
Metabolic Profile and Bone Status in Post-Menopausal Women with Rheumatoid Arthritis: A Monocentric Retrospective Survey

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Laboratory Tests
2.3. Clinical and Functional Parameters
2.4. Ongoing Treatments
2.5. Bone Status Assessment
Bone Mineral Density
2.6. Fragility Fractures
2.7. Measurement of TBS
2.8. Statistical Analysis
3. Results
3.1. Clinical, Metabolic and Bone Parameters of the Whole Cohort of RA Patients
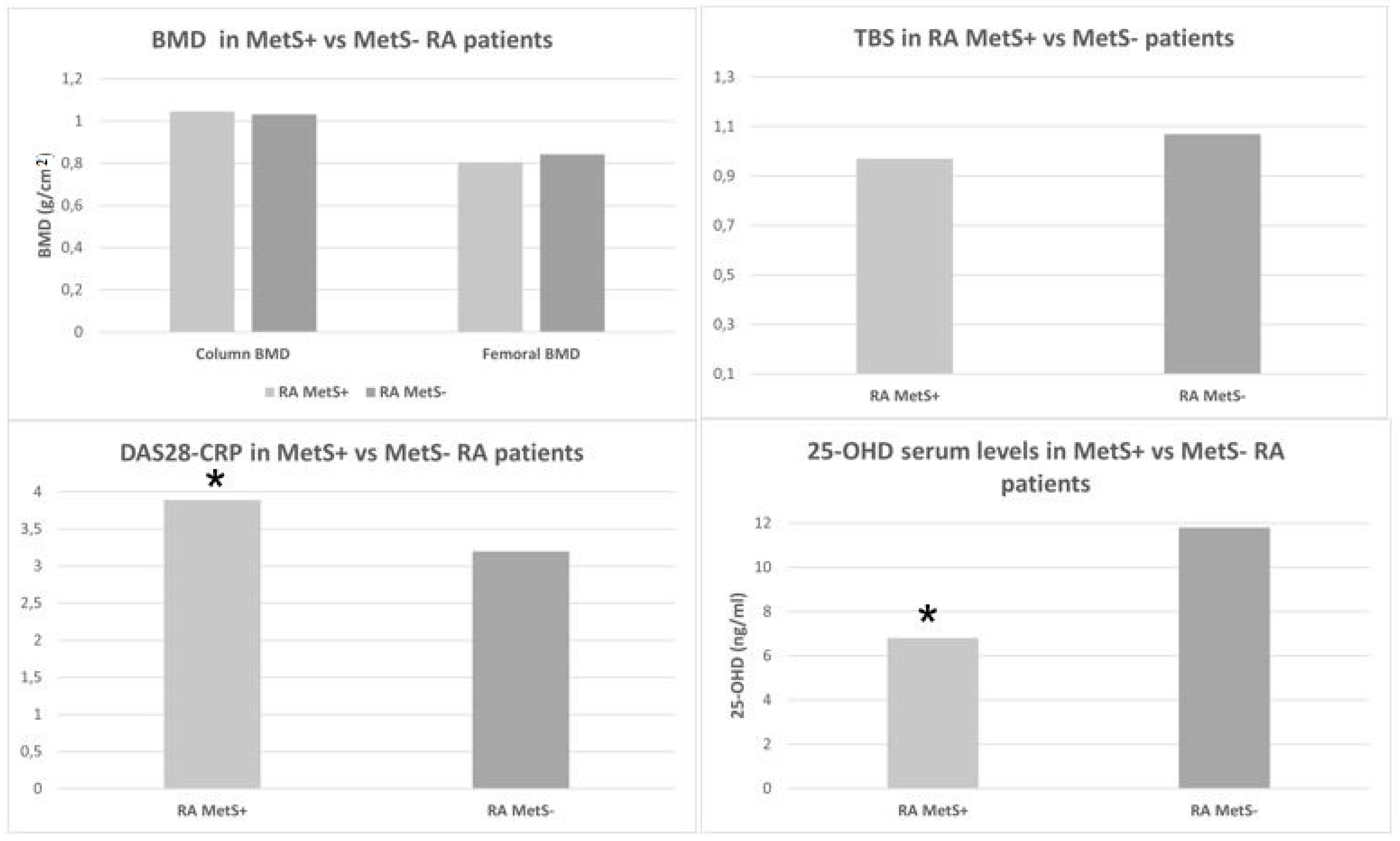
3.2. Clinical, Metabolic, and Bone Parameters of the MetS+ versus MetS− RA Patients
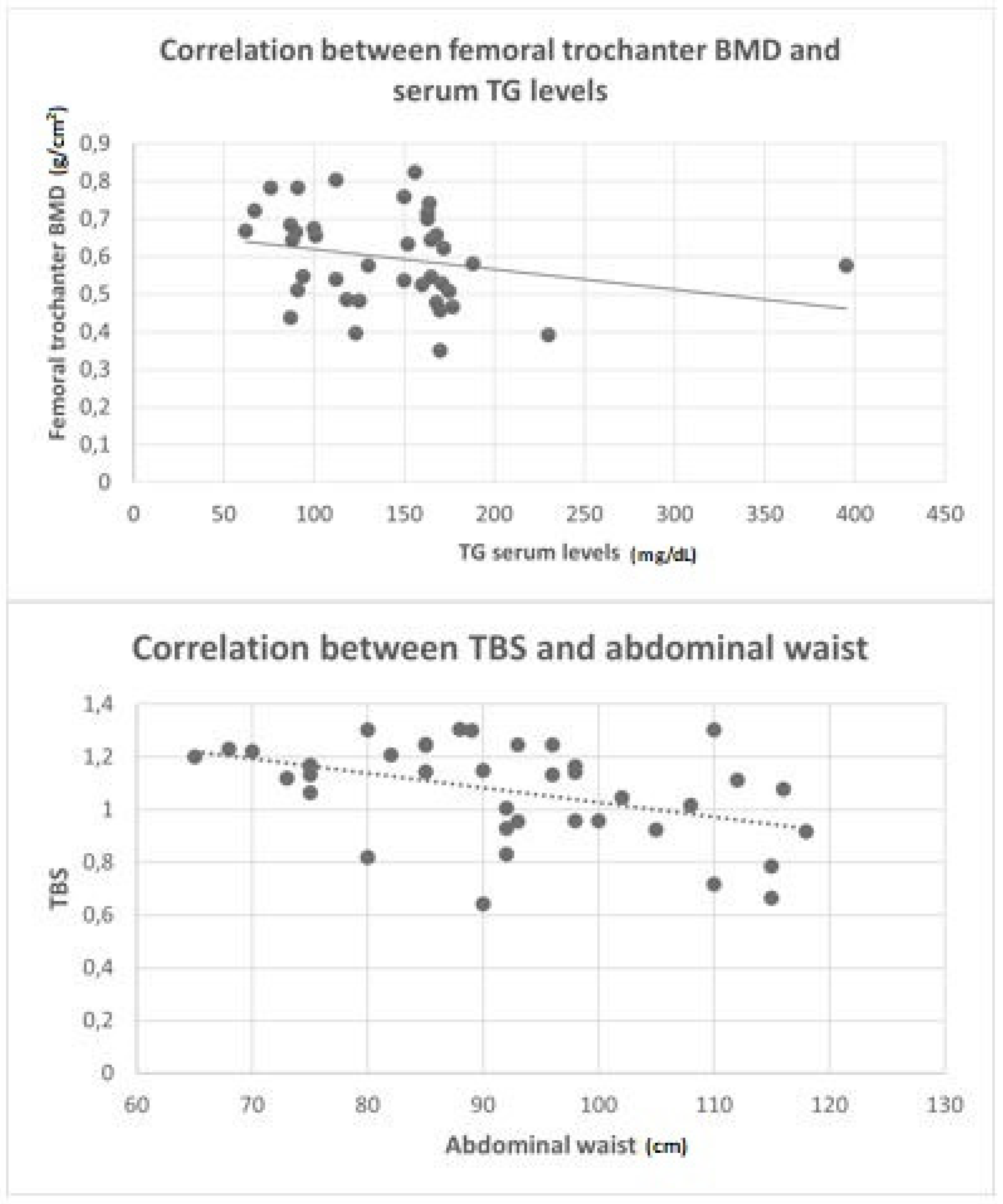
3.3. Correlations between Bone Mineral Density and Trabecular Bone Score with the Metabolic Parameters in the Whole Cohort of RA Patients
3.4. Correlations between RA Disease Activity with Metabolic Profile and Bone Status in the Whole Cohort of Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Michaud, K.; Wolfe, F. Comorbidities in rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2007, 21, 885–906. [Google Scholar] [CrossRef]
- Toms, T.E.; Symmons, D.P.; Kitas, G.D. Dyslipidaemia in rheumatoid arthritis: The role of inflammation, drugs, lifestyle and genetic factors. Curr. Vasc. Pharmacol. 2010, 8, 301–326. [Google Scholar] [CrossRef]
- Llorente, I.; García-Castañeda, N.; Valero, C.; González-Álvaro, I.; Castañeda, S. Osteoporosis in Rheumatoid Arthritis: Dangerous Liaisons. Front. Med. (Lausanne) 2020, 7, 601618. [Google Scholar] [CrossRef] [PubMed]
- Adami, G.; Saag, K.G. Osteoporosis Pathophysiology, Epidemiology, and Screening in Rheumatoid Arthritis. Curr. Rheumatol. Rep. 2019, 21, 34. [Google Scholar] [CrossRef]
- Hallajzadeh, J.; Safiri, S.; Mansournia, M.A.; Khoramdad, M.; Izadi, N.; Almasi-Hashiani, A.; Pakzad, R.; Ayubi, E.; Sullman, M.J.; Karamzad, N. Metabolic syndrome and its components among rheumatoid arthritis patients: A comprehensive updated systematic review and meta-analysis. PLoS ONE 2017, 12, e0170361. [Google Scholar] [CrossRef] [Green Version]
- Adami, G.; Fassio, A.; Rossini, M.; Caimmi, C.; Giollo, A.; Orsolini, G.; Viapiana, O.; Gatti, D. Osteoporosis in Rheumatic Diseases. Int. J. Mol. Sci. 2019, 20, 5867. [Google Scholar] [CrossRef] [Green Version]
- Muka, T.; Trajanoska, K.; Kiefte-de Jong, J.C.; Oei, L.; Uitterlinden, A.G.; Hofman, A.; Dehghan, A.; Zillikens, M.C.; Franco, O.H.; Rivadeneira, F. The Association between Metabolic Syndrome, Bone Mineral Density, Hip Bone Geometry and Fracture Risk: The Rotterdam Study. PLoS ONE 2015, 10, e0129116. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Chiodini, P.; Capuano, A.; Colao, A.; Giugliano, D. Fracture risk and bone mineral density in metabolic syndrome: A meta-analysis. J. Clin. Endocrinol. Metab. 2013, 98, 3306–3314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vis, M.; Haavardsholm, E.A.; Bøyesen, P.; Haugeberg, G.; Uhlig, T.; Hoff, M.; Woolf, A.; Dijkmans, B.; Lems, W.; Kvien, T.K. High incidence of vertebral and non-vertebral fractures in the OSTRA cohort study: A 5-year follow-up study in postmenopausal women with rheumatoid arthritis. Osteoporos. Int. 2011, 22, 2413–2419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis. Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Wells, G.; Becker, J.C.; Teng, J.; Dougados, M.; Schiff, M.; Smolen, J.; Aletaha, D.; Van Riel, P.L.C.M. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythr. Ann. Rheum. Dis. 2009, 68, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Gutch, M.; Kumar, S.; Razi, S.M.; Gupta, K.K.; Gupta, A. Assessment of insulin sensitivity/resistance. Indian J. Endocrinol. Metab. 2015, 19, 160–164. [Google Scholar] [CrossRef]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef] [PubMed]
- Sözen, T.; Özışık, L.; Başaran, N. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Genant, H.K.; Jergas, M.; Palermo, L.; Nevitt, M.; Valentin, R.S.; Black, D.; Cummings, S.R. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J. Bone Miner. Res. 1996, 11, 984–996. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Leslie, W.D.; Resch, H.; Lamy, O.; Lesnyak, O.; Binkley, N.; McCloskey, E.V.; Kanis, J.A.; Bilezikian, J.P. Trabecular Bone Score: A Noninvasive Analytical Method Based Upon the DXA Image. J. Bone Mineral. Res. 2014, 29, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Boutroy, S.; Zhang, C.; McMahon, D.J.; Zhou, B.; Wang, J.; Udesky, J.; Cremers, S.; Sarquis, M.; Guo, X.D.; et al. Trabecular bone score (TBS)--a novel method to evaluate bone microarchitectural texture in patients with primary hyperparathyroidism. J. Clin. Endocrinol. Metab. 2013, 98, 1963–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, B.; Hassanjani Roushan, M.R. Rheumatoid arthritis and osteoporosis. Casp. J. Intern. Med. 2012, 3, 445–446. [Google Scholar]
- Steffen, U.; Schett, G.; Bozec, A. How Autoantibodies Regulate Osteoclast Induced Bone Loss in Rheumatoid Arthritis. Front. Immunol. 2019, 10, 1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stemmler, F.; Simon, D.; Liphardt, A.-M.; Englbrecht, M.; Rech, J.; Hueber, A.J.; Engelke, K.; Schett, G.; Kleyer, A. Biomechanical properties of bone are impaired in patients with ACPA-positive rheumatoid arthritis and associated with the occurrence of fractures. Ann. Rheum. Dis. 2018, 77, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Xue, P.; Gao, P.; Li, Y. The association between metabolic syndrome and bone mineral density: A meta-analysis. Endocrine 2012, 42, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Liu, J.; Lu, N.; Sun, H.; Ning, G. Association between metabolic syndrome and bone fractures: A meta-analysis of observational studies. BMC Endocr. Disord. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Lv, X.; Wei, D.; Yue, F.; Guo, J.; Zhang, T. Metabolic syndrome and the risk of bone fractures: A Meta-analysis of prospective cohort studies. Bone 2016, 84, 52–56. [Google Scholar] [CrossRef]
- Hou, J.; He, C.; He, W.; Yang, M.; Luo, X.; Li, C. Obesity and Bone Health: A Complex Link. Front. Cell Dev. Biol. 2020, 8, 600181. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Choe, J.W.; Kim, H.K.; Bae, S.J.; Kim, B.J.; Lee, S.H.; Koh, J.M.; Han, K.O.; Park, H.M.; Kim, G.S. Negative association between metabolic syndrome and bone mineral density in Koreans, especially in men. Calcif. Tissue Int. 2010, 86, 350–358. [Google Scholar] [CrossRef]
- Bredella, M.A.; Gill, C.M.; Gerweck, A.V.; Landa, M.G.; Kumar, V.; Daley, S.M.; Torriani, M.; Miller, K.K. Ectopic and serum lipid levels are positively associated with bone marrow fat in obesity. Radiology 2013, 269, 534–541. [Google Scholar] [CrossRef]
- Wong, S.K.; Chin, K.Y.; Suhaimi, F.H.; Ahmad, F.; Ima-Nirwana, S. The Relationship between Metabolic Syndrome and Osteoporosis: A Review. Nutrients 2016, 8, 347. [Google Scholar] [CrossRef] [Green Version]
- McInnes, K.J.; Brown, K.A.; Knower, K.C.; Chand, A.L.; Clyne, C.D.; Simpson, E.R. Characterisation of aromatase expression in the human adipocyte cell line SGBS. Breast Cancer Res. Treat. 2008, 112, 429–435. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Kanazawa, I.; Yamamoto, M.; Kurioka, S.; Yamauchi, M.; Yano, S.; Sugimoto, T. Associations between components of the metabolic syndrome versus bone mineral density and vertebral fractures in patients with type 2 diabetes. Bone 2009, 45, 174–179. [Google Scholar] [CrossRef]
- Napoli, N.; Strollo, R.; Paladini, A.; Briganti, S.I.; Pozzilli, P.; Epstein, S. The Alliance of Mesenchymal Stem Cells, Bone, and Diabetes. Int. J. Endocrinol. 2014, 2014, 690783. [Google Scholar] [CrossRef]
- Adami, S.; Braga, V.; Zamboni, M.; Gatti, D.; Rossini, M.; Bakri, J.; Battaglia, E. Relationship between lipids and bone mass in 2 cohorts of healthy women and men. Calcif. Tissue Int. 2004, 74, 136–142. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Meilahn, E.; Zmuda, J.M.; Cauley, J.A. High blood pressure and bone-mineral loss in elderly white women: A prospective study. Study of Osteoporotic Fractures Research Group. Lancet 1999, 354, 971–975. [Google Scholar] [CrossRef]
- Hernández, J.L.; Olmos, J.M.; Pariente, E.; Martínez, J.; Valero, C.; García-Velasco, P.; Nan, D.; Llorca, J.; González-Macías, J. Metabolic syndrome and bone metabolism: The Camargo Cohort study. Menopause 2010, 17, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Ferron, M.; Clarke, C.J.; Hannun, Y.A.; Jiang, H.; Blaner, W.S.; Karsenty, G. Bone-specific insulin resistance disrupts whole-body glucose homeostasis via decreased osteocalcin activation. J. Clin. Investig. 2014, 124, 1781–1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Cunha, V.R.; Brenol, C.V.; Brenol, J.C.; Fuchs, S.C.; Arlindo, E.M.; Melo, I.M.; Machado, C.A.; de Castro Chaves, H., Jr.; Xavier, R.M. Metabolic syndrome prevalence is increased in rheumatoid arthritis patients and is associated with disease activity. Scand. J. Rheumatol. 2012, 41, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S.; Peraldi, P.; Budavari, A.; Ellis, R.; White, M.F.; Spiegelman, B.M. IRS-1-mediated inhibition of insulin receptor tyrosine kinase activity in TNF-alpha- and obesity-induced insulin resistance. Science 1996, 271, 665–668. [Google Scholar] [CrossRef]
- Scoditti, E.; Carpi, S.; Massaro, M.; Pellegrino, M.; Polini, B.; Carluccio, M.A.; Wabitsch, M.; Verri, T.; Nieri, P.; De Caterina, R. Hydroxytyrosol Modulates Adipocyte Gene and miRNA Expression Under Inflammatory Condition. Nutrients 2019, 11, 2493. [Google Scholar] [CrossRef] [Green Version]
- Lumeng, C.N.; DelProposto, J.B.; Westcott, D.J.; Saltiel, A.R. Phenotypic switching of adipose tissue macrophages with obesity is generated by spatiotemporal differences in macrophage subtypes. Diabetes 2008, 57, 3239–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tardito, S.; Martinelli, G.; Soldano, S.; Paolino, S.; Pacini, G.; Patane, M.; Alessandri, E.; Smith, V.; Cutolo, M. Macrophage M1/M2 polarization and rheumatoid arthritis: A systematic review. Autoimmun. Rev. 2019, 18, 102397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, R.K.; Dar, H.Y.; Mishra, P.K. Immunoporosis: Immunology of Osteoporosis—Role of T Cells. Front. Immunol. 2018, 9, 657. [Google Scholar] [CrossRef] [PubMed]
- Wesley, A.; Bengtsson, C.; Elkan, A.C.; Klareskog, L.; Alfredsson, L.; Wedrén, S. Association between body mass index and anti-citrullinated protein antibody-positive and anti-citrullinated protein antibody-negative rheumatoid arthritis: Results from a population-based case-control study. Arthritis Care Res. (Hoboken) 2013, 65, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Seriolo, B.; Paolino, S.; Ferrone, C.; Cutolo, M. Impact of long-term anti-TNF-alpha treatment on insulin resistance in patients with rheumatoid arthritis. Clin. Exp. Rheumatol. 2008, 26, 159–160, Author Reply 160. [Google Scholar] [PubMed]
- Drincic, A.T.; Armas, L.A.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity (Silver Spring) 2012, 20, 1444–1448. [Google Scholar] [CrossRef]
- Silveira, E.A.; Cardoso, C.K.; Moura, L.D.; dos Santos Rodrigues, A.P.; de Oliveira, C. Serum and Dietary Vitamin D in Individuals with Class II and III Obesity: Prevalence and Association with Metabolic Syndrome. Nutrients 2021, 13, 2138. [Google Scholar] [CrossRef]
- Cutolo, M.; Pizzorni, C.; Sulli, A. Vitamin D endocrine system involvement in autoimmune rheumatic diseases. Autoimmun. Rev. 2011, 11, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Otsa, K.; Uprus, M.; Paolino, S.; Seriolo, B. Vitamin D in rheumatoid arthritis. Autoimmun. Rev. 2007, 7, 59–64. [Google Scholar] [CrossRef]
- Nguyen, Y.; Sigaux, J.; Letarouilly, J.-G.; Sanchez, P.; Czernichow, S.; Flipo, R.-M.; Soubrier, M.; Semerano, L.; Seror, R.; Sellam, J.; et al. Efficacy of Oral Vitamin Supplementation in Inflammatory Rheumatic Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 107. [Google Scholar] [CrossRef]
- Mutt, S.J.; Hyppönen, E.; Saarnio, J.; Järvelin, M.-R.; Herzig, K.-H. Vitamin D and adipose tissue—More than storage. Front. Physiol. 2014, 5, 228. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Kim, J. Serum vitamin D status and metabolic syndrome: A systematic review and dose-response meta-analysis. Nutr. Res. Pract. 2021, 15, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Gremese, E.; Ferraccioli, G. The metabolic syndrome: The crossroads between rheumatoid arthritis and cardiovascular risk. Autoimmun. Rev. 2011, 10, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Kerekes, G.; Nurmohamed, M.T.; González-Gay, M.A.; Seres, I.; Paragh, G.; Kardos, Z.; Baráth, Z.; Tamási, L.; Soltész, P.; Szekanecz, Z. Rheumatoid arthritis and metabolic syndrome. Nature Rev. Rheumatol. 2014, 10, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Boini, S.; Guillemin, F. Radiographic scoring methods as outcome measures in rheumatoid arthritis: Properties and advantages. Ann. Rheum. Dis. 2001, 60, 817–827. [Google Scholar]
- Cutolo, M.; Plebani, M.; Shoenfeld, Y.; Adorini, L.; Tincani, A. Vitamin D endocrine system and the immune response in rheumatic diseases. Vitam. Horm. 2011, 86, 327–351. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical, Metabolic and Bone Variables | N = 39 |
|---|---|
| Age (mean ± SD, years) | 66.6 ± 10.4 |
| Disease duration (mean ± SD, years) | 3 ± 2.7 |
| Weight (mean ± SD, kg) | 68.3 ± 12.6 |
| Height (mean ± SD, cm) | 162 ± 7 |
| BMI (mean ± SD, Kg/m2) | 25.9 ± 3.8 |
| Previous osteoporosis related fractures, n (%) | 5/39 (12.8%) |
| Waist circumference, (mean ± SD, cm) | 90.6 ± 13 |
| Systolic BP value (mean ± SD, mmHg) | 137.6 ± 11.6 |
| Diastolic BP (mean ± SD, mmHg) | 79.8 ± 7.6 |
| CRP (mean ± SD, mg/L) | 10 ± 12.6 |
| ESR (mean ± SD, mm/h) | 49.6 ± 28.5 |
| DAS28-CRP (mean ± SD, units) | 3.03 ± 0.95 |
| RF seropositivity, n (%) | 15/39 (38.4%) |
| ACPA seropositivity, n (%) | 10/39 (25.6%) |
| Current PDN treatment, n (%) | 100% |
| Current oral PDN, dose, (mean ± SD, mg/day) | 5.3 ± 0.91 |
| Patients treated with PDN ≤ 2.5 mg daily, n (%) | 10/39 (25.6%) |
| Patients treated with 5 mg daily PDN, n (%) | 20/39 (51.3%) |
| Patients treated with PDN dosages ranging from 7.5 to 10 mg daily, n (%) | 7/39 (18%) |
| Patients treated with PDN dosages > 10 mg daily, n (%) | 2/39 (5.1%) |
| Current csDMARD, n (%) | 36/39 (92.3%) |
| Current bDMARD or tsDMARD, n (%) | 5/39 (12.8%) |
| Lipids and Metabolic Profile | |
| TC (mean ± SD, mg/dL) | 215 ± 38.6 |
| LDL-C (mean ± SD, mg/dL) | 129 ± 34.3 |
| HDL-C (mean ± SD, mg/dL) | 64.5 ± 19.5 |
| TG (mean ± SD, mg/dL) | 122.3 ± 37 |
| ApoA1 (mean ± SD, g/L) | 1.7 ± 0.4 |
| ApoB (mean ± SD, g/L) | 1.2 ± 1.4 |
| FG (mean ± SD, mg/dL) | 85 ± 13.5 |
| Insulin, mean ± SD, µ/mL | 10 ± 4.3 |
| HOMA-I (mean ± SD) | 2.04 ± 1.04 |
| 25(OH)D (mean ± SD, ng/mL) | 11 ± 6.5 |
| PTH (mean ± SD, ng/L) | 26.9 ± 16.9 |
| Ca (mean ± SD, mg/mL) | 9.5 ± 0.32 |
| P (mean ± SD, mg/mL) | 3.3 ± 0.5 |
| ALP-b (mean ± SD, µg/L) | 9.33 ± 7.48 |
| Bone Parameters | |
| L1–L4 BMD (mean ± SD, g/cm2) | 1.1 ± 0.17 |
| L1–L4 T-score (mean ± SD) | −1.1 ± 1.5 |
| Total femur BMD (mean ± SD, g/cm2) | 0.85 ± 0.11 |
| Total femur T-score (mean ± SD) | −1.4 ± 1.0 |
| Femoral neck BMD (mean ± SD, g/cm2) | 0.77 ± 0.1 |
| Femoral neck T-score (mean ± SD) | −1.8 ± 0.94 |
| Femoral trochanter BMD (mean ± SD, g/cm2) | 0.61 ± 0.12 |
| Femoral trochanter T-score (mean ± SD) | −2.3 ± 0.9 |
| TBS (mean ± SD) | 1.058 ± 0.19 |
| MetS+ N = 13 | MetS− N = 26 | p-Value | |
|---|---|---|---|
| Age (mean ± SD, years) | 73 ± 6.3 | 64 ± 9.9 | 0.009 |
| Disease duration (mean ± SD, years) | 3.1 ± 3.1 | 2.8 ± 1.2 | ns |
| Weight (mean ± SD, kg) | 79.3 ± 18.5 | 65.3 ± 12.1 | 0.001 |
| Height (mean ± SD, cm) | 160.8 ± 7 | 163.1 ± 7.7 | ns |
| BMI (mean ± SD, Kg/m2) | 30.5 ± 6.1 | 24.4 ± 3.0 | 0.0007 |
| Previous OP related fractures, n (%) | 4/13 (30%) | 4/16 (19%) | ns |
| AW (mean ± SD, cm) | 101.2 ± 12.7 | 87.4 ± 13.2 | 0.004 |
| Systolic BP value (mean ± SD, mmHg) | 142.3 ± 11 | 135.2 ± 11.3 | ns |
| Diastolic BP (mean ± SD, mmHg) | 84.2 ± 7.3 | 77.6 ± 6.9 | ns |
| CRP (mean ± SD, mg/L) | 11.2 ± 8.4 | 9.5 ± 14.0 | ns |
| ESR (mean ± SD) | 63.7 ± 28.4 | 50.8 ± 32.2 | ns |
| DAS28-CRP (mean ± SD, units) | 3.89 ± 0.97 | 3.2 ± 0.83 | 0.04 |
| RF seropositivity, n (%) | 5/13 (34.5%) | 10/16 (62.5%) | ns |
| ACPA seropositivity, n (%) | 5/13 (34.5%) | 5/26 (19.3%) | ns |
| Current PDN, n (%) | 100% | 100% | |
| Current oral PDN, dose (mean ± SD, mg/day) | 5.5 ± 1 | 5.4 ± 1 | ns |
| Current csDMARD, n (%) | 11/13 (84.6%) | 12/26 (46%) | 0.02 |
| Current bDMARD, n (%) | 2/13 (15.3%) | 2/26 (11.5%) | ns |
| Current tsDMARD, n (%) | 0/13 (0%) | 1/26 (3.8%) | ns |
| Lipids and Metabolic Profile | |||
| TC (mean ± SD, mg/dL) | 179.2 ± 72.7 | 123 ± 37.6 | 0.008 |
| LDL-C (mean ± SD, mg/dL) | 145.5 ± 39 | 122.7 ± 34.5 | Ns |
| HDL-C (mean ± SD, mg/dL) | 63.5 ± 16.5 | 69 ± 22.6 | Ns |
| ApoA1 (mean ± SD, g/L) | 1.6 ± 0.27 | 1.86 ± 0.47 | Ns |
| ApoB (mean ± SD, g/L) | 1.0 ± 0.21 | 1.20 ± 1.4 | Ns |
| FG (mean ± SD, mg/dL) | 92.9 ± 14.2 | 80.3 ± 11.5 | 0.01 |
| Insulin, (mean ± SD, µ/mL) | 15.4 ± 4.3 | 8.7 ± 3.8 | 0.0001 |
| HOMA-I (mean ± SD) | 3.4 ± 0.61 | 1.6 ± 0.81 | <0.0001 |
| 25(OH)D (mean ± SD, ng/mL) | 6.8 ± 2.4 | 11.8 ± 6.7 | 0.01 |
| PTH (mean ± SD, ng/L) | 29.4 ± 23.12 | 25 ± 11.43 | Ns |
| Ca (mean ± SD, mg/mL) | 9.6 ± 0.43 | 9.5 ± 0.23 | Ns |
| P (mean ± SD, mg/mL) | 3.4 ± 0.6 | 3.3 ± 0.47 | Ns |
| ALP-b (mean ± SD, µg/L) | 7.5 ± 4 | 10.5 ± 8.89 | Ns |
| Bone Parameters | |||
| L1–L4 BMD (mean ± SD, g/cm2) | 1 ± 0.17 | 1.03 ± 0.15 | ns |
| L1–L4 T-score (mean ± SD) | −1.1 ± 1.5 | −1.1 ± 1.3 | ns |
| Total femur BMD (mean ± SD, g/cm2) | 0.80 ± 0.13 | 0.84 ± 0.12 | ns |
| Total femur T-score (mean ± SD) | −1.6 ± 1.0 | −1.4 ± 1.1 | ns |
| Femoral neck BMD (mean ± SD, g/cm2) | 0.74 ± 0.1 | 0.78 ± 0.11 | ns |
| Femoral neck T-score (mean ± SD) | −1.9 ± 0.8 | −1.6 ± 0.9 | ns |
| Femoral trochanter BMD (mean ± SD, g/cm2) | 0.55 ± 0.11 | 0.61 ± 0.12 | ns |
| Femoral trochanter T-score (mean ± SD) | −2.7 ± 0.9 | −2.2 ± 0.93 | ns |
| TBS (mean ± SD) | 0.970 ± 0.17 | 1.07 ± 0.17 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paolino, S.; Hysa, E.; Stoian, S.A.; Gotelli, E.; Casabella, A.; Clini, P.V.; Pacini, G.; Pizzorni, C.; Sulli, A.; Nikiphorou, E.; et al. Metabolic Profile and Bone Status in Post-Menopausal Women with Rheumatoid Arthritis: A Monocentric Retrospective Survey. Nutrients 2021, 13, 3168. https://doi.org/10.3390/nu13093168
Paolino S, Hysa E, Stoian SA, Gotelli E, Casabella A, Clini PV, Pacini G, Pizzorni C, Sulli A, Nikiphorou E, et al. Metabolic Profile and Bone Status in Post-Menopausal Women with Rheumatoid Arthritis: A Monocentric Retrospective Survey. Nutrients. 2021; 13(9):3168. https://doi.org/10.3390/nu13093168
Chicago/Turabian StylePaolino, Sabrina, Elvis Hysa, Sabrina Atena Stoian, Emanuele Gotelli, Andrea Casabella, Paolo Vittoriano Clini, Greta Pacini, Carmen Pizzorni, Alberto Sulli, Elena Nikiphorou, and et al. 2021. "Metabolic Profile and Bone Status in Post-Menopausal Women with Rheumatoid Arthritis: A Monocentric Retrospective Survey" Nutrients 13, no. 9: 3168. https://doi.org/10.3390/nu13093168
APA StylePaolino, S., Hysa, E., Stoian, S. A., Gotelli, E., Casabella, A., Clini, P. V., Pacini, G., Pizzorni, C., Sulli, A., Nikiphorou, E., Smith, V., & Cutolo, M. (2021). Metabolic Profile and Bone Status in Post-Menopausal Women with Rheumatoid Arthritis: A Monocentric Retrospective Survey. Nutrients, 13(9), 3168. https://doi.org/10.3390/nu13093168