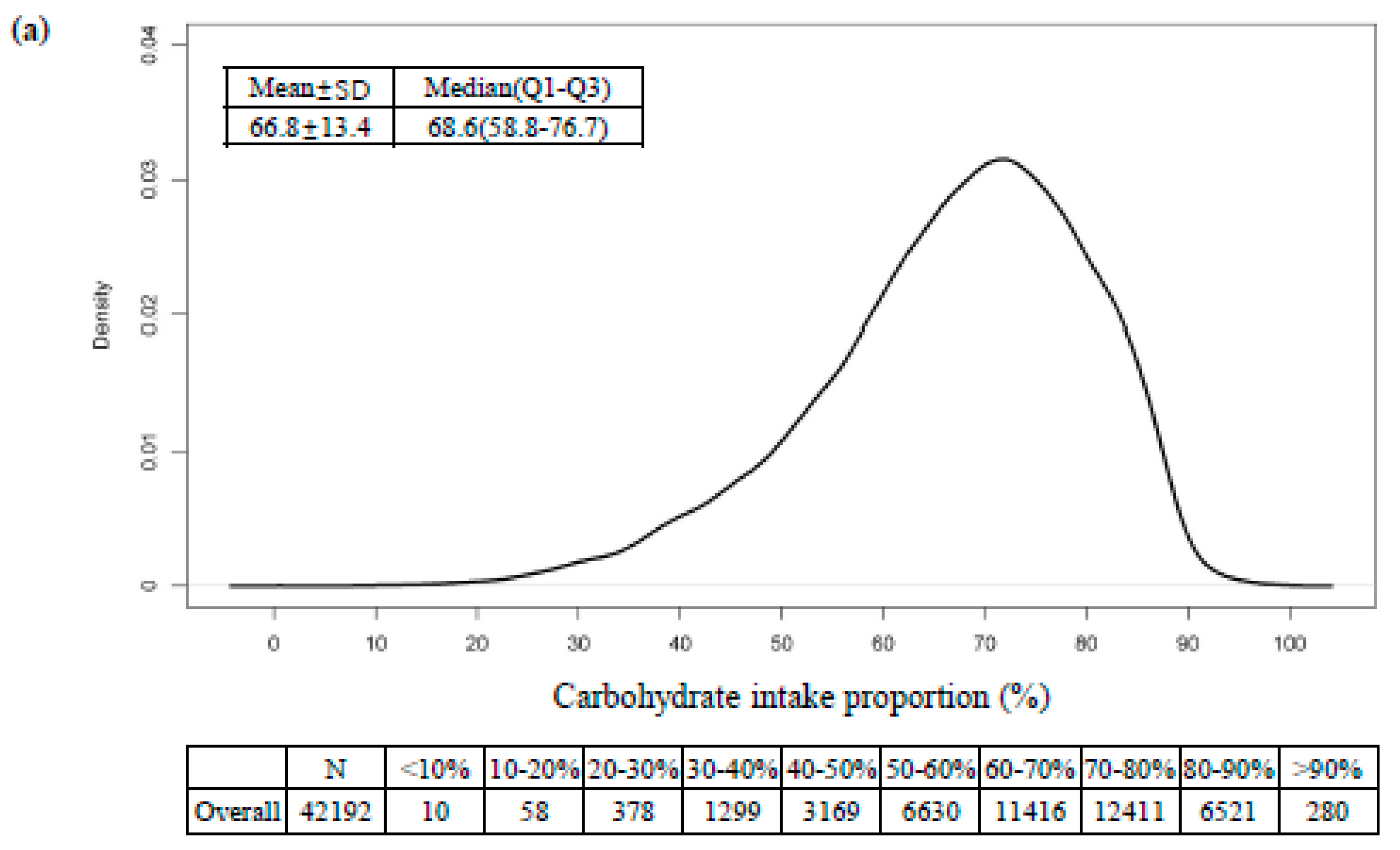
2.2. Assessment of Nutritional Status
2.3. Ascertainment of All-Cause Mortality
2.4. Covariates
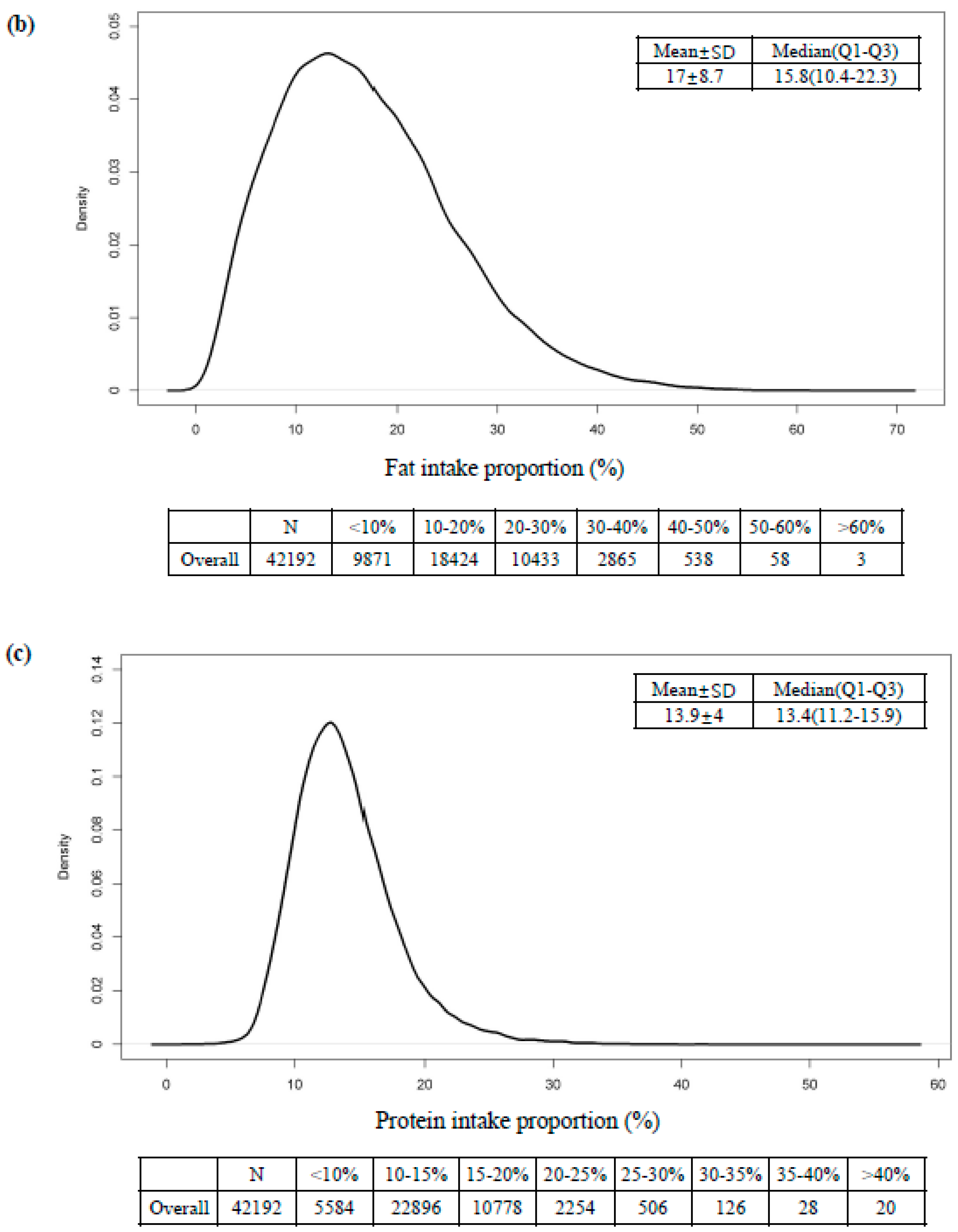
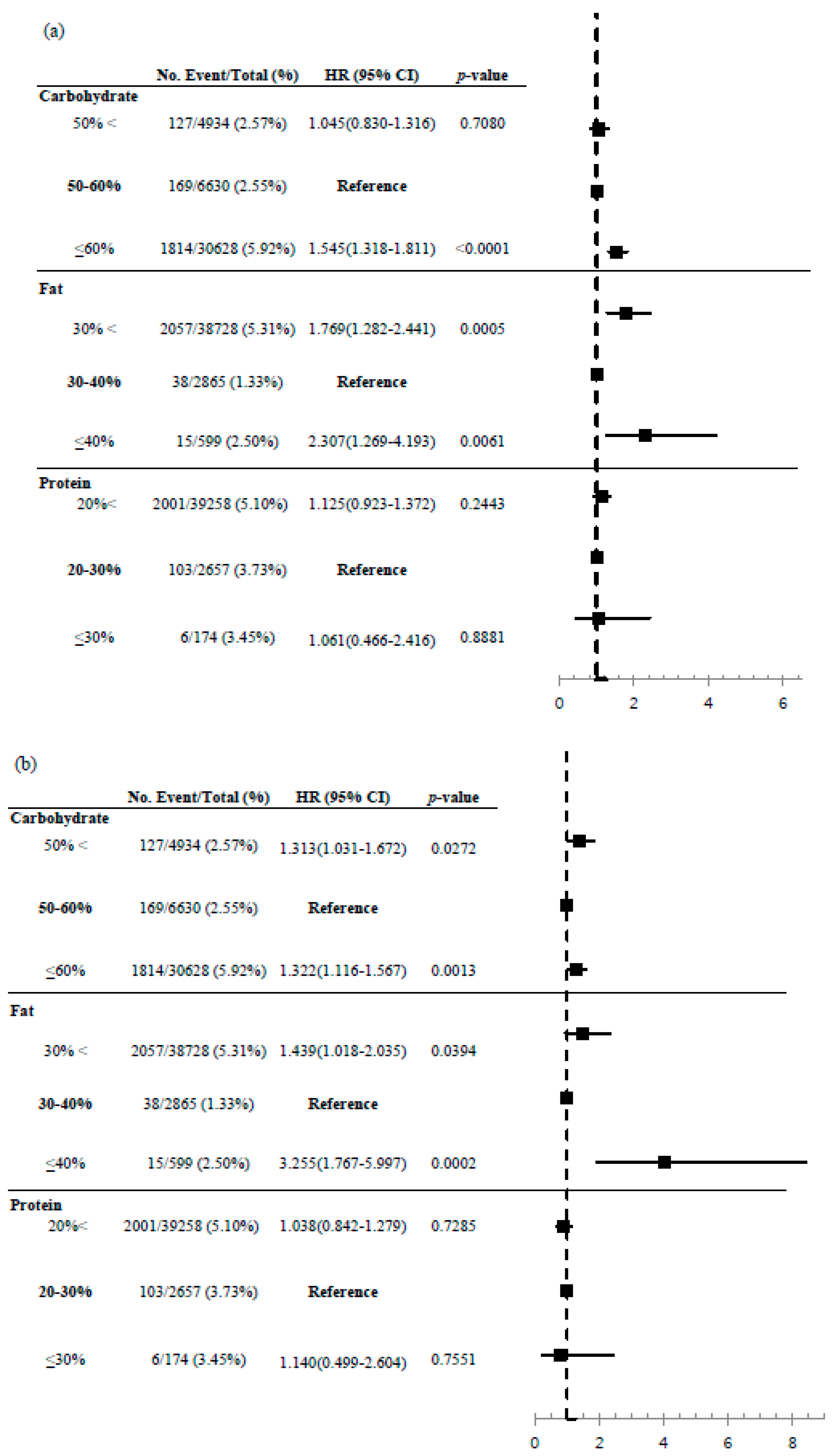
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Carreiro, A.L.; Dhillon, J.; Gordon, S.; Higgins, K.A.; Jacobs, A.G.; McArthur, B.M.; Redan, B.W.; Rivera, R.L.; Schmidt, L.R.; Mattes, R.D. The Macronutrients, Appetite, and Energy Intake. Annu. Rev. Nutr. 2016, 36, 73–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Souza, R.J.; Swain, J.F.; Appel, L.J.; Sacks, F.M. Alternatives for macronutrient intake and chronic disease: A comparison of the OmniHeart diets with popular diets and with dietary recommendations. Am. J. Clin. Nutr. 2008, 88, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, V.J.; Bishop, L.; Charleston, J.; Conlin, P.; Erlinger, T.; Laranjo, N.; McCarron, P.; Miller, E.; Rosner, B.; Swain, J.; et al. Rationale and design of the Optimal Macro-Nutrient Intake Heart Trial to Prevent Heart Disease (OMNI-Heart). Clin. Trials 2005, 2, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Ungvari, Z.; Parrado-Fernandez, C.; Csiszar, A.; De Cabo, R. Mechanisms Underlying Caloric Restriction and Lifespan Regulation: Implications for vascular aging. Circ. Res. 2008, 102, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Masoro, E.J. Role of Hormesis in Life Extension by Caloric Restriction. Dose Response 2006, 5, 163–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattan, S.I. Aging, anti-aging, and hormesis. Mech. Ageing Dev. 2004, 125, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Solon-Biet, S.M.; Mitchell, S.J.; De Cabo, R.; Raubenheimer, D.; Le Couteur, D.G.; Simpson, S.J. Macronutrients and caloric intake in health and longevity. J. Endocrinol. 2015, 226, R17–R28. [Google Scholar] [CrossRef]
- Mair, W.; Piper, M.D.W.; Partridge, L. Calories Do Not Explain Extension of Life Span by Dietary Restriction in Drosophila. PLoS Biol. 2005, 3, e223. [Google Scholar] [CrossRef] [Green Version]
- Solon-Biet, S.M.; McMahon, A.C.; Ballard, J.W.; Ruohonen, K.; Wu, L.E.; Cogger, V.C.; Warren, A.; Huang, X.; Pichaud, N.; Melvin, R.G.; et al. The Ratio of Macronutrients, Not Caloric Intake, Dictates Cardiometabolic Health, Aging, and Longevity in Ad Libitum-Fed Mice. Cell Metab. 2014, 19, 418–430. [Google Scholar] [CrossRef] [Green Version]
- Table, M. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2005; Volume 5. [Google Scholar]
- Buyken, A.E.; Mela, D.J.; Dussort, P.; Johnson, I.T.; Macdonald, I.A.; Stowell, J.D.; Brouns, F. Dietary carbohydrates: A review of international recommendations and the methods used to derive them. Eur. J. Clin. Nutr. 2018, 72, 1625–1643. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health Human Services. US Department of Agriculture 2015–2020 Dietary Guidelines for Americans; US Department of Health Human Services: Washington, DC, USA, 2019. [Google Scholar]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef] [Green Version]
- Seidelmann, S.B.; Claggett, B.; Cheng, S.; Henglin, M.; Shah, A.; Steffen, L.M.; Folsom, A.R.; Rimm, E.B.; Willett, W.C.; Solomon, S.D. Dietary carbohydrate intake and mortality: A prospective cohort study and meta-analysis. Lancet Public Health 2018, 3, e419–e428. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, P.; Zhang, Y.; He, W.; Chen, X.; Chen, J.; He, L.; Mao, L.; Wu, F.; Jiao, J. Dietary Fats in Relation to Total and Cause-Specific Mortality in a Prospective Cohort of 521 120 Individuals with 16 Years of Follow-Up. Circ. Res. 2019, 124, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Moon, S.; Popkin, B.M. The nutrition transition in South Korea. Am. J. Clin. Nutr. 2000, 71, 44–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garralda-Del-Villar, M.; Carlos-Chillerón, S.; Diaz-Gutierrez, J.; Ruiz-Canela, M.; Gea, A.; Martínez-González, M.A.; Bes-Rastrollo, M.; Ruiz-Estigarribia, L.; Kales, S.N.; Fernández-Montero, A. Healthy Lifestyle and Incidence of Metabolic Syndrome in the SUN Cohort. Nutrients 2018, 11, 65. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.D.; Li, Y.; Chiuve, S.E.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Association of Specific Dietary Fats With Total and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1134–1145. [Google Scholar] [CrossRef]
- Ho, F.K.W.; Gray, S.R.; Welsh, P.; Petermann-Rocha, F.; Foster, H.; Waddell, H.; Anderson, J.; Lyall, D.; Sattar, N.; Gill, J.M.R.; et al. Associations of fat and carbohydrate intake with cardiovascular disease and mortality: Prospective cohort study of UK Biobank participants. BMJ 2020, 368, m688. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.-X.; Shen, P. Associations of dietary protein intake with all-cause, cardiovascular disease, and cancer mortality: A systematic review and meta-analysis of cohort studies. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1094–1105. [Google Scholar] [CrossRef]
- Mazidi, M.; Katsiki, N.; Mikhailidis, D.P.; Sattar, N.; Banach, M. Lower carbohydrate diets and all-cause and cause-specific mortality: A population-based cohort study and pooling of prospective studies. Eur. Heart J. 2019, 40, 2870–2879. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Kim, S.; Joung, H. Evidence-based approaches for establishing the 2015 Dietary Reference Intakes for Koreans. Nutr. Res. Pract. 2018, 12, 459–468. [Google Scholar] [CrossRef]
- Lee, Y.J.; Song, S.; Song, Y. High-Carbohydrate Diets and Food Patterns and Their Associations with Metabolic Disease in the Korean Population. Yonsei Med. J. 2018, 59, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, C.F.; Bolick, J.P.; Kris-Etherton, P.M.; Sikand, G.; Aspry, K.E.; Soffer, D.E.; Willard, K.-E.; Maki, K.C. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J. Clin. Lipidol. 2019, 13, 689–711.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PREDIMED Study Investigators; Guasch-Ferré, M.; Babio, N.; Martínez-Gonzalez, M.A.; Corella, D.; Ros, E.; Martín-Peláez, S.; Estruch, R.; Arós, F.; Gómez-Gracia, E.; et al. Dietary fat intake and risk of cardiovascular disease and all-cause mortality in a population at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2015, 102, 1563–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Gonzalez, M.A.; Martin-Calvo, N. Mediterranean diet and life expectancy; beyond olive oil, fruits, and vegetables. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 401–407. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Levine, M.E.; Suarez, J.A.; Brandhorst, S.; Balasubramanian, P.; Cheng, C.-W.; Madia, F.; Fontana, L.; Mirisola, M.G.; Guevara-Aguirre, J.; Wan, J.; et al. Low Protein Intake Is Associated with a Major Reduction in IGF-1, Cancer, and Overall Mortality in the 65 and Younger but Not Older Population. Cell Metab. 2014, 19, 407–417. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, S.; Lagisz, M.; Hector, K.L.; Spencer, H.G. Comparative and meta-analytic insights into life extension via dietary restriction. Aging Cell 2012, 11, 401–409. [Google Scholar] [CrossRef]
- Chen, Z.; Glisic, M.; Song, M.; Aliahmad, H.A.; Zhang, X.; Moumdjian, A.C.; Gonzalez-Jaramillo, V.; Van Der Schaft, N.; Bramer, W.M.; Ikram, M.A.; et al. Dietary protein intake and all-cause and cause-specific mortality: Results from the Rotterdam Study and a meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2020, 35, 411–429. [Google Scholar] [CrossRef] [Green Version]
- Gorissen, S.H.M.; Crombag, J.J.R.; Senden, J.M.G.; Waterval, W.A.H.; Bierau, J.; Verdijk, L.B.; Van Loon, L.J.C. Protein content and amino acid composition of commercially available plant-based protein isolates. Amino Acids 2018, 50, 1685–1695. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Joung, H. A traditional Korean dietary pattern and metabolic syndrome abnormalities. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 456–462. [Google Scholar] [CrossRef]
- Park, K.-B.; Park, H.A.; Kang, J.-H.; Kim, K.; Cho, Y.G.; Jang, J. Animal and Plant Protein Intake and Body Mass Index and Waist Circumference in a Korean Elderly Population. Nutrients 2018, 10, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All-Cause Mortality | |||
|---|---|---|---|
| Variables | Event (n = 2110) | Non-Event (n = 40,082) | p-Value |
| Age | 70.2 ± 11.1 | 48.7 ± 15.9 | <0.0001 |
| Sex | <0.0001 | ||
| Female | 936 (44.4) | 24,309 (60.7) | |
| Male | 1174 (55.6) | 15,773 (39.3) | |
| BMI, kg/m2 | 23.0 ± 3.4 | 23.7 ± 3.4 | <0.0001 |
| Smokers | <0.0001 | ||
| No | 871 (45.6) | 25,271 (65.0) | |
| Yes | 1041 (54.4) | 13,585 (35.0) | |
| Alcohol drinkers | <0.0001 | ||
| No | 1212 (73.5) | 19,691 (54.2) | |
| Yes | 436 (26.5) | 16,643 (45.8) | |
| Exercise | 0.0566 | ||
| No | 1326 (62.8) | 24,356 (60.8) | |
| Yes | 784 (37.2) | 15,726 (39.2) | |
| SBP, mmHg | 129.2 ± 19.4 | 118.1 ± 17.2 | <0.0001 |
| DBP, mmHg | 74.7 ± 11.5 | 75.6 ± 10.5 | 0.0006 |
| Pulse rate | 66.7 ± 20.2 | 58.4 ± 13.2 | <0.0001 |
| Fasting Glucose, mg/dL | 107.4 ± 35.4 | 97.8 ± 22.0 | <0.0001 |
| Total cholesterol, mg/dL | 187.0 ± 39.3 | 189.0 ± 35.7 | 0.0363 |
| Triglycerides, mg/dL | 140.1 ± 109.8 | 131.6 ± 104.4 | 0.0016 |
| HDL-cholesterol, mg/dL | 46.2 ± 12.3 | 49.9 ± 11.8 | <0.0001 |
| Total Energy intake | 1630.8 ± 675.1 | 1951.2 ± 813.8 | <0.0001 |
| Carbohydrate (%) | 73.0 ± 12.6 | 66.5 ± 13.3 | <0.0001 |
| Fat (%) | 11.8 ± 7.4 | 17.2 ± 8.7 | <0.0001 |
| Protein (%) | 12.7 ± 3.9 | 14.0 ± 4.0 | <0.0001 |
| Variables | Warranty Period (1%) | n | Person-Time (Years) | Events, n (%) | Incidence Per 1000 Person-Years (95% CI) |
|---|---|---|---|---|---|
| Carbohydrate (%) | |||||
| <40% | 3.422 | 1765 | 12,113.74 | 50(2.8) | 4.128(2.986–5.269) |
| 40–50% | 3.499 | 3169 | 21,895.57 | 77(2.4) | 3.517(2.733–4.301) |
| 50–60% | 3.504 | 6630 | 46,056.25 | 169(2.6) | 3.669(3.117–4.222) |
| 60–70% | 3.170 | 11,416 | 82,012.67 | 360(3.2) | 4.390(3.937–4.842) |
| ≤70% | 1.918 | 19,212 | 141,478.84 | 1454(7.6) | 10.277(9.752–10.803) |
| Fat (%) | |||||
| <10% | 1.584 | 9871 | 71,833.02 | 1029(10.4) | 14.325(13.456–15.194) |
| 10–20% | 2.748 | 18,424 | 134,497.21 | 815(4.4) | 6.060(5.645–6.474) |
| 20–30% | 4.255 | 10,433 | 73,652.93 | 213(2.0) | 2.892(2.504–3.280) |
| 30–40% | 6.167 | 2865 | 19,461.84 | 38(1.3) | 1.953(1.332–2.573) |
| ≤40% | 2.666 | 599 | 4112.05 | 15(2.5) | 3.648(1.805–5.490) |
| Protein (%) | |||||
| <10% | 1.586 | 5584 | 38,546.72 | 531(9.5) | 13.775(12.612–14.939) |
| 10–20% | 2.674 | 33,674 | 243,031.97 | 1470(4.4) | 6.049(5.740–6.357) |
| 20–30% | 2.836 | 2760 | 20,725.99 | 103(3.7) | 4.970(4.012–5.927) |
| ≤30% | 1.923 | 174 | 1252.38 | 6(3.5) | 4.791(0.967–8.615) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-J.; Lee, H.S.; Park, J.-Y.; Lee, J.-W. Associating Intake Proportion of Carbohydrate, Fat, and Protein with All-Cause Mortality in Korean Adults. Nutrients 2020, 12, 3208. https://doi.org/10.3390/nu12103208
Kwon Y-J, Lee HS, Park J-Y, Lee J-W. Associating Intake Proportion of Carbohydrate, Fat, and Protein with All-Cause Mortality in Korean Adults. Nutrients. 2020; 12(10):3208. https://doi.org/10.3390/nu12103208
Chicago/Turabian StyleKwon, Yu-Jin, Hye Sun Lee, Ju-Young Park, and Ji-Won Lee. 2020. "Associating Intake Proportion of Carbohydrate, Fat, and Protein with All-Cause Mortality in Korean Adults" Nutrients 12, no. 10: 3208. https://doi.org/10.3390/nu12103208
APA StyleKwon, Y.-J., Lee, H. S., Park, J.-Y., & Lee, J.-W. (2020). Associating Intake Proportion of Carbohydrate, Fat, and Protein with All-Cause Mortality in Korean Adults. Nutrients, 12(10), 3208. https://doi.org/10.3390/nu12103208