Nutritional Status and Oral Frailty: A Community Based Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Questionnaire
2.3. Dietary Reference Intakes for Japanese (2015)
2.4. Brief-Type Self-Administered Diet History Questionnaire (BDHQ)
2.5. Examinations
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Characteristics of the Participants
3.2. Nutritional Status and Body Mass Index
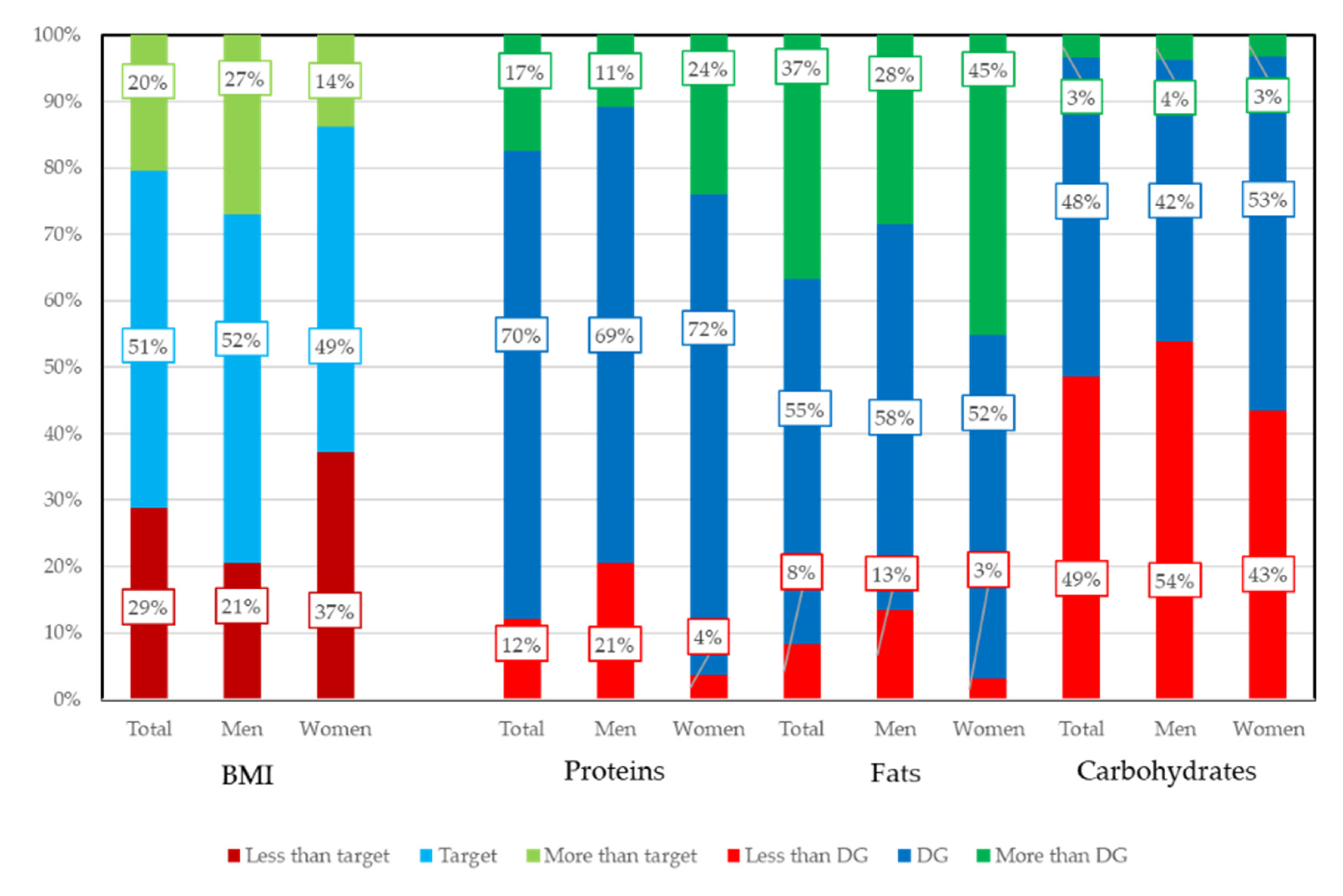
3.2.1. Proportion of Energy Intake and Body Mass Index (BMI)
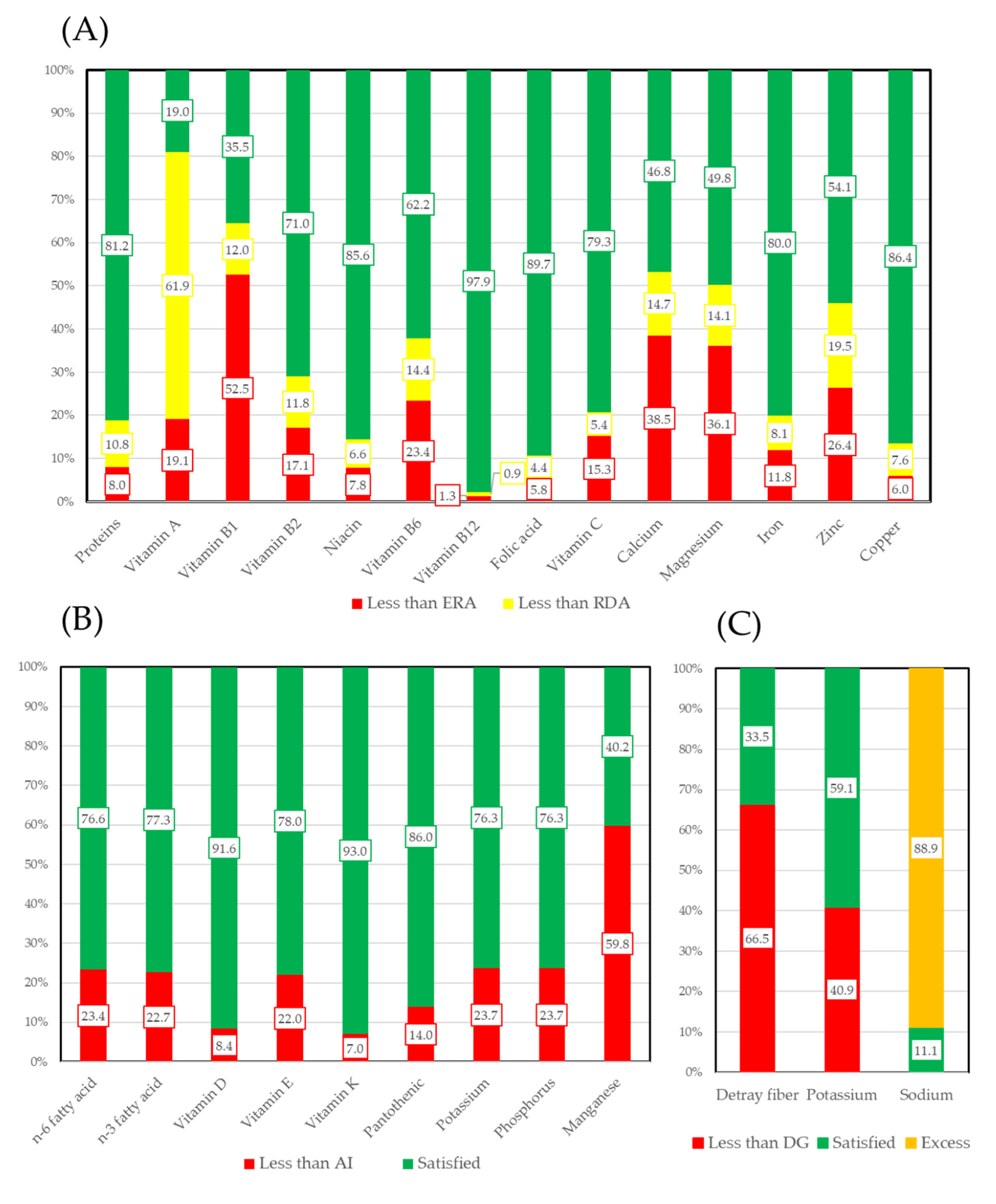
3.2.2. Vitamins, Macro Minerals, and Micro Minerals
3.3. Oral Health Status of the Participants
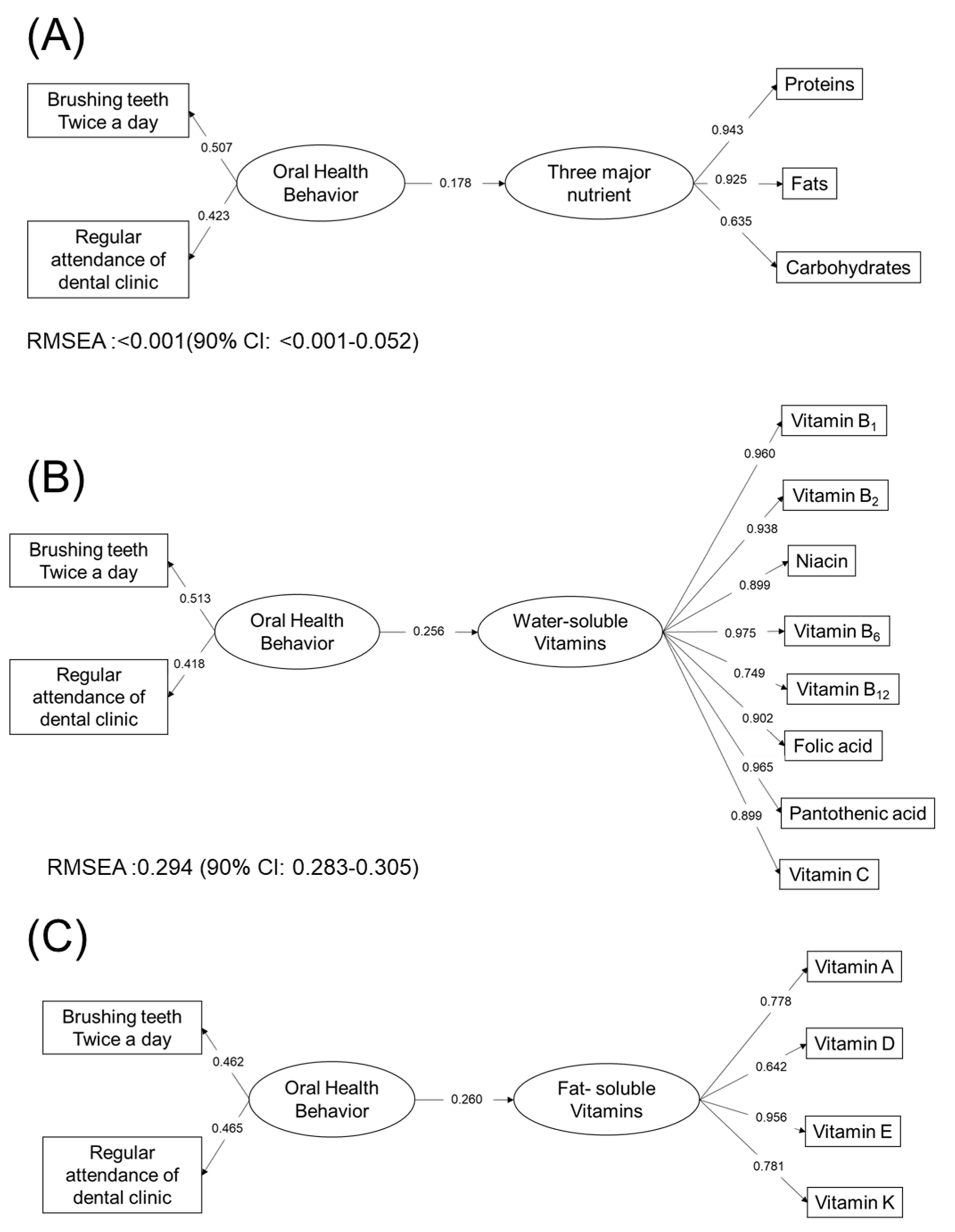
3.4. Oral Health Status and Nutritional Status
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hirschfeld, J.; Higham, J.; Chatzistavrianou, D.; Blair, F.; Richards, A.; Chapple, I.L.C. Systemic disease or periodontal disease? Distinguishing causes of gingival inflammation: A guide for dental practitioners. Part 1: Immune-Mediated, autoinflammatory, and hereditary lesions. Br. Dent. J. 2019, 227, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, J.; Higham, J.; Blair, F.; Richards, A.; Chapple, I.L.C. Systemic disease or periodontal disease? Distinguishing causes of gingival inflammation: A guide for dental practitioners. Part 2: Cancer related, infective, and other causes of gingival pathology. Br. Dent J. 2019, 227, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Ahn-Jarvis, J.H.; Piancino, M.G. Chapter 14: Impact of Oral Health on Diet/Nutrition. Monogr. Oral. Sci. 2020, 28, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, C.S.; Joshipura, K.; Hung, H.C.; Douglass, C.W. Nutrition as a mediator in the relation between oral and systemic disease: Associations between specific measures of adult oral health and nutrition outcomes. Crit. Rev. Oral. Biol. Med. 2002, 13, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Shwe, P.S.; Ward, S.; Thein, P.M.; Junckerstorff, R. Frailty, oral health and nutrition in geriatrics inpatients: A cross-sectional study. Gerodontology 2019, 36, 223–228. [Google Scholar] [CrossRef] [PubMed]
- N’gom, P.I.; Woda, A.A. Influence of impaired mastication on nutrition. J. Prosthet. Dent. 2002, 87, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Hollis, J.H. The effect of mastication on food intake, satiety and body weight. Physiol. Behav. 2018, 193, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horibe, Y.; Ueda, T.; Watanabe, Y.; Motokawa, K.; Edahiro, A.; Hirano, H.; Shirobe, M.; Ogami, K.; Kawai, H.; Obuchi, S.; et al. A 2-year longitudinal study of the relationship between masticatory function and progression to frailty or pre-frailty among community-dwelling Japanese aged 65 and older. J. Oral. Rehabil. 2018, 45, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Kakuta, E.; Okada, A.; Otsuka, R.; Shimada, M.; Tomizawa, Y.; Taguchi, C.; Arikawa, K.; Daikoku, H.; Sato, T.; et al. Effects of self-assessed chewing ability, tooth loss and serum albumin on mortality in 80-year-old individuals: A 20-year follow-up study. BMC Oral Health 2020, 20, 122. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.A.C.; Law, G.G.; Milledge, K.L.; Chu, S.K.; Hsu, B.; Valdez, E.; Naganathan, V.; Hirani, V.; Blyth, F.M.; LeCouteur, D.G.; et al. Chewing function, general health and the dentition of older Australian men: The Concord Health and Ageing in Men Project. Community Dent. Oral. Epidemiol. 2019, 47, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Kawai, H.; Yoshida, H.; Hirano, H.; Kojima, M.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Classification of frailty using the Kihon checklist: A cluster analysis of older adults in urban areas. Geriatr. Gerontol. Int. 2017, 17, 69–77. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sugars Intake for Adults and Children 2015. Available online: https://www.who.int/publications/i/item/9789241549028 (accessed on 1 September 2020).
- Valenzuela, M.J.; Waterhouse, B.; Aggarwal, V.R.; Bloor, K.; Doran, T. Effect of sugar-sweetened beverages on oral health: A systematic review and meta-analysis. Eur. J. Public Health 2020, ckaa147. [Google Scholar] [CrossRef] [PubMed]
- von Philipsborn, P.; Stratil, J.M.; Burns, J.; Busert, L.K.; Pfadenhauer, L.M.; Polus, S.; Holzapfel, C.; Hauner, H.; Rehfuess, E.A. Environmental Interventions to Reduce the Consumption of Sugar-Sweetened Beverages: Abridged Cochrane Systematic Review. Obes Facts. 2020, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.L.P.; Milledge, K.L.; O’Leary, F.; Cumming, R.; Eberhard, J.; Hirani, V. Poor dietary intake of nutrients and food groups are associated with increased risk of periodontal disease among community-dwelling older adults: A systematic literature review. Nutr. Rev. 2020, 78, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Tenelanda-López, D.; Valdivia-Moral, P.; Castro-Sánchez, M. Eating Habits and Their Relationship to Oral Health. Nutrients 2020, 12, 2619. [Google Scholar] [CrossRef] [PubMed]
- Costacurta, M.; DiRenzo, L.; Sicuro, L.; Gratteri, S.; Lorenzo, A.D.; Docimo, R. Dental caries and childhood obesity: Analysis of food intakes, lifestyle. Eur. J. Paediatr. Dent. 2014, 15, 343–348. [Google Scholar] [PubMed]
- Ministry of Health, Labor and Welfare. Overview of Dietary Reference Intakes for Japanese (2015). Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/Overview.pdf (accessed on 1 September 2020).
- Ministry of Health, Labor and Welfare. Overview of Dietary Reference Intakes for Japanese (2020). Available online: https://www.mhlw.go.jp/content/10904750/000586553.pdf (accessed on 1 September 2020).
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, K.; Kokubo, Y.; Yamanaka, T.; Watanabe, M.; Iso, H.; Okamura, T.; Miyamoto, Y. The reasonable reliability of a self-administered food frequency questionnaire for an urban, Japanese, middle-aged population: The Suita study. Nutr. Res. 2015, 35, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Yuan, X.; Sasaki, S.; Osawa, Y.; Hirata, T.; Abe, Y.; Takayama, M.; Arai, Y.; Masui, Y.; Ishizaki, T. Relative validity of brief-type self-administered diet history questionnaire among very old Japanese aged 80 years or older. Public Health Nutr. 2019, 22, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Nordenram, G.; Ryd-Kjellen, E.; Johansson, G.; Nordstrom, G.; Winblad, B. Alzheimer’s disease, oral function and nutritional status. Gerodontology 1996, 13, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. National Health and Nutrition Examination Survey (2018). Available online: https://www.mhlw.go.jp/stf/newpage_08789.html (accessed on 1 September 2020).
- Molnár, E.S.; Nagy-Lőrincz, Z.; Nagy, B.; Bakacs, M.; Kis, O.; Nagy, E.S.; Martos, É. Hungarian Diet and Nutritional Status Survey—The OTAP2014 study. V. Vitamin intake of the Hungarian population. Orv. Hetil. 2017, 158, 1302–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, B.; Nagy-Lőrincz, Z.; Bakacs, M.; Illés, É.; Nagy, E.S.; Martos, É. Hungarian Diet and Nutritional Status Survey—OTÁP2014. III. Macroelement intake of the Hungarian population]. Orv. Hetil. 2017, 158, 653–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandstetter, S.; Rüter, J.; Curbach, J.; Loss, J. A systematic review on empowerment for healthy nutrition in health promotion. Public Health Nutr. 2015, 18, 3146–3154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeuchi, H.; Terada, M.; Kobayashi, K.; Uraguchi, M.; Nomura, Y.; Hanada, N. Influences of Masticatory Function Recovery Combined with Health Guidance on Body Composition and Metabolic Parameters. Open Dent. J. 2019, 13, 124–136. [Google Scholar] [CrossRef]
- Nomura, Y.; Takeuchi, H.; Shigemoto, S.; Okada, A.; Shigeta, Y.; Ogawa, T.; Hanada, N. Secondary Endpoint of the Prosthodontics. Int. J. Clin. Case Stud. 2017, 3, IJCCS-117. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMI | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Categorical Variable | Continuous Variable | ||||||||
| Nutrients | Cut Off | n | <Target | Target Range | Target< | p-Value | Mean SD | Median 25th–75th | p-Value |
| Proteins (%) | <DG | 85 | 20 | 37 | 28 | 0.017 | 23.5 ± 3.4 * | 23.4 (20.8–25.7) | 0.032 |
| DG | 494 | 147 | 249 | 98 | 22.7 ± 3.1 | 22.5 (20.5–24.5) | |||
| DG< | 122 | 35 | 70 | 17 | 24.2 ± 22.4 * | 23.2 (20.8–23.6) | |||
| Fats (%) | <DG | 58 | 14 | 24 | 20 | 0.091 | 23.5 ± 3.3 | 23.7 (20.5–25.6) | 0.062 |
| DG | 385 | 113 | 196 | 76 | 22.6 ± 3.1 | 22.6 (20.6–24.5) | |||
| DG< | 258 | 75 | 136 | 47 | 22.6 ± 3.2 | 22.4 (20.6–24.1) | |||
| Carbohydrates (%) | <DG | 341 | 75 | 187 | 79 | 0.002 | 23.1 ± 3.1 ** | 22.9 (21.1–24.7) | 0.003 |
| DG | 336 | 116 | 160 | 60 | 22.3 ± 3.2 ** | 22.2 (20.3–24.1) | |||
| DG< | 24 | 11 | 9 | 4 | 22.2 ± 3.2 | 21.7 (20.1–24.0) | |||
| No | Yes | Missing | ||||
|---|---|---|---|---|---|---|
| Item of Oral Frailly Scorning Questionnaire | N | % | N | % | N | % |
| Difficult to eat hard food | 572 | 81.6 | 127 | 18.1 | 2 | 0.3 |
| Choking | 595 | 84.9 | 102 | 14.6 | 4 | 0.6 |
| Using denture | 371 | 52.9 | 323 | 46.1 | 7 | 1.0 |
| Xerostomia | 528 | 75.3 | 171 | 24.4 | 2 | 0.3 |
| Less frequently going out | 571 | 81.5 | 127 | 18.1 | 3 | 0.4 |
| Feasible to chew hard food | 603 | 86.0 | 96 | 13.7 | 2 | 0.3 |
| Brushing teeth at least twice a day | 542 | 77.3 | 157 | 22.4 | 2 | 0.3 |
| Regular attendance of dental clinic | 513 | 73.2 | 183 | 26.1 | 5 | 0.7 |
| Brushing Teeth at Least Twice a Day | Regular Attendance of Dental Clinic | ||||||
|---|---|---|---|---|---|---|---|
| No | Yes | p-Value | No | Yes | p-Value | ||
| Proteins | <DG | 31 | 54 | 0.001 | 25 | 60 | 0.778 |
| DG | 109 | 383 | 127 | 362 | |||
| DG< | 17 | 105 | 31 | 91 | |||
| Fats | <DG | 21 | 36 | 0.006 | 21 | 36 | 0.153 |
| DG | 90 | 294 | 99 | 282 | |||
| DG< | 46 | 212 | 63 | 195 | |||
| Carbohydrates | <DG | 74 | 267 | 0.419 | 86 | 254 | 0.085 |
| DG | 75 | 259 | 86 | 246 | |||
| DG< | 8 | 16 | 11 | 13 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, Y.; Ishii, Y.; Suzuki, S.; Morita, K.; Suzuki, A.; Suzuki, S.; Tanabe, J.; Ishiwata, Y.; Yamakawa, K.; Chiba, Y.; et al. Nutritional Status and Oral Frailty: A Community Based Study. Nutrients 2020, 12, 2886. https://doi.org/10.3390/nu12092886
Nomura Y, Ishii Y, Suzuki S, Morita K, Suzuki A, Suzuki S, Tanabe J, Ishiwata Y, Yamakawa K, Chiba Y, et al. Nutritional Status and Oral Frailty: A Community Based Study. Nutrients. 2020; 12(9):2886. https://doi.org/10.3390/nu12092886
Chicago/Turabian StyleNomura, Yoshiaki, Yoshimasa Ishii, Shunsuke Suzuki, Kenji Morita, Akira Suzuki, Senichi Suzuki, Joji Tanabe, Yasuo Ishiwata, Koji Yamakawa, Yota Chiba, and et al. 2020. "Nutritional Status and Oral Frailty: A Community Based Study" Nutrients 12, no. 9: 2886. https://doi.org/10.3390/nu12092886
APA StyleNomura, Y., Ishii, Y., Suzuki, S., Morita, K., Suzuki, A., Suzuki, S., Tanabe, J., Ishiwata, Y., Yamakawa, K., Chiba, Y., Ishikawa, M., Sogabe, K., Kakuta, E., Okada, A., Otsuka, R., & Hanada, N. (2020). Nutritional Status and Oral Frailty: A Community Based Study. Nutrients, 12(9), 2886. https://doi.org/10.3390/nu12092886