Food Involvement, Eating Restrictions and Dietary Patterns in Polish Adults: Expected Effects of Their Relationships (LifeStyle Study)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Ethical Approval
2.3. Eating Restrictions
2.4. Dietary Patterns
2.5. Food Involvement
2.6. Sociodemographic Variables
2.7. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Dietary Patterns
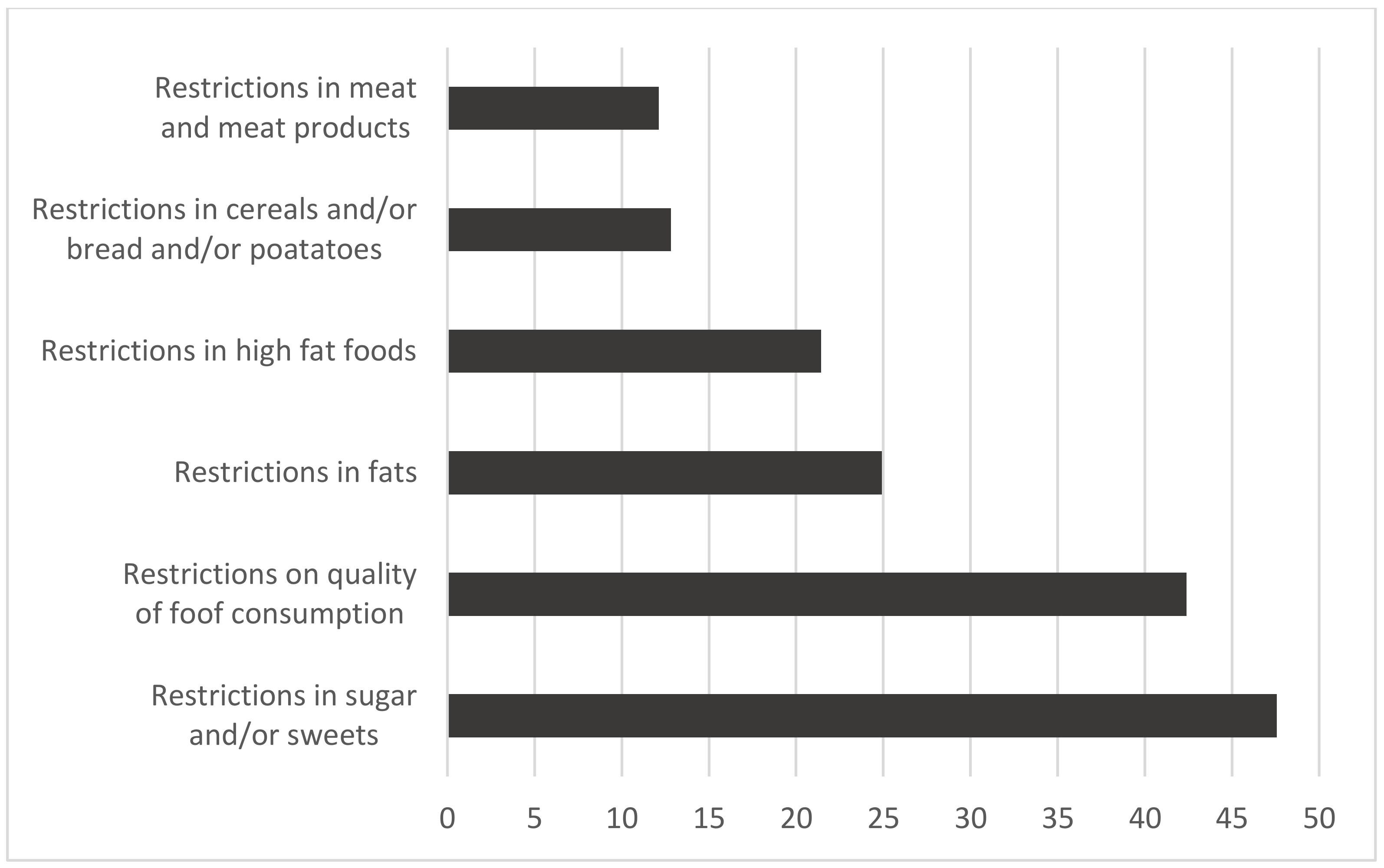
3.3. Eating Restrictions
3.4. Food Involvement
3.5. Associations between Eating Restrictions, Food Involvement, and Dietary Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mond, J.; Van den Berg, P.; Boutelle, K.; Hannan, P.; Neumark-Sztainer, D. Obesity, body dissatisfaction, and emotional well-being in early and late adolescence: Findings from the project EAT study. J. Adolesc. Heal. 2011, 48, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Fayet, F.; Petocz, P.; Samman, S. Prevalence and correlates of dieting in college women: A cross sectional study. Int. J. Womens Health 2012, 4, 405. [Google Scholar] [PubMed] [Green Version]
- Iorga, M.; Manole, I.; Pop, L.; Muraru, I.-D.; Petrariu, F.-D. Eating disorders in relationship with dietary habits among pharmacy students in Romania. Pharmacy 2018, 6, 97. [Google Scholar] [CrossRef] [Green Version]
- Kesse-Guyot, E.; Bertrais, S.; Peneau, S.; Estaquio, C.; Dauchet, L.; Vergnaud, A.C.; Czernichow, S.; Galan, P.; Hercberg, S.; Bellisle, F. Dietary patterns and their sociodemographic and behavioural correlates in French middle-aged adults from the SU. VI. MAX cohort. Eur. J. Clin. Nutr. 2009, 63, 521–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Togo, P.; Osler, M.; Sørensen, T.I.A.; Heitmann, B.L. Food intake patterns and body mass index in observational studies. Int. J. Obes. 2001, 25, 1741–1751. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Pareja, M.; Guallar-Castillón, P.; Mesas, A.E.; López-García, E.; Rodríguez-Artalejo, F. Obesity-related eating behaviors are associated with higher food energy density and higher consumption of sugary and alcoholic beverages: A cross-sectional study. PLoS One 2013, 8. [Google Scholar] [CrossRef] [Green Version]
- Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; WHO Technical Report Series 916; World Health Organization: Geneva, Switzerland, 2003; Volume 916.
- Messier, S.P.; Mihalko, S.L.; Legault, C.; Miller, G.D.; Nicklas, B.J.; DeVita, P.; Beavers, D.P.; Hunter, D.J.; Lyles, M.F.; Eckstein, F. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: The IDEA randomized clinical trial. Jama 2013, 310, 1263–1273. [Google Scholar] [CrossRef]
- Napoli, N.; Shah, K.; Waters, D.L.; Sinacore, D.R.; Qualls, C.; Villareal, D.T. Effect of weight loss, exercise, or both on cognition and quality of life in obese older adults. Am. J. Clin. Nutr. 2014, 100, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Bell, R.; Marshall, D.W. The construct of food involvement in behavioral research: Scale development and validation☆. Appetite 2003, 40, 235–244. [Google Scholar] [CrossRef]
- Oliveros, E.; Somers, V.K.; Sochor, O.; Goel, K.; Lopez-Jimenez, F. The concept of normal weight obesity. Prog. Cardiovasc. Dis. 2014, 56, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Pliner, P.; Hobden, K. Development of a scale to measure the trait of food neophobia in humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef]
- Marshall, D.; Bell, R. Relating the food involvement scale to demographic variables, food choice and other constructs. Food Qual. Prefer. 2004, 15, 871–879. [Google Scholar] [CrossRef]
- Jarman, M.; Lawrence, W.; Ntani, G.; Tinati, T.; Pease, A.; Black, C.; Baird, J.; Barker, M.; Group, S.I.H.S. Low levels of food involvement and negative affect reduce the quality of diet in women of lower educational attainment. J. Hum. Nutr. Diet. 2012, 25, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Sarmugam, R.; Worsley, A. Dietary behaviours, impulsivity and food involvement: Identification of three consumer segments. Nutrients 2015, 7, 8036–8057. [Google Scholar] [CrossRef]
- Olsen, S.O. Consumer involvement in seafood as family meals in Norway: An application of the expectancy-value approach. Appetite 2001, 36, 173–186. [Google Scholar] [CrossRef]
- Juhl, H.J.; Poulsen, C.S. Antecedents and effects of consumer involvement in fish as a product group. Appetite 2000, 34, 261–267. [Google Scholar] [CrossRef]
- Smith, A.D.A.C.; Emmett, P.M.; Newby, P.K.; Northstone, K. A comparison of dietary patterns derived by cluster and principal components analysis in a UK cohort of children. Eur. J. Clin. Nutr. 2011, 65, 1102. [Google Scholar] [CrossRef] [Green Version]
- Ruano, C.; Henriquez, P.; Martínez-González, M.Á.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Sanchez-Villegas, A. Empirically derived dietary patterns and health-related quality of life in the SUN project. PLoS One 2013, 8, e61490. [Google Scholar] [CrossRef] [Green Version]
- Thorpe, M.G.; Milte, C.M.; Crawford, D.; McNaughton, S.A. A comparison of the dietary patterns derived by principal component analysis and cluster analysis in older Australians. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 30. [Google Scholar] [CrossRef] [Green Version]
- Esmaillzadeh, A.; Entezari, M.; Paknahad, Z.; Safavi, M.; Jalali, M.; Ghiasvand, R.; Bahreini, N.; Nourian, M.; Azadbakht, L. Identification of diet-disease relations through dietary pattern approach: A review. J. Res. Med. Sci. 2008, 13, 337–348. [Google Scholar]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Galinski, G.; Lonnie, M.; Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Self-Reported Dietary Restrictions and Dietary Patterns in Polish Girls: A Short Research Report (GEBaHealth Study). Nutrients 2016, 8, 796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beliefs and Eating Habits Questionnaire. Behavioral Conditions of Nutrition Team, Committee of Human Nutrition Science; Polish Academy of Science: Warsaw, Poland, 2014; Available online: http://www.knozc.pan.pl/ (accessed on 20 September 2017).
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M.; Bronkowska, M.; Dlugosz, A.; Loboda, D.; Wyka, J. Reproducibility of a questionnaire for dietary habits, lifestyle and nutrition knowledge assessment (KomPAN) in Polish adolescents and adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A. Discovering Statistics using IBM SPSS Statistics: North American Edition; Sage: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Jezewska-Zychowicz, M.; Gębski, J.; Guzek, D.; Świątkowska, M.; Stangierska, D.; Plichta, M.; Wasilewska, M. The Associations between Dietary Patterns and Sedentary Behaviors in Polish Adults (LifeStyle Study). Nutrients 2018, 10, 1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gębski, J.; Jezewska-Zychowicz, M.; Guzek, D.; Świątkowska, M.; Stangierska, D.; Plichta, M. The Associations between Dietary Patterns and Short Sleep Duration in Polish Adults (LifeStyle Study). Int. J. Environ. Res. Public Health 2018, 15, 2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Redman, L.M.; Ravussin, E. Caloric restriction in humans: Impact on physiological, psychological, and behavioral outcomes. Antioxid. Redox Signal. 2011, 14, 275–287. [Google Scholar] [CrossRef] [Green Version]
- Nakai, Y.; Noma, S.; Nin, K.; Teramukai, S.; Wonderlich, S.A. Eating disorder behaviors and attitudes in Japanese adolescent girls and boys in high schools. Psychiatry Res. 2015, 230, 722–724. [Google Scholar] [CrossRef]
- Ritchie, L.D.; Spector, P.; Stevens, M.J.; Schmidt, M.M.; Schreiber, G.B.; Striegel-Moore, R.H.; Wang, M.-C.; Crawford, P.B. Dietary patterns in adolescence are related to adiposity in young adulthood in black and white females. J. Nutr. 2007, 137, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Lyly, M.; Soini, E.; Rauramo, U.; Lähteenmäki, L. Perceived role of fibre in a healthy diet among Finnish consumers. J. Hum. Nutr. Diet. 2004, 17, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Mialon, V.S.; Clark, M.R.; Leppard, P.I.; Cox, D.N. The effect of dietary fibre information on consumer responses to breads and “English” muffins: A cross-cultural study. Food Qual. Prefer. 2002, 13, 1–12. [Google Scholar] [CrossRef]
- Lee, Y.; Joo, N. The awareness level and needs for education on reducing sugar consumption among mothers with preschool children. Nutr. Res. Pract. 2016, 10, 229–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayser, M.; Nitzko, S.; Spiller, A. Analysis of differences in meat consumption patterns. Int. Food Agribus. Manag. Rev. 2013, 16, 43–56. [Google Scholar]
- Adams, J.F.; Engstrom, A. Dietary intake of whole grain vs. recommendations. Cereal Foods World 2000, 45, 75–78. [Google Scholar]
- Wadolowska, L.; Kowalkowska, J.; Lonnie, M.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Associations between physical activity patterns and dietary patterns in a representative sample of Polish girls aged 13-21 years: A cross-sectional study (GEBaHealth Project). BMC Public Health 2016, 16, 1–14. [Google Scholar] [CrossRef] [Green Version]
- French, S.A.; Harnack, L.; Jeffery, R.W. Fast food restaurant use among women in the Pound of Prevention study: Dietary, behavioral and demographic correlates. Int. J. Obes. 2000, 24, 1353–1359. [Google Scholar] [CrossRef] [Green Version]
- Burton, P.; Smit, H.J.; Lightowler, H.J. The influence of restrained and external eating patterns on overeating. Appetite 2007, 49, 191–197. [Google Scholar] [CrossRef]
- Ernst, B.; Wilms, B.; Thurnheer, M.; Schultes, B. Eating behaviour in treatment-seeking obese subjects–Influence of sex and BMI classes. Appetite 2015, 95, 96–100. [Google Scholar] [CrossRef]
- Hebden, L.; O’Leary, F.; Rangan, A.; Singgih Lie, E.; Hirani, V.; Allman-Farinelli, M. Fruit consumption and adiposity status in adults: A systematic review of current evidence. Crit. Rev. Food Sci. Nutr. 2017, 57, 2526–2540. [Google Scholar] [CrossRef]
- Barker, M.; Lawrence, W.; Woadden, J.; Crozier, S.R.; Skinner, T.C. Women of lower educational attainment have lower food involvement and eat less fruit and vegetables. Appetite 2008, 50, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Candel, M.J.J.M. Consumers’ convenience orientation towards meal preparation: Conceptualization and measurement. Appetite 2001, 36, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Brutus, S.; Aguinis, H.; Wassmer, U. Self-reported limitations and future directions in scholarly reports: Analysis and recommendations. J. Manage. 2013, 39, 48–75. [Google Scholar] [CrossRef] [Green Version]
- Burton, M.; Reid, M.; Worsley, A.; Mavondo, F. Food skills confidence and household gatekeepers’ dietary practices. Appetite 2017, 108, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Begley, A.; Paynter, E.; Butcher, L.M.; Dhaliwal, S.S. Effectiveness of an Adult Food Literacy Program. Nutrients 2019, 11, 797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathi, N.; Riddell, L.; Worsley, A. Secondary school students’ views of food and nutrition education in Kolkata, India. Health Educ. 2017, 117, 310–322. [Google Scholar] [CrossRef]


{kind=link}
| Variables | N = 1007 | % | |
|---|---|---|---|
| Gender | Female | 529 | 52.5 |
| Male | 478 | 47.5 | |
| Age | 21–34 years | 370 | 36.7 |
| 35–44 years | 235 | 23.3 | |
| 45–54 years | 132 | 13.1 | |
| 55–65 years | 270 | 26.8 | |
| Residence | City | 539 | 53.5 |
| Town | 199 | 19.8 | |
| Country side | 269 | 26.7 | |
| Education | Secondary and lower than secondary | 403 | 40.1 |
| Higher | 604 | 59.9 | |
| Body mass index (BMI) category | Underweight (BMI ≤ 18.5 kg/m2) | 35 | 3.5 |
| Normal weight (18.5 kg/m2 < BMI ≤ 25 kg/m2) | 484 | 48.1 | |
| Overweight (25 kg/m2 < BMI ≤ 30 kg/m2) | 360 | 35.7 | |
| Obesity (BMI > 30 kg/m2) | 128 | 12.7 |
| Variables | Factor 1 Fast Foods and Sweets | Factor 2 Meat and Meat Products | Factor 3 Fruit and Vegetable | Factor 4 Whole Meal Food | Factor 5 Fruit and Vegetable Juices |
|---|---|---|---|---|---|
| Crisps and other salty snacks | 0.824 | . | . | . | . |
| Meals or snacks such as burgers, pizza, chicken, fries | 0.756 | . | . | . | . |
| Sweets and cakes | 0.702 | . | . | . | . |
| Fizzy drinks | 0.633 | . | . | . | . |
| Red meat (pork, beef, venison) | . | 0.783 | . | . | . |
| White meat (poultry, turkey) | . | 0.748 | . | . | . |
| Cured meats and sausages | . | 0.696 | . | . | . |
| Fried foods | . | 0.551 | . | . | . |
| Fruits | . | . | 0.825 | . | . |
| Vegetables | . | . | 0.764 | . | . |
| Cheeses (including melted cheese, blue cheese) | . | . | . | . | . |
| Whole meal pasta, groats | . | . | . | 0.839 | . |
| Whole meal bread | . | . | . | 0.763 | . |
| Fermented milk drinks | . | . | . | . | . |
| Vegetable juice | . | . | . | . | 0.830 |
| Fruit juice | . | . | . | . | 0.799 |
| Variance Explained (%) | 24.9 | 16.0 | 9.5 | 7.4 | 6.4 |
| Total Variance Explained (%) | 64.2 | ||||
| Kaiser’s Measure of Sampling Adequacy: | 0.781 | ||||
| Food Involvement Scale (FIS) | Mean | SD | Median |
|---|---|---|---|
| I think a lot about food each day. | 3.01 | 1.02 | 3 |
| Cooking or barbequing is a lot of fun. | 3.55 | 1.01 | 4 |
| Talking about what I ate or am going to eat is something I like to do. | 3.27 | 1.03 | 3 |
| Compared with other daily decisions, my food choices are very important. | 2.67 | 1.04 | 3 |
| When I travel, one of the things I anticipate most is eating the food there. | 3.45 | 0.99 | 4 |
| I do most or all of the clean up after eating. | 3.66 | 0.93 | 4 |
| I enjoy cooking for others and myself. | 3.53 | 1.07 | 4 |
| When I eat out, I think or talk a lot about how the food tastes. | 3.27 | 0.98 | 3 |
| I do like to mix or chop food. | 3.28 | 1.07 | 3 |
| I do most or all of my own food shopping. | 3.44 | 1.16 | 4 |
| I wash dishes or clean the table. | 3.39 | 1.15 | 4 |
| I care whether or not the table is nicely set. | 7.74 | 0.90 | 4 |
| Variable | Fast Foods and Sweets | Meat and Meat Products | Fruit and Vegetables | Whole Meal Food | Fruit and Vegetables Juices | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T3 | pa | T1 | T3 | p | T1 | T3 | p | T1 | T3 | p | T1 | T3 | p | |
| Restriction on quantity of food consumption (ref.: without restrictions): | |||||||||||||||
| OR crude (95%CI) | 1 | 0.41 (0.30; 0.56) | **** | 1 | 0.94 (0.68; 1.30) | ns | 1 | 2.30 (1.66; 3.19) | **** | 1 | 1.76 (1.27; 2.45) | *** | 1 | 0.61 (0.44; 0.85) | ** |
| Restrictions in consumption of sugar and/or sweets (ref.: without restrictions): | |||||||||||||||
| OR (95%CI) | 1 | 0.35 (0.25; 0.48) | **** | 1 | 0.64 (0.49; 0.88) | *** | 1 | 1.89 (1.36; 2.61) | **** | 1 | 3.14 (2.25; 4.39) | **** | 1 | 0.88 (0.63; 1.22) | ns |
| Restrictions in consumption of fats (ref.: without restrictions): | |||||||||||||||
| OR (95%CI) | 1 | 0.42 (0.29; 0.61) | **** | 1 | 0.68 (0.47; 0.98) | * | 1 | 1.93 (1.34; 2.77) | *** | 1 | 2.05 (1.40; 2.99) | *** | 1 | 0.89 (0.61; 1.28) | ns |
| Restrictions in consumption of high-fat foods (ref.: without restrictions): | |||||||||||||||
| OR (95%CI) | 1 | 0.23 (0.15; 0.36) | **** | 1 | 0.58 (0.39; 0.88) | *** | 1 | 1.90 (1.29; 2.80) | *** | 1 | 1.78 (1.20; 2.65) | ** | 1 | 1.13 (0.77; 1.67) | ns |
| Restrictions in consumption of cereals and/or bread and/or potatoes (ref.: without restrictions): | |||||||||||||||
| OR (95%CI) | 1 | 0.47 (0.30; 0.74) | **** | 1 | 1.16 (0.74; 1.83) | ns | 1 | 0.80 (0.51; 1.27) | ns | 1 | 1.91 (1.20; 3.04) | ** | 1 | 0.91 (0.57; 1.43) | ns |
| Restrictions in consumption of meat (ref.: without restrictions): | |||||||||||||||
| OR (95%CI) | 1 | 0.71 (0.44; 1.14) | ns | 1 | 0.29 (0.17; 0.48) | **** | 1 | 1.32 (0.81; 2.15) | ns | 1 | 3.13 (1.83; 5.35) | **** | 1 | 1.54 (0.94; 2.52) | ns |
| Food involvement (ref. higher than 40 points) | |||||||||||||||
| OR (95%CI) | 1 | 1.30 (0.94; 1.79) | ns | 1 | 1.80 (1.30; 2.49) | *** | 1 | 1.85 (1.34; 2.57) | *** | 1 | 3.46 (2.48; 4.82) | **** | 1 | 2.00 (1.44; 2.77) | **** |
| Eating Restrictions: | Food Involvement | ||
|---|---|---|---|
| FIS ≤ 40 Points | FIS > 40 Points | Pa | |
| Restriction on quantity of food consumption (ref.: without restrictions): | |||
| OR crude (95%CI) | 1 | 1.06 (0.86; 1.42) | ns |
| Restrictions in consumption of sugar and/or sweets (ref.: without restrictions): | |||
| OR (95%CI) | 1 | 1.28 (0.96; 1.57) | ns |
| Restrictions in consumption of fats (ref.: without restrictions): | |||
| OR (95%CI) | 1 | 1.35 (1.01; 1.80) | * |
| Restrictions in consumption of high-fat foods (ref.: without restrictions): | |||
| OR (95%CI) | 1 | 1.64 (1.21; 2.23) | ** |
| Restrictions in consumption of cereals and/or bread and/or potatoes (ref.: without restrictions): | |||
| OR (95%CI) | 1 | 1.32 (0.91; 1.92) | ns |
| Restrictions in consumption of meat (ref.: without restrictions): | |||
| OR (95%CI) | 1 | 1.27 (0.87; 1.86) | ns |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jezewska-Zychowicz, M.; Gębski, J.; Kobylińska, M. Food Involvement, Eating Restrictions and Dietary Patterns in Polish Adults: Expected Effects of Their Relationships (LifeStyle Study). Nutrients 2020, 12, 1200. https://doi.org/10.3390/nu12041200
Jezewska-Zychowicz M, Gębski J, Kobylińska M. Food Involvement, Eating Restrictions and Dietary Patterns in Polish Adults: Expected Effects of Their Relationships (LifeStyle Study). Nutrients. 2020; 12(4):1200. https://doi.org/10.3390/nu12041200
Chicago/Turabian StyleJezewska-Zychowicz, Marzena, Jerzy Gębski, and Milena Kobylińska. 2020. "Food Involvement, Eating Restrictions and Dietary Patterns in Polish Adults: Expected Effects of Their Relationships (LifeStyle Study)" Nutrients 12, no. 4: 1200. https://doi.org/10.3390/nu12041200
APA StyleJezewska-Zychowicz, M., Gębski, J., & Kobylińska, M. (2020). Food Involvement, Eating Restrictions and Dietary Patterns in Polish Adults: Expected Effects of Their Relationships (LifeStyle Study). Nutrients, 12(4), 1200. https://doi.org/10.3390/nu12041200