1. Introduction
Due to climatic factors and a traditionally nomadic lifestyle, Mongolia contains a smaller fraction of arable land devoted to permanent crops than any other country (0.003%) [
1], and the national food supply is marked by a pattern of extremes. Normalized against the total per capita supply of caloric energy in each country, data from the Food and Agriculture Organization of the United Nations (FAO) from the most recent year available indicate that the daily per capita food supply of Mongolia ranked 9th and 12th out of 175 countries in terms of whole milk and meat supplied, respectively, and ranked in the bottom 10% of countries in the supply of fruit, fish and seafood, pulses, and oil crops [
2]. Particularly in rural areas, food consumption remains highly seasonal, especially with respect to dairy products and meat which are mostly consumed in summer and winter, respectively [
3].
Extremes in Mongolia’s national food supply are plausibly related to the national burden of disease, particularly chronic disease. Recent analysis of the Global Dietary Database shows that Mongolia scored lower than any other country in both 1990 and 2017 in the Alternative Healthy Eating Index [
4]. Using FAO food balance data to estimate food consumption in Mongolia [
5], the Global Burden of Disease study found that out of 195 countries and territories in 2017, Mongolia ranked 1st globally in the fraction of cardiovascular (CVD) mortality attributable to dietary imbalances in both men (62.8%) and women (60.5%) and 12th in the rate of age-standardized all-cause mortality attributable to diet (309 deaths per 100,000) [
6]. Mongolia also ranked 22nd and 12th in rates of all-cause and CVD mortality attributable to metabolic risk factors. While childhood stunting and vitamin A deficiency have decreased over the past two decades, this period has also seen a sharp rise in the prevalence of adolescent and adult overweight and type 2 diabetes [
7,
8]. Currently, almost one third of pregnant women are anemic, less than two thirds of infants are reportedly exclusively breastfed up to six months of age, and vitamin D deficiency is endemic [
7,
9].
Despite these concerning statistics, national assessments of dietary intakes of individuals are lacking for the Mongolian population. From 1999–2009, dietary assessments of individuals and analytic epidemiologic research on Mongolian and Inner Mongolian diets were pioneered by Mongolian and Japanese scientists [
10,
11,
12,
13,
14,
15], but methods used in these studies were not applied on a nationwide scale. Current nationally-representative food or nutrient consumption data at the individual level are not available. Without such data, it is impossible to precisely quantify the extent of dietary imbalances throughout the population, and difficult to design evidence-based and targeted strategies to address such imbalances.
The objective of this study was to provide a multifaceted nutritional analysis of the modern Mongolian diet, using paired summer and winter weighed diet records collected from urban and rural Mongolian men and women living in 8 regions of the country. As part of a prior analysis based on these diet records [
16], we reported the extent of population dietary inadequacy of 10 micronutrients; the present analysis extends this investigation to 21 nutrients, includes analysis of daily intake of food groups and their contributions to nutrient intakes, and includes exploratory analysis of population diet patterns. To support interpretation of the dietary data, we also assessed anthropometry and selected micronutrient biomarkers.
3. Results
Based on a possible maximum of 6 diet records (3 per season), 2 serum samples (1 per season), and 1 height and weight measurement collected from each participant, participants (167 men and 167 women) completed 1838 of 1986 (92.5%) diet records (mean number of records per person: 5.50), provided 610 of 658 (92.7%) serum samples (mean number of samples per person: 1.83), and 315 of 334 (94.3%) height and weight measurements (
Table S2). Mean age of participants was 39.2 years (
Table S3). Additional population characteristics have been reported previously [
9]. There were no significant differences in age, sex, urbanicity, province, or season between participants who provided a serum sample in both summer and winter and 3.9% who provided only one sample.
Urban men and women consumed more fruits and non-tuberous vegetables than their rural counterparts in both seasons, with urban women consuming markedly more fruit than any other population subgroup (62 and 69 g/day in summer and winter, respectively) (
Table 1). However, consumption of fruits, non-tuberous vegetables, eggs, nuts and seeds, fish and poultry, and whole grains was generally low across population subgroups and seasons, and consumption of deep orange tubers was not observed. Total consumption of milk and dairy products ranged from 116 g/day among urban males in winter to 657 g/day among rural males in summer, with rural men and women consuming more than their urban counterparts in both seasons, and summer consumption exceeding that in winter among all subgroups. Consumption of reduced-fat milk or dairy products was not observed. Consumption of juice and sugar-sweetened beverages (SSBs) was highest in urban areas, particularly among urban males (178 and 138 g/day in summer and winter, respectively), while consumption of sweets was highest among urban females (28 and 34 g/day in summer and winter, respectively), and approximately double that of their rural counterparts. Consumption of meat was extremely high, particularly among men and in winter (with urban and rural men consuming 425 and 450 g/day in winter, respectively), as was that of refined grains (ranging from 322 g/day among rural females in summer and 533 g/day among rural males in winter). Age-trends in food consumption are presented in
Table S4.
Across subgroups and seasons, protein, carbohydrates, fat, and alcohol contributed an average of 21%, 40%, 38%, and 1% of caloric energy, respectively, and mean phytate intake did not exceed 500 mg (
Table 2). The prevalence of dietary protein, copper, phosphorous, zinc, riboflavin, niacin, and vitamin B12 inadequacy was very low, only exceeding 10% for riboflavin and niacin among urban females in winter. A moderate prevalence of iron inadequacy was observed among urban women (19 and 21% in summer and winter, respectively) and rural women (16 and 14%). Inadequacies of calcium, magnesium, thiamin, and vitamins A and B6 were common, and almost the entire study population was inadequate in folate and vitamins C, D, and E in both seasons. Median intakes of dietary fiber and potassium fell short of sex-specific adequate intake levels, and median intakes of manganese and pantothenic acid generally met or exceeded adequate levels (median intake (IQR) of fiber, potassium, manganese, and pantothenic acid averaged across the 8 subgroup-seasons: 9.3 (4.3), 2732 (1117), 3.176 (1.568), 6.354 (2.596), respectively). Urban-rural differences in nutrient inadequacy were most salient for calcium (more commonly inadequate in urban areas), vitamin A (more common in urban areas in summer, and rural areas in winter), and vitamin B6 (more common in rural areas in summer). The prevalence of intakes above the upper limit did not exceed 10% except for calcium among rural males in summer (12%) (
Table S5), due to their high summer intake of milk and dairy products (mean: 657 g/day) which contributed 62% of their total calcium intake in that season. Age-trends in nutrient intake and adequacy are presented in
Table S6.
Dishes contributing the majority of dietary energy in urban and rural areas included bread with or without toppings (contributing an average of 10% across urban and rural men and women in summer and winter, and 8% across rural subgroups), milk, dairy products, and airag (fermented mares’ milk) (10 and 18% in urban and rural subgroups respectively), biscuits, cookies, and doughnuts (12 and 18%), stir fries (21 and 15%), soups (14 and 13%), dumplings not included in soup (14 and 13%), and miscellaneous meat dishes (9 and 10%) (
Table 3). See
Table S7 for each dish’s contribution to other nutrients.
Of the study population, 61% of the men and 51% of the women were overweight, with 16% and 8%, respectively, being obese; 3% were underweight (
Table 4). Mean BMI was significantly higher among men than women in both urban areas (men: 26.9 kg/m
2, women: 25.5) and rural areas (men: 26.0, women: 24.6), and did not differ across urban and rural areas within sex. In adjusted analyses, urban residence was independently associated with higher BMI (adjusted mean: 26.4 vs. 24.9 in urban and rural areas, respectively) (
Table 5). Biochemical iron deficiency, iron overload, and vitamin A deficiency were observed only in
n = 12, 4, and 2 samples, respectively, and elevated CRP and AGP concentrations were observed in 11 and 7% of samples, respectively (
Table 4). Urban residence was independently associated with higher serum RBP and lower AGP concentrations (
Table 5).
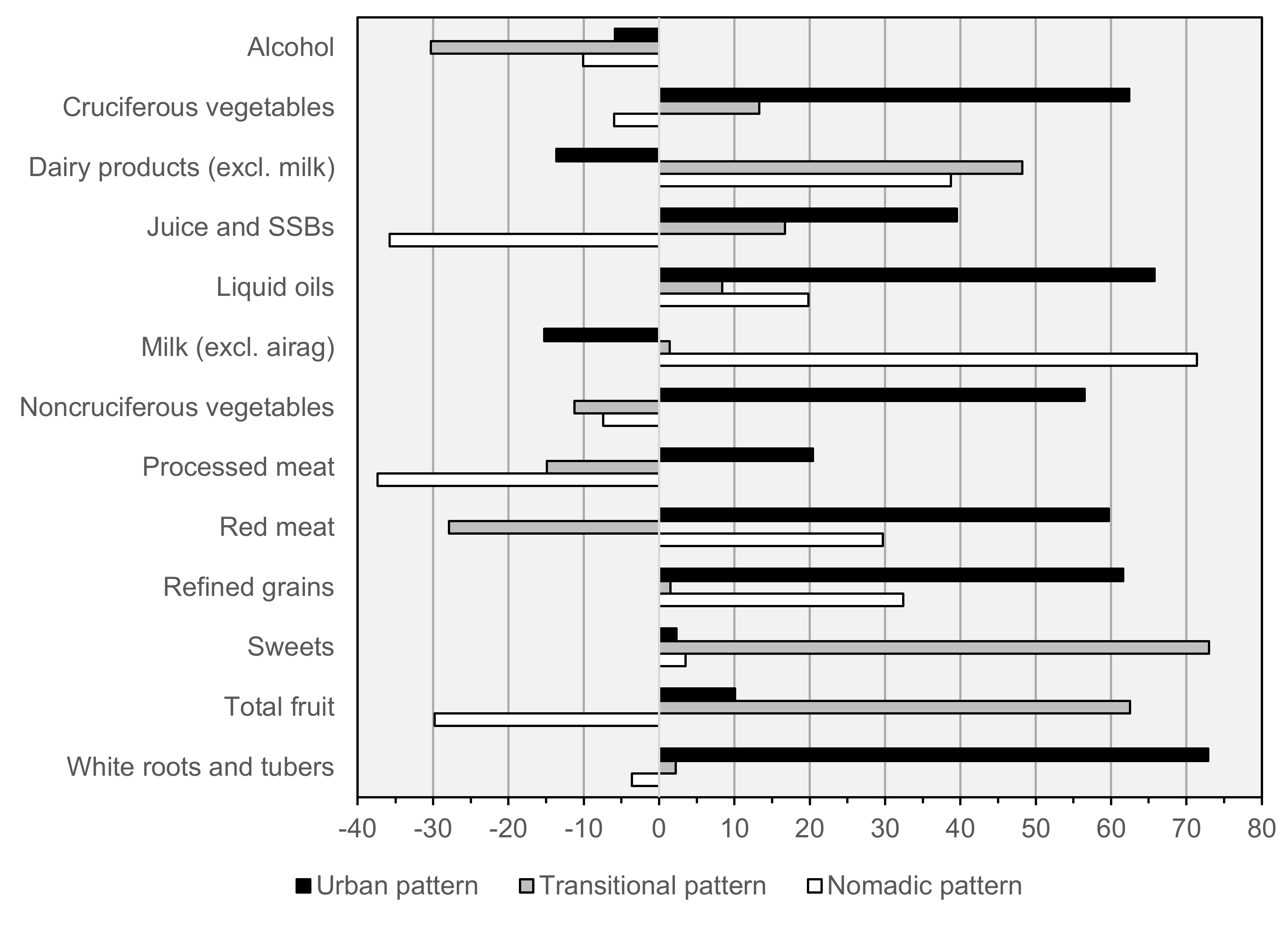
Factor loadings, and the mean observed intake of each factor component across quintiles of factor scores in both seasons combined are presented in
Table 6 and
Figure 2. Three patterns were retained: an “Urban” pattern (attributing 21% of variance in intake of factor components) marked by high consumption of vegetables, juice and sugar-sweetened beverages, liquid oils, red meat, refined grains, and white roots and tubers; a “Transitional” pattern (11% of variance) marked by high consumption of dairy products, sweets, and fruit, and low alcohol and red meat; and a “Nomadic” pattern (10% of variance) marked by high consumption of dairy products, milk, red meat, and refined grains, and low juice and SSBs, processed meat, and fruit. In adjusted analyses, adherence to the Urban pattern was significantly higher among urban and Ulaanbaatar residents; the Transitional pattern was most associated with female sex, and the Nomadic pattern with rural residence (
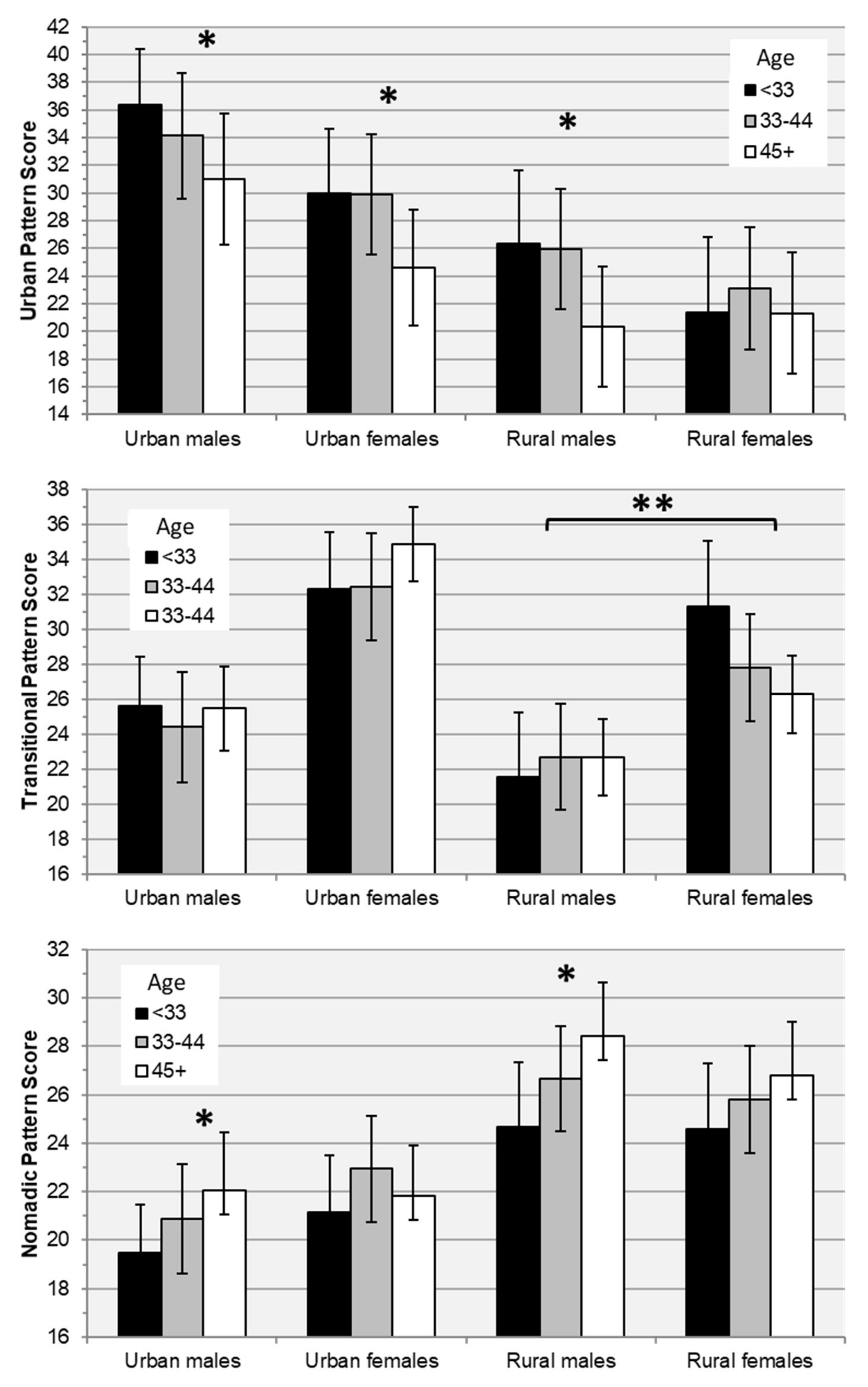
Table 7). Urban pattern scores were independently associated with younger age in all subgroups except rural females, the Transitional pattern was not associated with age in any subgroup, and Nomadic pattern scores increased with age among urban and rural males (
Table 8,
Figure 3). Adjusting for total energy intake and other covariates, increased adherence to the Urban pattern was significantly associated with increased intakes of protein, fiber, iron, and zinc, and decreased calcium intake; the Transitional pattern with increased protein intake; and both the Transitional and Nomadic patterns with increased intakes of iron and zinc, and decreased fiber intake (
Table 9).
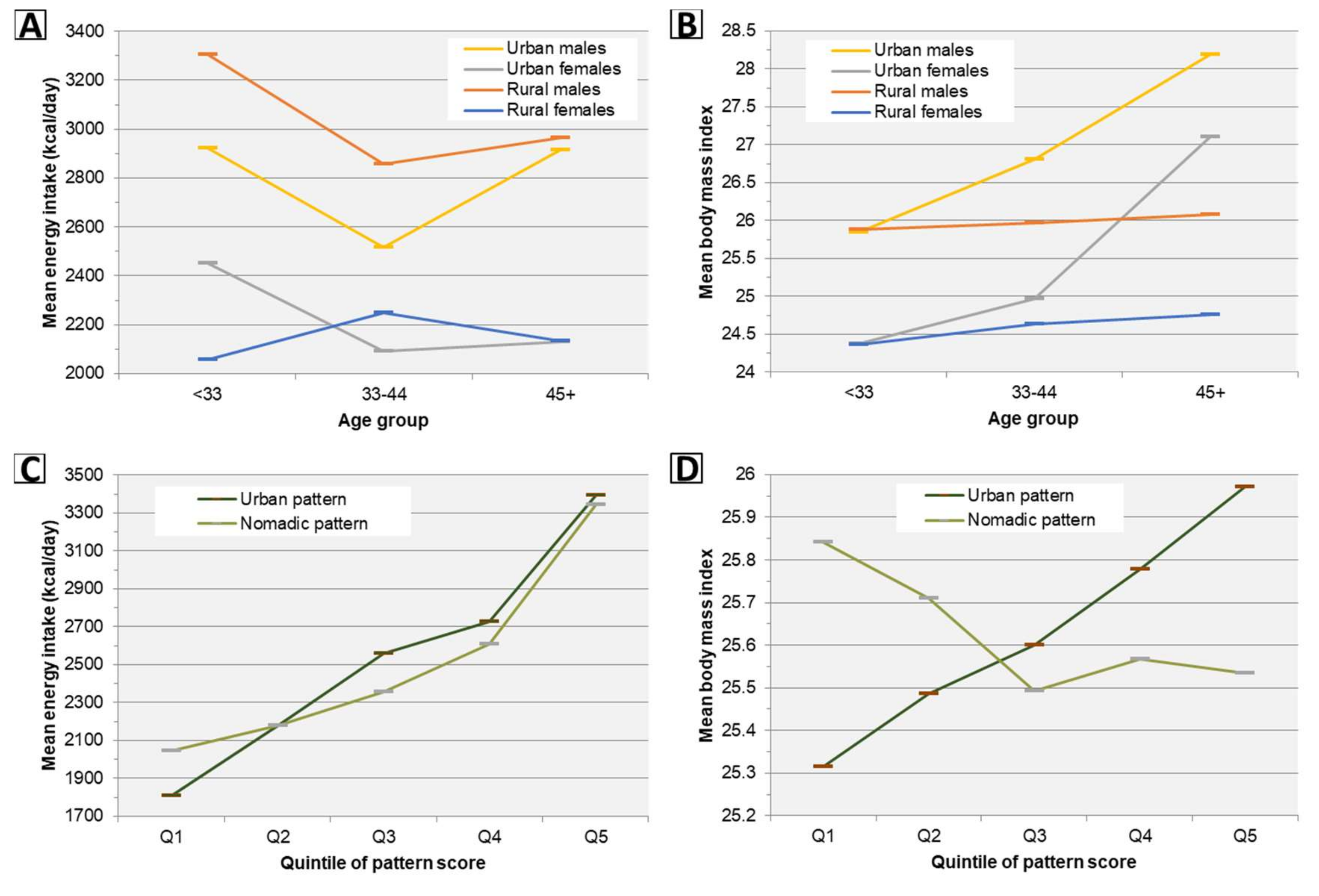
Trends in estimated marginal means of energy intake and body mass index by age and pattern scores across subgroups are presented graphically in
Figure 4. Despite no significant differences in linear trend of adjusted energy intake with age between any population subgroups, a significant upward trend in BMI with age was observed among both men and women in urban areas but not rural areas (
Figure 4,
Table 5). Increased adherence to all pattern scores was independently associated with increased energy intake, however only the Urban pattern was also (positively) associated with increased BMI (
Figure 4,
Table 9).
4. Discussion
The present study found a high prevalence of key dietary nutrient inadequacies in a nationwide sample of Mongolian adults in summer and winter. Prior analysis of data collected from the present study population, and the Fifth National Nutrition Survey (FNNS), indicate an extremely high prevalence of biochemical vitamin D deficiency throughout the Mongolian population, especially in winter [
7,
9]. The present study also found a high prevalence of dietary vitamin A inadequacy, and among women, a moderate prevalence of iron inadequacy. By contrast, we found little evidence of biochemical iron and vitamin A deficiency; in the FNNS, these deficiencies were also rare, while iron deficiency was moderately prevalent among pregnant women [
7]. Retinol binding protein, while useful for assessing clinical vitamin A deficiency, is subject to homeostatic regulation that renders it a less sensitive measure of subclinical deficiency (which may be widespread in Mongolia, given the high prevalence of dietary vitamin A inadequacy observed in the present study). There is also evidence that biochemical deficiencies disproportionately affect young children and pregnant women in Mongolia [
7,
28,
34].
Other nutrients of concern identified in our study included fiber, calcium, magnesium, thiamin, folate, and vitamins B6, C, D, and E, while inadequacies of protein, zinc, riboflavin, niacin, and vitamin B12 were uncommon. With the exception of calcium, these findings can generally be attributed to the population’s low consumption of nutrient-dense vegetal foods (including fruits, non-tuberous vegetables, and whole grains) and high consumption of animal-source foods. Low calcium intake was more common in urban areas and in winter given lower urban and winter consumption of milk and dairy products. Inadequate intake of calcium, vitamin D, and magnesium may jointly contribute to the relatively high prevalence of osteoporosis in Mongolian adults [
35], and low intake of fiber has been linked to higher risk of heart disease, type 2 diabetes, and metabolic syndrome in large prospective cohort studies [
36,
37,
38]. Implications of observed deficits of folate and other nutrients are discussed in previous studies by our group [
16], in which we have also suggested evidence-based interventions to reduce the prevalence of micronutrient deficiency in the Mongolian population, including industrial food fortification and micronutrient supplementation [
9,
16,
39]. As micronutrients work together to allow healthy body functioning and prevent disease, addressing multiple inadequacies (particularly through large-scale diet modification in the long term) may reap multiplicative benefits, and ensuring adequate micronutrient intake should remain integral to Mongolia’s national health policy.
It is notable that fat contributed an average of 38% of caloric energy in this survey. Although we lacked data on the breakdown of fatty acid intake, as the majority of fat consumed originated from meat and dairy products, it can be assumed that saturated fat contributed a majority of fat consumed; this is supported by results from the Global Dietary Database [
40]. Omega-3 fatty acid intake was also likely very low in the study population, given minimal observed intake of fish, nuts, and seeds, and the relatively low alpha-linolenic content of the dominant liquid oil consumed (sunflower seed oil) [
41]. Low intake of unsaturated fats has been associated with a more deleterious cholesterol profile, insulin resistance, and higher blood pressure [
42,
43,
44,
45]; this, and a combination with a constellation of other dietary risks for chronic disease observed in our study (including high intake of refined grains, red meat, and high intake of sugary drinks in urban areas) are likely important contributors to the increasing burden of cardiovascular disease and type 2 diabetes in Mongolia [
6,
7,
8].
In the present study, three dietary patterns explained 41% variation in consumption of major food groups, and while all were associated with increased energy intake, only the “Urban” pattern was independently associated with increased body mass index. In a prior study, Dugee and colleagues derived three exploratory diet patterns using semiquantitative food frequency questionnaire data collected from 420 healthy men and women aged >25 years from urban and rural areas of Ulaanbaatar and Khuvsgul in August 2005 [
46], providing an interesting comparison with Mongolian adults in the present study in 2012–2016. Between 2005 and 2012–2016, pattern factor loadings and the variation in food intake explained by each were closely comparable, except that the 2012–2016 “Transitional” pattern contains high factor loadings for both sweets and SSBs not present in the comparable 2005 “Healthy” pattern. Likely in part due to this difference, only the 2005 “Healthy” pattern, and not its 2012–2016 “Transitional” counterpart, was associated with reduced odds of obesity in energy-adjusted analysis. Both the 2005 study’s “Transitional” pattern and its 2012–2016 “Urban” counterpart were associated with obesity in both unadjusted and energy-adjusted analyses, while the 2005 “Traditional” pattern and its 2012–2016 “Nomadic” counterpart were not, suggesting that diets in urban Mongolia have remained consistently obesogenic, while that of rural areas are not. Furthermore, our finding that adherence to the 2012–2016 “Urban” and “Nomadic” patterns decreases and increases with age, respectively, in both urban and rural areas suggests the possibility that the nation will continue to converge toward an increasingly obesogenic diet in the future.
A key finding of this study was an upward trend in BMI by age among urban Mongolian adults, but not rural ones, despite similar age trends in energy intake. One probable reason for this difference is an intensely physically-active lifestyle that many nomadic Mongolians continue to engage in even into older age, while lifestyles in urban areas have become increasingly sedentary [
8]. Another likely reason is higher adherence in urban areas to the Urban diet pattern, which was positively associated with BMI after adjustment for age and energy intake. It is known that increased consumption of specific foods typically associated with industrial or western diet patterns globally (such as refined grain products and sugar-sweetened beverages, factor loadings of which were highest for the Urban pattern) are linked to long-term weight gain independent of increases in energy intake [
47].
Comparable to results of the FNNS, the present study observed a low prevalence of underweight and a high prevalence of overweight and obesity among urban and rural men and non-pregnant women [
7]. Nationally, from 2005 to 2013 alone, the prevalence of child stunting decreased from 27.5 to 10.8% [
1], while that of overweight increased more than all but three countries globally [
48]. In addition, analysis of Multiple Indicator Cluster Survey (MICS) data from 2005, 2009, and 2013 has shown consistent increases in population mean body mass index, waist circumference, percent body fat, blood pressure, and cholesterol in the adult population [
8], with 61.9% and 27.5% of Mongolian adults having elevated levels of serum cholesterol and blood pressure, respectively, or on blood pressure medication. Concurrent to trends in metabolic risks, 2005 to 2013 saw a 11.4% increase in per capita caloric energy in the Mongolian Food Supply (the 15th largest increase among 175 countries during that period) and an increase in the prevalence of low physical activity (<600 MET-minutes/week) from 7.4 to 22.3% [
2,
8], trends that are in turn plausibly related to tremendous economic and demographic changes that have swept Mongolia as a result of the country’s recent mining boom. Since the year 2000, the fraction of Mongolians living in urban areas increased from 57.1 to 68.4%, national gross domestic production by a factor of 11.4, and total imports value by a factor of 9.6 [
1]. While rapid economic growth and foreign investment, globalization of the food market, and shifts from a traditionally nomadic lifestyle to one of urban sedentism are implicated in Mongolia’s waning burden of severe undernutrition, these trends have also contributed toward the proliferation of noncommunicable diseases and have done so since the country’s tumultuous adoption of free-market reforms after 1990 [
49].
Nonetheless, there is some evidence that the overall nutritional quality of the Mongolian food supply has improved from 1990 to 2010 in terms of both increased per capita supply of healthy foods and nutrients, and decreased supply of unhealthy ones (more so than any other country) [
50]. Shifts in specific dietary components during this period may have also predisposed Mongolians to weight loss and other positive metabolic changes independent of changes in caloric intake [
47]; these include a 69.4 to 52.6 g/day decrease in intake of sugar-sweetened beverages and a 12.9 to 25.9 g/day increase in whole grains [
40]. Despite these improvements, the annual reduction in age-standardized cardiovascular, type 2 diabetes, and cancer mortality attributable to dietary imbalances from 1990 to 2010 has been minimal (−0.5%, which is close to the median change observed in countries globally), while the magnitude of reductions in under-5 DALYs attributable to wasting (−8.9%), stunting (−10.6%), protein-energy malnutrition (−11.6%), and deficiencies of iron (−7.8%), zinc (−11.0%), and other nutrients (−11.5%) during this period has each been within the top 15% of countries [
6]. This is in part attributable to the fact that national indicators of undernutrition respond relatively sensitively to increased food and nutrient availability, while NCDs do not on account of their longer longer latency periods. It can therefore be expected that ongoing improvements in the Mongolian food supply will have a more positive impact on NCD risk in the future, and this is borne out by current models that project a substantially increased annual reduction (−2.1%) in age-standardized diet-related mortality from 2020 to 2040 [
6].
To our knowledge, this has been the most detailed and expansive study of the diet of Mongolian adults to date. An important strength of this study was the use of paired sampling in summer and winter, which ensured that seasonal differences were largely un-confounded by participant characteristics. One limitation of the study was the fact that data were collected in only two seasons, although this limitation was mitigated by sampling during the peaks of summer and winter (which represent seasonal extremes in the Mongolian food supply). A second limitation was the lack of data on physical activity, which likely plays a role in differences in clinical measurements observed between subgroups, particularly urban-rural differences. To reduce bias in associational analyses, we attempted to stratify by or control for factors that may in part reflect physical activity (such as urbanicity, energy intake, or BMI), however, residual confounding is possible. Third, due to resource limitations, each year of the study involved data collection from up to three provinces only, and in each province, collection was completed over the course of one year; it was therefore not possible to examine changes in diet or nutrition that may have occurred in diet and nutrition from 2011 to 2016 (which are possible, given rapid trends in urbanization and global market integration that have occurred in Mongolia in recent years) because such analyses would be intractably confounded by region. Fourth, despite the size and breadth of the study population (comprising 1838 person-days of summer and winter prospective dietary intake from urban and rural men and women in 8 national provinces), and the use of random sampling within each province, the study population is not intended to be nationally-representative and results should be interpreted in the context of the sampling frame. Readers of our earlier fortification modeling study [
16], which includes national estimates for the baseline prevalence of dietary inadequacy of ten nutrients using data from the same population as the present study, will note moderate quantitative differences between those and the present results for thiamin and vitamin A in some subgroups. These differences may be attributable to differing methodologies used in estimating intake distributions as well as our earlier use of survey weights. The latter were necessary given the objective of that study to estimate and evaluate operational parameters of a national fortification program; for the explicit purpose of describing population thiamin and vitamin A adequacy, we thus suggest treating the estimates of both studies as realistic bounds of the true values.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}