
Propolis and Its Gastroprotective Effects on NSAID-Induced Gastric Ulcer Disease: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
1.1. NSAIDs Adverse Effects
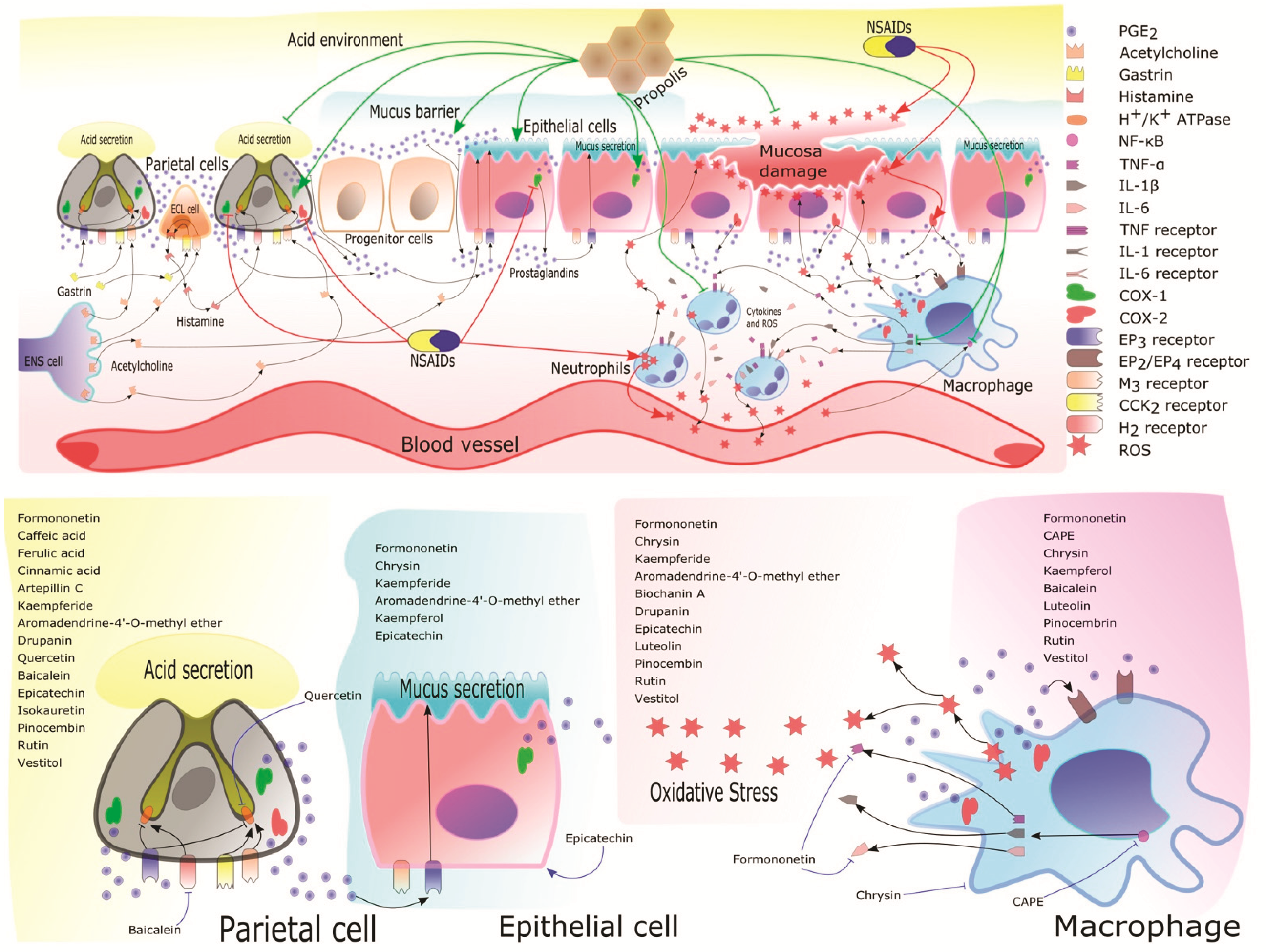
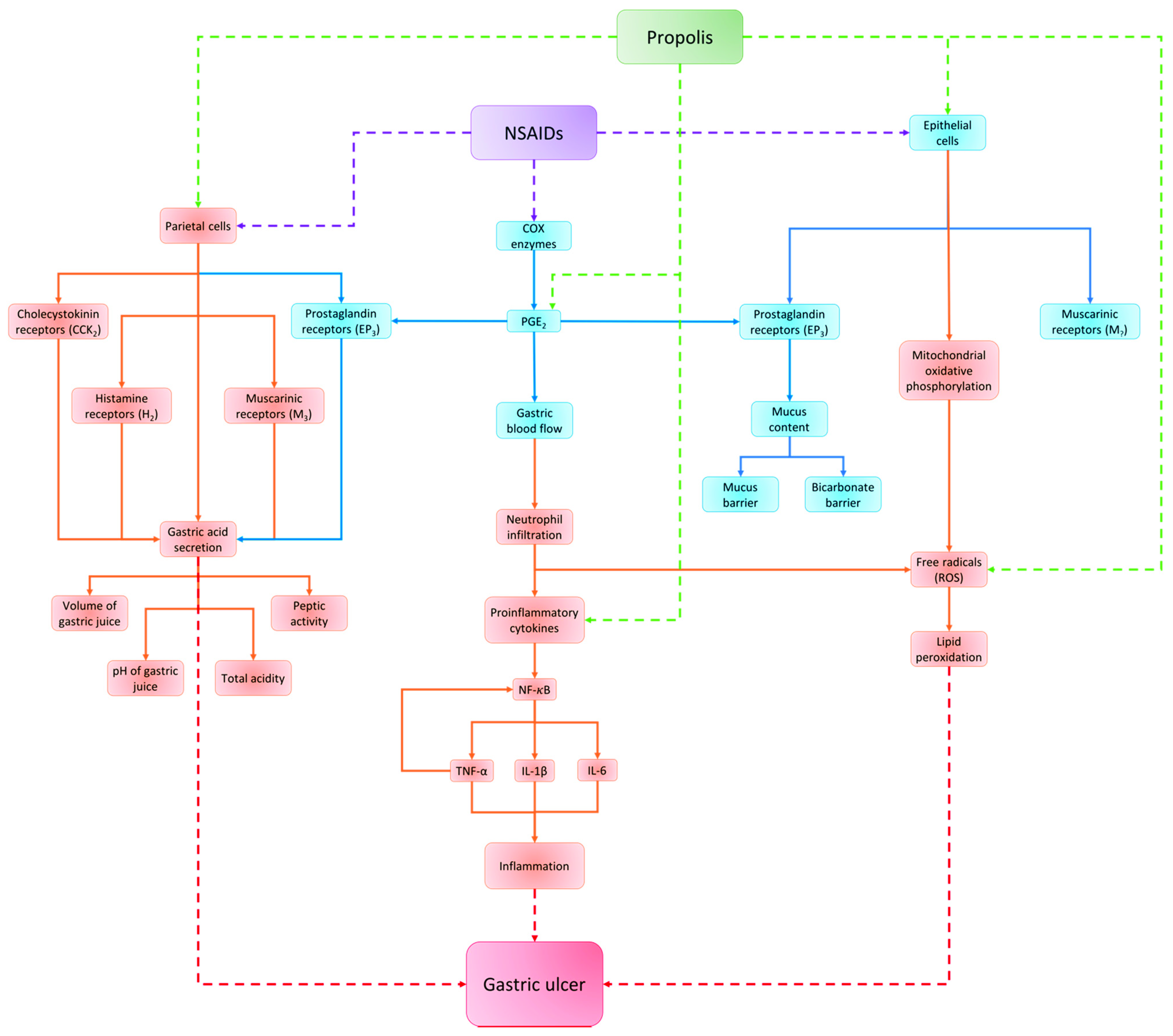
1.2. Mechanism of NSAIDs to Induce GI Damage
1.3. Gastric Ulcer Disease
1.4. Actual Therapy for the Treatment of Gastric Ulcer Disease and Its Side Effects
1.5. Folk Medicine and Its Relevance as a Source of New Treatments
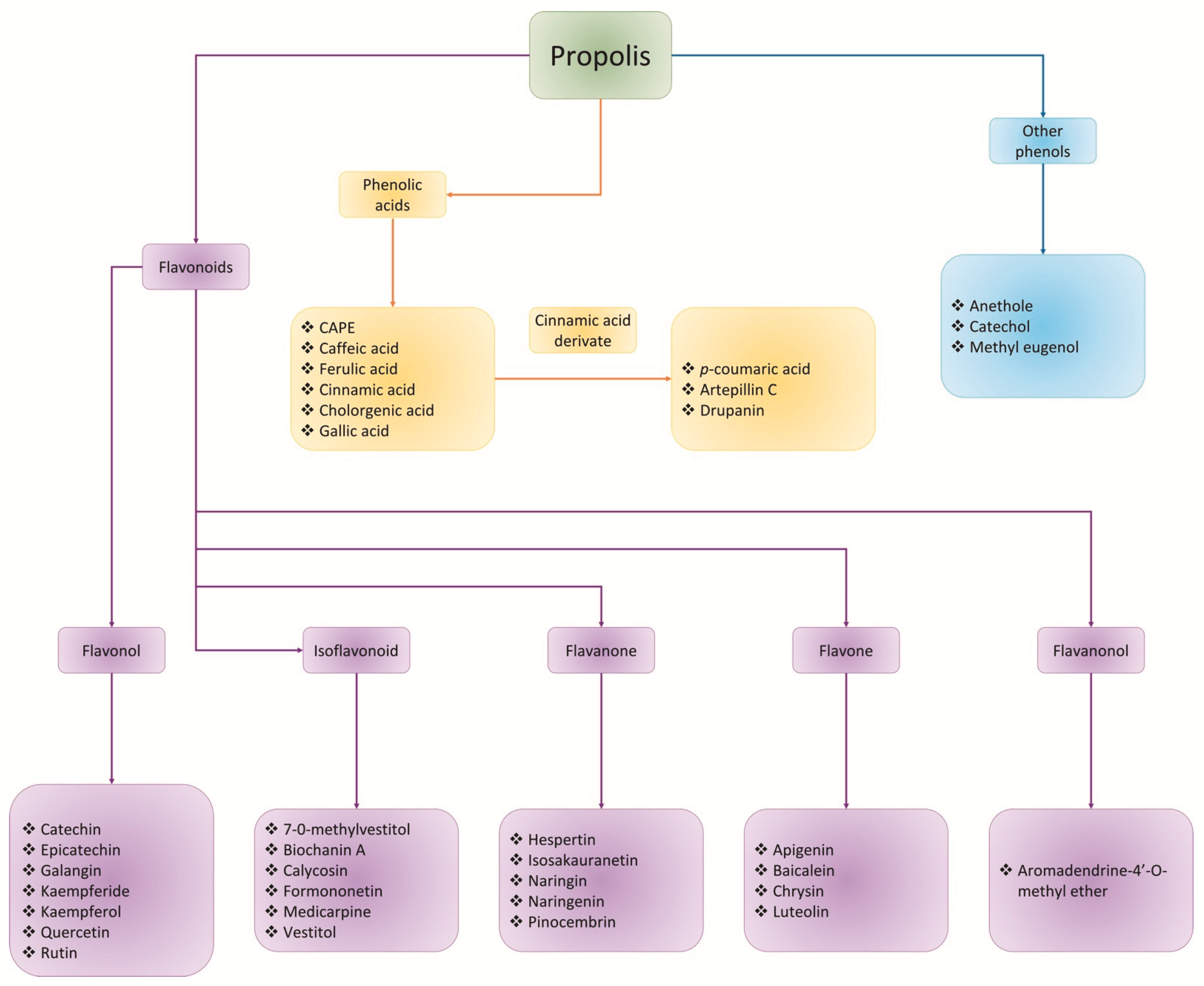
1.6. Propolis: An Old Known Substance with Gastroprotective Potential
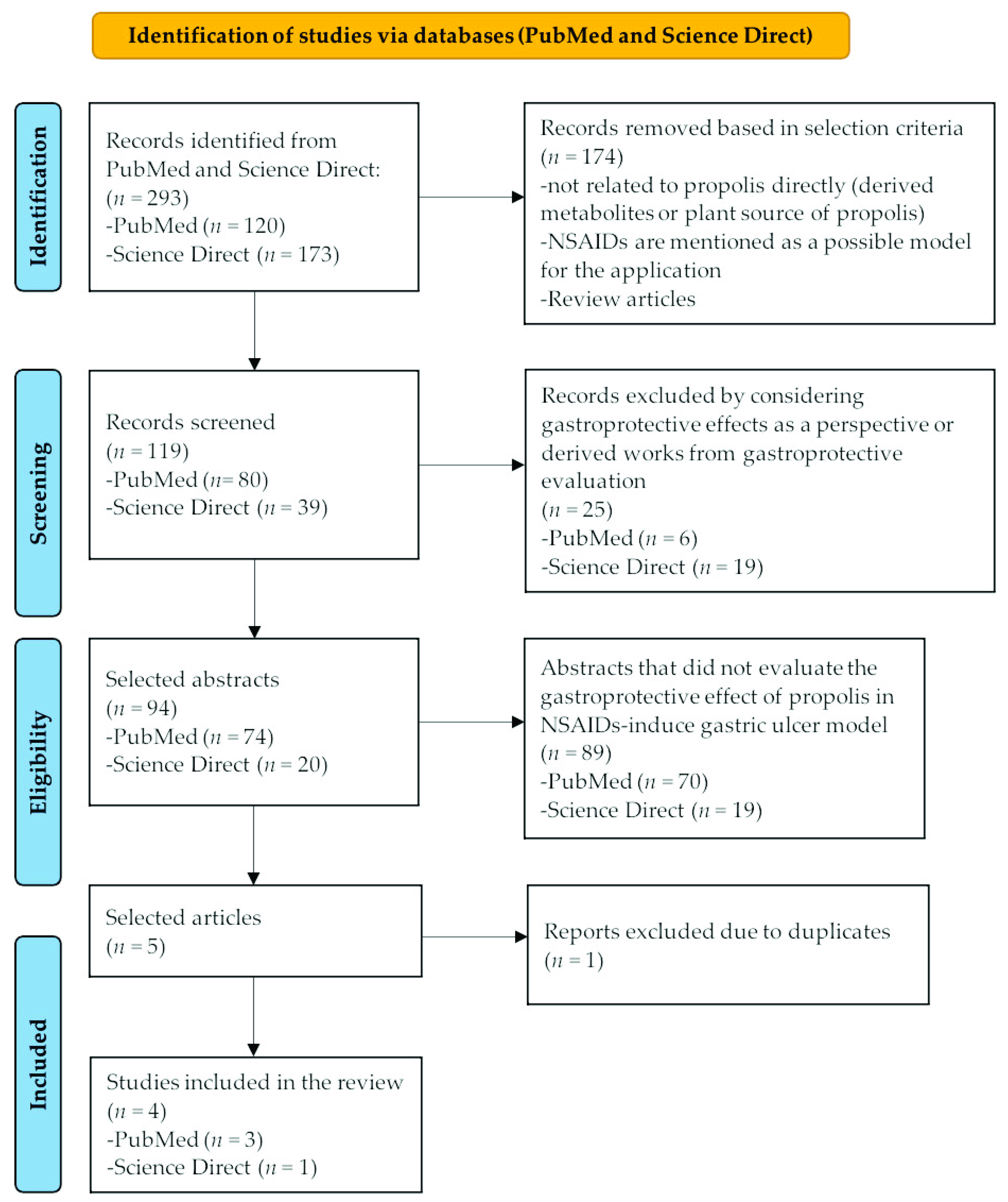
2. Materials and Methods
3. Results
3.1. Selection and Study Characteristics
3.2. Effect of the Propolis in Gastric Ulcer Healing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halter, F.; Tarnawski, A.; Schmassmann, A.; Peskar, B. Cyclooxygenase 2—Implications on maintenance of gastric mucosal integrity and ulcer healing: Controversial issues and perspectives. Gut 2001, 49, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K. Pathogenesis of NSAID-induced gastric damage: Importance of cyclooxygenase inhibition and gastric hypermotility. World J. Gastroenterol. WJG 2012, 18, 2147. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, H.; Albayrak, A.; Bilici, M.; Cadirci, E.; Halici, Z. Different mechanisms in formation and prevention of indomethacin-induced gastric ulcers. Inflammation 2010, 33, 224–234. [Google Scholar] [CrossRef]
- García-Rayado, G.; Navarro, M.; Lanas, A. NSAID induced gastrointestinal damage and designing GI-sparing NSAIDs. Expert Rev. Clin. Pharmacol. 2018, 11, 1031–1043. [Google Scholar] [CrossRef]
- Wallace, J.L. Recent advances in gastric ulcer therapeutics. Curr. Opin. Pharmacol. 2005, 5, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Fazalda, A.; Quraisiah, A.; Nur Azlina, M.F. Antiulcer effect of honey in nonsteroidal anti-inflammatory drugs induced gastric ulcer model in rats: A systematic review. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Holle, G. Pathophysiology and modern treatment of ulcer disease. Int. J. Mol. Med. 2010, 25, 483–491. [Google Scholar] [CrossRef] [Green Version]
- Silva, L.M.d.; Souza, P.d.; Jaouni, S.K.A.; Harakeh, S.; Golbabapour, S.; de Andrade, S.F. Propolis and its potential to treat gastrointestinal disorders. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kuna, L.; Jakab, J.; Smolic, R.; Raguz-Lucic, N.; Vcev, A.; Smolic, M. Peptic ulcer disease: A brief review of conventional therapy and herbal treatment options. J. Clin. Med. 2019, 8, 179. [Google Scholar] [CrossRef] [Green Version]
- Díaz, L. Gastric mucosa: Protective mechanisms and harmful effects of acetylsalicylic acid. Physiol. Biochem. Approaches. Med. E Investig. 2016, 3, 100–103. [Google Scholar]
- Kinoshita, Y.; Ishimura, N.; Ishihara, S. Advantages and disadvantages of long-term proton pump inhibitor use. J. Neurogastroenterol. Motil. 2018, 24, 182. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M.; Menon, J.; Muiandy, R.; Fredie, R.; Sein, M.; Fariz, A. Risk Factors, Diagnosis, and Management of Peptic ulcer Disease. IOSR J. Dent. Med. Sci. Sabah Malays. 2015, 14, 40–46. [Google Scholar]
- Vanderhoff, B.T.; Tahboub, R. Proton pump inhibitors: An update. Am. Fam. Physician 2002, 66, 273. [Google Scholar]
- Yu, L.-Y.; Sun, L.-N.; Zhang, X.-H.; Li, Y.-Q.; Yu, L.; Meng, L.; Zhang, H.-W.; Wang, Y.-Q. A review of the novel application and potential adverse effects of proton pump inhibitors. Adv. Ther. 2017, 34, 1070–1086. [Google Scholar] [CrossRef]
- Aparicio Mena, A.J. Traditional medicine as eco-cultural medicine. Gaz. Antropol. 2005, 21, 1–9. [Google Scholar]
- Canales Martínez, M.; Hernández Delgado, T.; Caballero Nieto, J.; Romo de Vivar Romo, A.; Durán Díaz, Á.; Lira Saade, R. Análisis cuantitativo del conocimiento tradicional de las plantas medicinales en San Rafael, Coxcatlán, Valle de Tehuacán-Cuicatlán, Puebla, México. Acta Bot. Mex. 2006, 75, 21–43. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Traditional Medicine Strategy: 2014–2023; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- McChesney, J.D.; Venkataraman, S.K.; Henri, J.T. Plant natural products: Back to the future or into extinction? Phytochemistry 2007, 68, 2015–2022. [Google Scholar] [CrossRef]
- Dias, D.A.; Urban, S.; Roessner, U. A historical overview of natural products in drug discovery. Metabolites 2012, 2, 303–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balunas, M.J.; Kinghorn, A.D. Drug discovery from medicinal plants. Life Sci. 2005, 78, 431–441. [Google Scholar] [CrossRef]
- Falcão, H.; Mariath, I.; Diniz, M.; Batista, L.; Barbosa-Filho, J. Plants of the American continent with antiulcer activity. Phytomedicine 2008, 15, 132–146. [Google Scholar] [CrossRef]
- Adhikary, B.; Yadav, S.K.; Roy, K.; Bandyopadhyay, S.K.; Chattopadhyay, S. Black tea and theaflavins assist healing of indomethacin-induced gastric ulceration in mice by antioxidative action. Evid.-Based Complement. Altern. Med. 2011, 2011, 1–11. [Google Scholar] [CrossRef]
- Phillipson, J.D. Phytochemistry and medicinal plants. Phytochemistry 2001, 56, 237–243. [Google Scholar] [CrossRef]
- Rates, S.M. Plants as source of drugs. Toxicon Off. J. Int. Soc. Toxinol. 2001, 39, 603–613. [Google Scholar] [CrossRef]
- Loraine, S.; Mendoza-Espinoza, J.A. Las plantas medicinales en la lucha contra el cáncer, relevancia para México. Rev. Mex. De Cienc. Farm. 2010, 41, 18–27. [Google Scholar]
- Castaldo, S.; Capasso, F. Propolis, an old remedy used in modern medicine. Fitoterapia 2002, 73 (Suppl. 1), S1–S6. [Google Scholar] [CrossRef]
- Burdock, G.A. Review of the biological properties and toxicity of bee propolis (propolis). Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 1998, 36, 347–363. [Google Scholar] [CrossRef]
- Pietta, P.G.; Gardana, C.; Pietta, A.M. Analytical methods for quality control of propolis. Fitoterapia 2002, 73 (Suppl. 1), S7–S20. [Google Scholar] [CrossRef]
- Volpi, N.; Bergonzini, G. Analysis of flavonoids from propolis by on-line HPLC-electrospray mass spectrometry. J. Pharm. Biomed. Anal. 2006, 42, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Sforcin, J.M.; Bankova, V. Propolis: Is there a potential for the development of new drugs? J. Ethnopharmacol. 2011, 133, 253–260. [Google Scholar] [CrossRef]
- Kumazawa, S.; Hamasaka, T.; Nakayama, T. Antioxidant activity of propolis of various geographic origins. Food Chem. 2004, 84, 329–339. [Google Scholar] [CrossRef]
- Sawicka, D.; Car, H.; Borawska, M.H.; Niklinski, J. The anticancer activity of propolis. Folia Histochem. Cytobiol. Pol. Acad. Sci. Pol. Histochem. Cytochem. Soc. 2012, 50, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Khalil, M.L. Biological activity of bee propolis in health and disease. Asian Pac. J. Cancer Prev. APJCP 2006, 7, 22–31. [Google Scholar]
- Chan, G.C.; Cheung, K.W.; Sze, D.M. The immunomodulatory and anticancer properties of propolis. Clin. Rev. Allergy Immunol. 2013, 44, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Yañez, N.; Rivera-Yañez, C.R.; Pozo-Molina, G.; Méndez-Catalá, C.F.; Méndez-Cruz, A.R.; Nieto-Yañez, O. Biomedical Properties of Propolis on Diverse Chronic Diseases and Its Potential Applications and Health Benefits. Nutrients 2021, 13, 78. [Google Scholar] [CrossRef] [PubMed]
- Bastos, E.M.; Simone, M.; Jorge, D.M.; Soares, A.E.; Spivak, M. In vitro study of the antimicrobial activity of Brazilian propolis against Paenibacillus larvae. J. Invertebr. Pathol. 2008, 97, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Grange, J.M.; Davey, R.W. Antibacterial properties of propolis (bee glue). J. R. Soc. Med. 1990, 83, 159–160. [Google Scholar] [CrossRef]
- Kilic, A.; Baysallar, M.; Besirbellioglu, B.; Salih, B.; Sorkun, K.; Tanyuksel, M. In vitro antimicrobial activity of propolis against methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus faecium. Ann. Microbiol. 2005, 55, 113–117. [Google Scholar]
- Velazquez, C.; Navarro, M.; Acosta, A.; Angulo, A.; Dominguez, Z.; Robles, R.; Robles-Zepeda, R.; Lugo, E.; Goycoolea, F.M.; Velazquez, E.F.; et al. Antibacterial and free-radical scavenging activities of Sonoran propolis. J. Appl. Microbiol. 2007, 103, 1747–1756. [Google Scholar] [CrossRef]
- Silici, S.; Koc, A.N. Comparative study of in vitro methods to analyse the antifungal activity of propolis against yeasts isolated from patients with superficial mycoses. Lett. Appl. Microbiol. 2006, 43, 318–324. [Google Scholar] [CrossRef]
- Koc, A.N.; Silici, S.; Mutlu-Sariguzel, F.; Sagdic, O. Antifungal activity of propolis in four different fruit juices. Food Technol. Biotechnol. 2007, 45, 57–61. [Google Scholar]
- Hendi, N.K.; Naher, H.S.; Al-Charrakh, A.H. In vitro antibacterial and antifungal activity of Iraqi propolis. J. Med. Plants Res. 2011, 5, 5058–5066. [Google Scholar]
- Sforcin, J.M.; Fernandes, A., Jr.; Lopes, C.A.; Bankova, V.; Funari, S.R. Seasonal effect on Brazilian propolis antibacterial activity. J. Ethnopharmacol. 2000, 73, 243–249. [Google Scholar] [CrossRef]
- Lu, L.C.; Chen, Y.W.; Chou, C.C. Antibacterial activity of propolis against Staphylococcus aureus. Int. J. Food Microbiol. 2005, 102, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Jastrzebska-Stojko, Z.; Stojko, R.; Rzepecka-Stojko, A.; Kabala-Dzik, A.; Stojko, J. Biological activity of propolis-honey balm in the treatment of experimentally-evoked burn wounds. Molecules 2013, 18, 14397–14413. [Google Scholar] [CrossRef] [Green Version]
- Lopes-Rocha, R.; Miranda, J.; Lima, N.L.; Ferreira, F.O.; Santos, A.; Verli, F.D.; Marinho, S. Effect of topical propolis and dexamethasone on the healing of oral surgical wounds: Original research. Wound Health S. Afr. 2012, 5, 25–30. [Google Scholar]
- Barroso, P.R.; Lopes-Rocha, R.; Pereira, E.M.; Marinho, S.A.; de Miranda, J.L.; Lima, N.L.; Verli, F.D. Effect of propolis on mast cells in wound healing. Inflammopharmacology 2012, 20, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.A.; Libério, S.A.; Guerra, R.N.; Ribeiro, M.N.S.; Nascimento, F.R. Mechanisms of action underlying the anti-inflammatory and immunomodulatory effects of propolis: A brief review. Rev. Bras. Farmacogn. 2012, 22, 208–219. [Google Scholar] [CrossRef] [Green Version]
- Ramos, A.; Miranda, J.d. Propolis: A review of its anti-inflammatory and healing actions. J. Venom. Anim. Toxins Incl. Trop. Dis. 2007, 13, 697–710. [Google Scholar] [CrossRef]
- Park, E.-H.; Kim, S.-H.; Park, S.-S. Anti-inflammatory activity of propolis. Arch. Pharm. Res. 1996, 19, 337–341. [Google Scholar] [CrossRef]
- Lima, L.D.; Andrade, S.P.; Campos, P.P.; Barcelos, L.S.; Soriani, F.M.; Moura, S.A.; Ferreira, M.A. Brazilian green propolis modulates inflammation, angiogenesis and fibrogenesis in intraperitoneal implant in mice. BMC Complement. Altern Med. 2014, 14, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, J.L.; Assunçao, A.K.M.; da Silva, M.C.P.; Reis, A.S.d.; Costa, G.C.; Arruda, D.d.S.; Rocha, B.A.; Vaz, M.M.d.O.L.L.; Paes, A.M.d.A.; Guerra, R.N.M. Brazilian green propolis: Anti-inflammatory property by an immunomodulatory activity. Evid.-Based Complement. Altern. Med. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Hu, X.; Xuan, Y.; Ying, J.; Fei, Y.; Rong, J.; Zhang, Y.; Zhang, J.; Liu, C.; Liu, Z. Kaempferol protects ethanol-induced gastric ulcers in mice via pro-inflammatory cytokines and NO. Acta Biochim. Biophys. Sin. 2018, 50, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Beber, A.P.; de Souza, P.; Boeing, T.; Somensi, L.B.; Mariano, L.N.B.; Cury, B.J.; Burci, L.M.; da Silva, C.B.; Simionatto, E.; de Andrade, S.F. Constituents of leaves from Bauhinia curvula Benth. exert gastroprotective activity in rodents: Role of quercitrin and kaempferol. Inflammopharmacology 2018, 26, 539–550. [Google Scholar] [CrossRef]
- Ribeiro, A.R.S.; do Nascimento Valença, J.D.; da Silva Santos, J.; Boeing, T.; da Silva, L.M.; de Andrade, S.F.; Albuquerque-Júnior, R.L.; Thomazzi, S.M. The effects of baicalein on gastric mucosal ulcerations in mice: Protective pathways and anti-secretory mechanisms. Chem.-Biol. Interact. 2016, 260, 33–41. [Google Scholar] [CrossRef] [PubMed]
- George, M.Y.; Esmat, A.; Tadros, M.G.; El-Demerdash, E. In vivo cellular and molecular gastroprotective mechanisms of chrysin; Emphasis on oxidative stress, inflammation and angiogenesis. Eur. J. Pharmacol. 2018, 818, 486–498. [Google Scholar] [CrossRef] [PubMed]
- de Barros, M.P.; Sousa, J.P.B.; Bastos, J.K.; de Andrade, S.F. Effect of Brazilian green propolis on experimental gastric ulcers in rats. J. Ethnopharmacol. 2007, 110, 567–571. [Google Scholar] [CrossRef] [PubMed]
- El-Ghazaly, M.A.; Rashed, R.R.; Khayyal, M.T. Anti-ulcerogenic effect of aqueous propolis extract and the influence of radiation exposure. Int. J. Radiat. Biol. 2011, 87, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- de Mendonça, M.A.; Ribeiro, A.R.; Lima, A.K.d.; Bezerra, G.B.; Pinheiro, M.S.; de Albuquerque-Júnior, R.L.; Gomes, M.Z.; Padilha, F.F.; Thomazzi, S.M.; Novellino, E. Red propolis and its dyslipidemic regulator formononetin: Evaluation of antioxidant activity and gastroprotective effects in rat model of gastric ulcer. Nutrients 2020, 12, 2951. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Hurtado, P.A.; Garduño-Siciliano, L.; Dominguez-Verano, P.; Martinez-Galero, E.; Canales-Martinez, M.M.; Rodriguez-Monroy, M.A. Evaluation of the gastroprotective effects of Chihuahua propolis on indomethacin-induced gastric ulcers in mouse. Biomed. Pharmacother. 2021, 137, 111345. [Google Scholar] [CrossRef]
- Nakamura, T.; Ohta, Y.; Tada, M.; Teruya, A.; Ohashi, K.; Ikeno, K.; Watanabe, R.; Tokunaga, K.; Harada, N. Protective effect of Brazilian propolis ethanol extract against stress-induced gastric mucosal lesions in rats. Its evaluation using oxidative stress markers. J. Anal. Bio-Sci. Vol. 2011, 34, 135–146. [Google Scholar]
- Costa, P.; Somensi, L.B.; Mariano, L.N.B.; Boeing, T.; Longo, B.; Perfoll, E.; de Souza, P.; Gushiken, L.F.S.; Pellizzon, C.H.; Rodrigues, D.M. Role of the antioxidant properties in the gastroprotective and gastric healing activity promoted by Brazilian green propolis and the healing efficacy of Artepillin C. Inflammopharmacology 2019, 28, 1009–1025. [Google Scholar] [CrossRef] [PubMed]
- Boeing, T.; Mejía, J.A.A.; Ccana-Ccapatinta, G.V.; Mariott, M.; de Souza, P.; Mariano, L.N.B.; Oliveira, G.R.; da Rocha, I.M.; da Costa, G.A.; de Andrade, S.F. The gastroprotective effect of red propolis extract from Northeastern Brazil and the role of its isolated compounds. J. Ethnopharmacol. 2021, 267, 113623. [Google Scholar] [CrossRef] [PubMed]
- CzarneCki Ryszard, L.T. Effect of propolis on the healing of ethanol-and acetic acid-induced chronic gastric ulcer in rats. Acta Biol. Crac. Ser. Zool. 2010, 52, 37–43. [Google Scholar]
- Liu, C.-F.; Lin, C.-C.; Lin, M.-H.; Lin, Y.-S.; Lin, S.-C. Cytoprotection by propolis ethanol extract of acute absolute ethanol-induced gastric mucosal lesions. Am. J. Chin. Med. 2002, 30, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Song, M.-Y.; Lee, D.-Y.; Kim, E.-H. Anti-inflammatory and anti-oxidative effect of Korean propolis on Helicobacter pylori-induced gastric damage in vitro. J. Microbiol. 2020, 58, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Paulino, N.; Coutinho, L.A.; Coutinho, J.R.; Vilela, G.C.; da Silva Leandro, V.P.; Paulino, A.S. Antiulcerogenic effect of Brazilian propolis formulation in mice. Pharmacol. Pharm. 2015, 6, 580. [Google Scholar] [CrossRef] [Green Version]
- Costa, P.; Almeida, M.O.; Lemos, M.; Arruda, C.; Casoti, R.; Somensi, L.B.; Boeing, T.; Mariott, M.; Stein, B.D.P.; de Souza, P. Artepillin C, drupanin, aromadendrin-4′-O-methyl-ether and kaempferide from Brazilian green propolis promote gastroprotective action by diversified mode of action. J. Ethnopharmacol. 2018, 226, 82–89. [Google Scholar] [CrossRef]
- Tapia, A.; Rodriguez, J.; Theoduloz, C.; Lopez, S.; Feresin, G.E.; Schmeda-Hirschmann, G. Free radical scavengers and antioxidants from Baccharis grisebachii. J. Ethnopharmacol. 2004, 95, 155–161. [Google Scholar] [CrossRef]
- Guzmán-Gutiérrez, S.L.; Nieto-Camacho, A.; Castillo-Arellano, J.I.; Huerta-Salazar, E.; Hernández-Pasteur, G.; Silva-Miranda, M.; Argüello-Nájera, O.; Sepúlveda-Robles, O.; Espitia, C.I.; Reyes-Chilpa, R. Mexican propolis: A source of antioxidants and anti-inflammatory compounds, and isolation of a novel chalcone and ε-caprolactone derivative. Molecules 2018, 23, 334. [Google Scholar] [CrossRef] [Green Version]
- Conti, B.J.; Búfalo, M.C.; Golim, M.d.A.; Bankova, V.; Sforcin, J.M. Cinnamic acid is partially involved in propolis immunomodulatory action on human monocytes. Evid.-Based Complement. Altern. Med. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Tiveron, A.P.; Rosalen, P.L.; Franchin, M.; Lacerda, R.C.C.; Bueno-Silva, B.; Benso, B.; Denny, C.; Ikegaki, M.; Alencar, S.M.d. Chemical characterization and antioxidant, antimicrobial, and anti-inflammatory activities of South Brazilian organic propolis. PLoS ONE 2016, 11, e0165588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Liu, M.; He, J.; Li, K.; Zhang, X.; Yin, G. Identification and determination of seven phenolic acids in Brazilian green propolis by UPLC-ESI-QTOF-MS and HPLC. Molecules 2019, 24, 1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakanishi, I.; Uto, Y.; Ohkubo, K.; Miyazaki, K.; Yakumaru, H.; Urano, S.; Okuda, H.; Ueda, J.-I.; Ozawa, T.; Fukuhara, K. Efficient radical scavenging ability of artepillin C, a major component of Brazilian propolis, and the mechanism. Org. Biomol. Chem. 2003, 1, 1452–1454. [Google Scholar] [CrossRef] [PubMed]
- Shahinozzaman, M.; Basak, B.; Emran, R.; Rozario, P.; Obanda, D. Artepillin C: A comprehensive review of its chemistry, bioavailability, and pharmacological properties. Fitoterapia 2020, 147, 104775. [Google Scholar] [CrossRef]
- Rivero-Cruz, J.F.; Granados-Pineda, J.; Pedraza-Chaverri, J.; Pérez-Rojas, J.M.; Kumar-Passari, A.; Diaz-Ruiz, G.; Rivero-Cruz, B.E. Phytochemical constituents, antioxidant, cytotoxic, and antimicrobial activities of the ethanolic extract of Mexican brown propolis. Antioxidants 2020, 9, 70. [Google Scholar] [CrossRef] [Green Version]
- Granados-Pineda, J.; Uribe-Uribe, N.; García-López, P.; Ramos-Godinez, M.D.P.; Rivero-Cruz, J.F.; Pérez-Rojas, J.M. Effect of pinocembrin isolated from Mexican brown propolis on diabetic nephropathy. Molecules 2018, 23, 852. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Yañez, N.; Rodriguez-Canales, M.; Nieto-Yañez, O.; Jimenez-Estrada, M.; Ibarra-Barajas, M.; Canales-Martinez, M.; Rodriguez-Monroy, M. Hypoglycaemic and antioxidant effects of propolis of Chihuahua in a model of experimental diabetes. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas-Sánchez, R.D.; Torrescano-Urrutia, G.R.; Torres-Martínez, B.d.M.; Pateiro, M.; Lorenzo, J.M.; Sánchez-Escalante, A. Propolis extract as antioxidant to improve oxidative stability of fresh patties during refrigerated storage. Foods 2019, 8, 614. [Google Scholar] [CrossRef] [Green Version]
- de Morais, D.V.; Rosalen, P.L.; Ikegaki, M.; de Souza Silva, A.P.; Massarioli, A.P.; Alencar, S.M.d. Active antioxidant phenolics from Brazilian red propolis: An optimization study for their recovery and identification by LC-ESI-QTOF-MS/MS. Antioxidants 2021, 10, 297. [Google Scholar] [CrossRef]
- Zhao, N.; Dong, Q.; Fu, X.-X.; Du, L.-L.; Cheng, X.; Du, Y.-M.; Liao, Y.-H. Acacetin blocks kv1. 3 channels and inhibits human T cell activation. Cell. Physiol. Biochem. 2014, 34, 1359–1372. [Google Scholar] [CrossRef]
- Han, W.-M.; Chen, X.-C.; Li, G.-R.; Wang, Y. Acacetin protects against high glucose-induced endothelial cells injury by preserving mitochondrial function via activating Sirt1/Sirt3/AMPK signals. Front. Pharmacol. 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rufatto, L.C.; Luchtenberg, P.; Garcia, C.; Thomassigny, C.; Bouttier, S.; Henriques, J.A.P.; Roesch-Ely, M.; Dumas, F.; Moura, S. Brazilian red propolis: Chemical composition and antibacterial activity determined using bioguided fractionation. Microbiol. Res. 2018, 214, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Hu, R.; Li, J.; Xing, X.; Chen, J.; Zhou, Q.; Sun, J. Alpinetin exerts anti-inflammatory, anti-oxidative and anti-angiogenic effects through activating the Nrf2 pathway and inhibiting NLRP3 pathway in carbon tetrachloride-induced liver fibrosis. Int. Immunopharmacol. 2021, 96, 107660. [Google Scholar] [CrossRef]
- Valenzuela, B.; Rodríguez, F.E.; Modak, B.; Imarai, M. Alpinone exhibited immunomodulatory and antiviral activities in Atlantic salmon. Fish Shellfish. Immunol. 2018, 74, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Marinov, V.; Valcheva-Kuzmanova, S. Review on the pharmacological activities of anethole. Scr. Sci. Pharm. 2015, 2, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Ritter, A.M.V.; Hernandes, L.; da Rocha, B.A.; Estevao-Silva, C.F.; Wisniewski-Rebecca, E.S.; dos Santos Cezar, J.; Caparroz-Assef, S.M.; Cuman, R.K.N.; Bersani-Amado, C.A. Anethole reduces inflammation and joint damage in rats with adjuvant-induced arthritis. Inflamm. Res. 2017, 66, 725–737. [Google Scholar] [CrossRef]
- de Lira Mota, K.S.; Dias, G.E.N.; Pinto, M.E.F.; Luiz-Ferreira, Â.; Monteiro Souza-Brito, A.R.; Hiruma-Lima, C.A.; Barbosa-Filho, J.M.; Batista, L.M. Flavonoids with gastroprotective activity. Molecules 2009, 14, 979–1012. [Google Scholar] [CrossRef] [Green Version]
- Hosseinzade, A.; Sadeghi, O.; Naghdipour Biregani, A.; Soukhtehzari, S.; Brandt, G.S.; Esmaillzadeh, A. Immunomodulatory effects of flavonoids: Possible induction of T CD4+ regulatory cells through suppression of mTOR pathway signaling activity. Front. Immunol. 2019, 10, 51. [Google Scholar] [CrossRef] [Green Version]
- Franck, T.; Mouithys-Mickalad, A.; Robert, T.; Ghitti, G.; Neven, P.; Serteyn, D. Antioxidant and anti-inflammatory like properties of benzoic acid analogs on the oxidant response of neutrophils: Structure/redox potential relationship study. Free Radic. Biol. Med. 2012, 53, S112–S113. [Google Scholar] [CrossRef]
- López, B.G.-C.; Schmidt, E.M.; Eberlin, M.N.; Sawaya, A.C. Phytochemical markers of different types of red propolis. Food Chem. 2014, 146, 174–180. [Google Scholar] [CrossRef]
- Hajrezaie, M.; Salehen, N.; Karimian, H.; Zahedifard, M.; Shams, K.; Al Batran, R.; Majid, N.A.; Khalifa, S.A.; Ali, H.M.; El-Seedi, H. Biochanin a gastroprotective effects in ethanol-induced gastric mucosal ulceration in rats. PLoS ONE 2015, 10, e0121529. [Google Scholar]
- Govindasami, S.; Uddandrao, V.V.; Raveendran, N.; Sasikumar, V. Therapeutic Potential of biochanin-A against isoproterenol-induced myocardial infarction in rats. Cardiovasc. Hematol. Agents Med. Chem. 2020, 18, 31–36. [Google Scholar] [CrossRef]
- Xue, Z.; Zhang, Q.; Yu, W.; Wen, H.; Hou, X.; Li, D.; Kou, X. Potential lipid-lowering mechanisms of biochanin A. J. Agric. Food Chem. 2017, 65, 3842–3850. [Google Scholar] [CrossRef]
- Fukai, T.; Marumo, A.; Kaitou, K.; Kanda, T.; Terada, S.; Nomura, T. Anti-Helicobacter pylori flavonoids from licorice extract. Life Sci. 2002, 71, 1449–1463. [Google Scholar] [CrossRef]
- Wang, W.; Tang, L.; Li, Y.; Wang, Y. Biochanin A protects against focal cerebral ischemia/reperfusion in rats via inhibition of p38-mediated inflammatory responses. J. Neurol. Sci. 2015, 348, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Kundu, A.; Saha, S.; Walia, S.; Ahluwalia, V.; Kaur, C. Antioxidant potential of essential oil and cadinene sesquiterpenes of Eupatorium adenophorum. Toxicol. Environ. Chem. 2013, 95, 127–137. [Google Scholar] [CrossRef]
- De Barros, M.P.; Lemos, M.; Maistro, E.L.; Leite, M.F.; Sousa, J.P.B.; Bastos, J.K.; de Andrade, S.F. Evaluation of antiulcer activity of the main phenolic acids found in Brazilian Green Propolis. J. Ethnopharmacol. 2008, 120, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.H.d.O.; Barreto, G.d.A.; Cerqueira, J.C.; Anjos, J.P.d.; Andrade, L.N.; Padilha, F.F.; Druzian, J.I.; Machado, B.A.S. Evaluation of the antioxidant profile and cytotoxic activity of red propolis extracts from different regions of northeastern Brazil obtained by conventional and ultrasound-assisted extraction. PLoS ONE 2019, 14, e0219063. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, J.K.; Kim, H.S.; Chung, S.T.; Eom, J.H.; Kim, K.A.; Chung, S.J.; Paik, S.Y.; Oh, H.Y. Immunomodulatory effect of caffeic acid phenethyl ester in Balb/c mice. Int. Immunopharmacol. 2004, 4, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.S.; Jeong, D.; Yi, Y.-S.; Park, J.G.; Seo, H.; Moh, S.H.; Hong, S.; Cho, J.Y. IRAK1/4-targeted anti-inflammatory action of caffeic acid. Mediat. Inflamm. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Stavchansky, S.; Bowman, P.D.; Kerwin, S.M. Cytoprotective effect of caffeic acid phenethyl ester (CAPE) and catechol ring-fluorinated CAPE derivatives against menadione-induced oxidative stress in human endothelial cells. Bioorg. Med. Chem. 2006, 14, 4879–4887. [Google Scholar] [CrossRef] [PubMed]
- Ganeshpurkar, A.; Ganeshpurkar, A.; Bansal, D.; Dubey, N. Biological evaluation of ferulic acid as potent immunomodulator: An in vitro study. Int. J. Green Pharm. 2014, 8, 130–134. [Google Scholar] [CrossRef]
- Alday-Provencio, S.; Diaz, G.; Rascon, L.; Quintero, J.; Alday, E.; Robles-Zepeda, R.; Garibay-Escobar, A.; Astiazaran, H.; Hernandez, J.; Velazquez, C. Sonoran propolis and some of its chemical constituents inhibit in vitro growth of Giardia lamblia trophozoites. Planta Med. 2015, 81, 742–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunberger, D.; Banerjee, R.; Eisinger, K.; Oltz, E.; Efros, L.; Caldwell, M.; Estevez, V.; Nakanishi, K. Preferential cytotoxicity on tumor cells by caffeic acid phenethyl ester isolated from propolis. Experientia 1988, 44, 230–232. [Google Scholar] [CrossRef]
- Natarajan, K.; Singh, S.; Burke, T.R.; Grunberger, D.; Aggarwal, B.B. Caffeic acid phenethyl ester is a potent and specific inhibitor of activation of nuclear transcription factor NF-kappa B. Proc. Natl. Acad. Sci. USA 1996, 93, 9090–9095. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.S.; Park, W.S.; Jung, W.-K.; Qian, Z.-j.; Lee, D.-S.; Choi, J.-S.; Lee, D.-Y.; Park, S.-G.; Seo, S.-K.; Kim, H.-J. Caffeic acid phenethyl ester promotes anti-inflammatory effects by inhibiting MAPK and NF-κB signaling in activated HMC-1 human mast cells. Pharm. Biol. 2014, 52, 926–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.-C.; Lin, Y.-L.; Liang, Y.-C.; Yang, Y.-H.; Lee, J.-H.; Yu, H.-H.; Wu, W.-M.; Chiang, B.-L. The effect of caffeic acid phenethyl ester on the functions of human monocyte-derived dendritic cells. BMC Immunol. 2009, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, F.; Posadas, I.; Capasso, R.; Aviello, G.; Ascione, V.; Capasso, F. Effect of caffeic acid phenethyl ester on gastric acid secretion in vitro. Eur. J. Pharmacol. 2005, 521, 139–143. [Google Scholar] [CrossRef]
- Li, D.; Zhao, L.; Li, Y.; Kang, X.; Zhang, S. Gastro-Protective Effects of Calycosin Against Precancerous Lesions of Gastric Carcinoma in Rats. Drug Des. Dev. Ther. 2020, 14, 2207. [Google Scholar] [CrossRef]
- Devequi-Nunes, D.; Machado, B.A.S.; Barreto, G.d.A.; Rebouças Silva, J.; da Silva, D.F.; da Rocha, J.L.C.; Brandão, H.N.; Borges, V.M.; Umsza-Guez, M.A. Chemical characterization and biological activity of six different extracts of propolis through conventional methods and supercritical extraction. PLoS ONE 2018, 13, e0207676. [Google Scholar] [CrossRef]
- Ahmadi, S.M.; Farhoosh, R.; Sharif, A.; Rezaie, M. Structure-Antioxidant Activity Relationships of Luteolin and Catechin. J. Food Sci. 2020, 85, 298–305. [Google Scholar] [CrossRef]
- González-Manzano, S.; Dueñas, M.; Surco-Laos, F.; Hidalgo, M.; González-Paramas, A.; Santos-Buelga, C.; de Pascual-Teresa, S. In vitro evaluation of the antioxidant and anti-inflammatory activities of sulphated metabolites of catechins Evaluación in vitro de las actividades antioxidante y antiinflamatoria de metabolitos sulfatados de catequinas. CyTA-J. Food 2011, 9, 257–264. [Google Scholar] [CrossRef]
- Garro, M.F.; Ibáñez, A.G.S.; Vega, A.E.; Sosa, A.C.A.; Pelzer, L.; Saad, J.R.; Maria, A.O. Gastroprotective effects and antimicrobial activity of Lithraea molleoides and isolated compounds against Helicobacter pylori. J. Ethnopharmacol. 2015, 176, 469–474. [Google Scholar] [CrossRef]
- Zheng, L.T.; Ryu, G.-M.; Kwon, B.-M.; Lee, W.-H.; Suk, K. Anti-inflammatory effects of catechols in lipopolysaccharide-stimulated microglia cells: Inhibition of microglial neurotoxicity. Eur. J. Pharmacol. 2008, 588, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, A.T.; Santin, J.R.; Machado, I.D.; e Silva, A.M.d.O.; de Melo, I.L.P.; Mancini-Filho, J.; Farsky, S.H. Antiulcerogenic activity of chlorogenic acid in different models of gastric ulcer. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2013, 386, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Pfeiffer, P.; Alday, E.; Carreño, A.L.; Hernández-Tánori, J.; Montaño-Leyva, B.; Ortega-García, J.; Valdez, J.; Garibay-Escobar, A.; Hernandez, J.; Valencia, D. Seasonality Modulates the Cellular Antioxidant Activity and Antiproliferative Effect of Sonoran Desert Propolis. Antioxidants 2020, 9, 1294. [Google Scholar] [CrossRef] [PubMed]
- Pontiki, E.; Hadjipavlou-Litina, D. Multi-target cinnamic acids for oxidative stress and inflammation: Design, synthesis, biological evaluation and modeling studies. Molecules 2019, 24, 12. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.; Lee, J.-H.; Bae, K.H.; Jeong, C.-S. Anti-gastric actions of eugenol and cinnamic acid isolated from Cinnamomi Ramulus. Yakugaku Zasshi 2011, 131, 1103–1110. [Google Scholar] [CrossRef] [Green Version]
- Hämäläinen, M.; Nieminen, R.; Vuorela, P.; Heinonen, M.; Moilanen, E. Anti-inflammatory effects of flavonoids: Genistein, kaempferol, quercetin, and daidzein inhibit STAT-1 and NF-κB activations, whereas flavone, isorhamnetin, naringenin, and pelargonidin inhibit only NF-κB activation along with their inhibitory effect on iNOS expression and NO production in activated macrophages. Mediat. Inflamm. 2007, 2007, 1–10. [Google Scholar]
- Dwiecki, K.; Neunert, G.; Polewski, P.; Polewski, K. Antioxidant activity of daidzein, a natural antioxidant, and its spectroscopic properties in organic solvents and phosphatidylcholine liposomes. J. Photochem. Photobiol. B Biol. 2009, 96, 242–248. [Google Scholar] [CrossRef]
- Ferreira, J.M.; Fernandes-Silva, C.C.; Salatino, A.; Negri, G.; Message, D. New propolis type from north-east Brazil: Chemical composition, antioxidant activity and botanical origin. J. Sci. Food Agric. 2017, 97, 3552–3558. [Google Scholar] [CrossRef] [PubMed]
- Rozza, A.; Hiruma-Lima, C.A.; Tanimoto, A.; Pellizzon, C. Morphologic and pharmacological investigations in the epicatechin gastroprotective effect. Evid.-Based Complement. Altern. Med. 2012, 2012, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Yin, Z.N.; Wu, W.J.; Sun, C.Z.; Liu, H.F.; Chen, W.B.; Zhan, Q.P.; Lei, Z.G.; Xuan, X.; Juan, J.; Kun, Y. Antioxidant and anti-inflammatory capacity of ferulic acid released from wheat bran by solid-state fermentation of Aspergillus Niger. Biomed. Environ. Sci. 2019, 32, 11–21. [Google Scholar] [PubMed]
- Umre, R.; Ganeshpurkar, A.; Ganeshpurkar, A.; Pandey, S.; Pandey, V.; Shrivastava, A.; Dubey, N. In vitro, in vivo and in silico antiulcer activity of ferulic acid. Future J. Pharm. Sci. 2018, 4, 248–253. [Google Scholar] [CrossRef]
- Jia, W.; Liu, G.; Zhang, C.; Zhang, S. Formononetin attenuates hydrogen peroxide (H2O2)-induced apoptosis and NF-κB activation in RGC-5 cells. Eur. Rev. Med. Pharm. Sci. 2014, 18, 2191–2197. [Google Scholar]
- Li, Z.; Dong, X.; Zhang, J.; Zeng, G.; Zhao, H.; Liu, Y.; Qiu, R.; Mo, L.; Ye, Y. Formononetin protects TBI rats against neurological lesions and the underlying mechanism. J. Neurol. Sci. 2014, 338, 112–117. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, Y.; Gao, L.; Yin, H.; Xie, Z.; Wang, D.; Zhu, Z.; Han, X. Formononetin attenuates IL-1β-induced apoptosis and NF-κB activation in INS-1 cells. Molecules 2012, 17, 10052–10064. [Google Scholar] [CrossRef] [Green Version]
- Draganova-Filipova, M.N.; Georgieva, M.G.; Peycheva, E.N.; Miloshev, G.A.; Sarafian, V.S.; Peychev, L.P. Effects of propolis and CAPE on proliferation and apoptosis of McCoy-Plovdiv cell line. Folia Med. 2008, 50, 53–59. [Google Scholar]
- Gong, J.; Zhang, X.; Tan, Y.; Li, H.; Hou, J.; Zhang, J. Gastroprotective effect of the root extract of Alpinia officinarum Hance (Zingiberoside) against acute indomethacin-induced gastric injuries in rats: Involvement of H+/K+-ATPase and prostaglandin E receptors. Trop. J. Pharm. Res. 2020, 19, 1887–1893. [Google Scholar] [CrossRef]
- Zhou, D.; Yang, Q.; Tian, T.; Chang, Y.; Li, Y.; Duan, L.-R.; Li, H.; Wang, S.-W. Gastroprotective effect of gallic acid against ethanol-induced gastric ulcer in rats: Involvement of the Nrf2/HO-1 signaling and anti-apoptosis role. Biomed. Pharmacother. 2020, 126, 110075. [Google Scholar] [CrossRef]
- Gao, Y.; Liu, F.; Fang, L.; Cai, R.; Zong, C.; Qi, Y. Genkwanin inhibits proinflammatory mediators mainly through the regulation of miR-101/MKP-1/MAPK pathway in LPS-activated macrophages. PLoS ONE 2014, 9, e96741. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Lange, S.; Oshalim, M.; Lönnroth, I. Anti-Inflammatory Substances in Wheat Malt Inducing Antisecretory Factor. Plant Foods Hum. Nutr. 2019, 74, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Anouar, E.; Calliste, C.; Kosinova, P.; Di Meo, F.; Duroux, J.; Champavier, Y.; Marakchi, K.; Trouillas, P. Free radical scavenging properties of guaiacol oligomers: A combined experimental and quantum study of the guaiacyl-moiety role. J. Phys. Chem. A 2009, 113, 13881–13891. [Google Scholar] [CrossRef]
- Moon, S.H.; Lee, J.H.; Kim, K.-T.; Park, Y.-S.; Nah, S.-Y.; Ahn, D.U.; Paik, H.-D. Antimicrobial effect of 7-O-butylnaringenin, a novel flavonoid, and various natural flavonoids against Helicobacter pylori strains. Int. J. Environ. Res. Public Health 2013, 10, 5459–5469. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-L.; Chen, S.-C.; Senthil Kumar, K.; Yu, K.-N.; Lee Chao, P.-D.; Tsai, S.-Y.; Hou, Y.-C.; Hseu, Y.-C. Antioxidant and anti-inflammatory potential of hesperetin metabolites obtained from hesperetin-administered rat serum: An ex vivo approach. J. Agric. Food Chem. 2012, 60, 522–532. [Google Scholar] [CrossRef]
- Bigoniya, P.; Singh, K. Ulcer protective potential of standardized hesperidin, a citrus flavonoid isolated from Citrus sinensis. Rev. Bras. Farmacogn. 2014, 24, 330–340. [Google Scholar] [CrossRef] [Green Version]
- Hao, B.-J.; Wu, Y.-H.; Wang, J.-G.; Hu, S.-Q.; Keil, D.J.; Hu, H.-J.; Lou, J.-D.; Zhao, Y. Hepatoprotective and antiviral properties of isochlorogenic acid A from Laggera alata against hepatitis B virus infection. J. Ethnopharmacol. 2012, 144, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Gong, G.; Guan, Y.-Y.; Zhang, Z.-L.; Rahman, K.; Wang, S.-J.; Zhou, S.; Luan, X.; Zhang, H. Isorhamnetin: A review of pharmacological effects. Biomed. Pharmacother. 2020, 128, 110301. [Google Scholar] [CrossRef]
- Kang, G.-D.; Kim, D.-H. Ponciretin attenuates ethanol-induced gastric damage in mice by inhibiting inflammatory responses. Int. Immunopharmacol. 2017, 43, 179–186. [Google Scholar] [CrossRef]
- Gaur, R.; Kumar, S.; Trivedi, P.; Bhakuni, R.S.; Bawankule, D.U.; Pal, A.; Shanker, K. Liquiritigenin derivatives and their hepatotoprotective activity. Nat. Prod. Commun. 2010, 5, 1934578X1000500819. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Zhao, R.; Park, S.; Lee, J.; Cho, I.; Yang, C.; Kim, S.; Kim, S. Anti-inflammatory effects of liquiritigenin as a consequence of the inhibition of NF-κB-dependent iNOS and proinflammatory cytokines production. Br. J. Pharmacol. 2008, 154, 165–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alrushaid, S.; Davies, N.M.; Martinez, S.E.; Sayre, C.L. Pharmacological characterization of liquiritigenin, a chiral flavonoid in licorice. Res. Pharm. Sci. 2016, 11, 355. [Google Scholar]
- Park, C.; Song, Y. Comparative analysis of anti-inflammatory activity of luteolin and luteolin-7-O-glucoside against galactosamine/lipopolysaccharide induced hepatotoxicity in mice. Proc. Nutr. Soc. 2018, 77, E175. [Google Scholar] [CrossRef] [Green Version]
- Ren, L.-Q.; Li, Q.; Zhang, Y. Luteolin suppresses the proliferation of gastric cancer cells and acts in synergy with oxaliplatin. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansoori, M.N.; Raghuvanshi, A.; Shukla, P.; Awasthi, P.; Trivedi, R.; Goel, A.; Singh, D. Medicarpin prevents arthritis in post-menopausal conditions by arresting the expansion of TH17 cells and pro-inflammatory cytokines. Int. Immunopharmacol. 2020, 82, 106299. [Google Scholar] [CrossRef] [PubMed]
- Righi, A.A.; Alves, T.R.; Negri, G.; Marques, L.M.; Breyer, H.; Salatino, A. Brazilian red propolis: Unreported substances, antioxidant and antimicrobial activities. J. Sci. Food Agric. 2011, 91, 2363–2370. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Mendoza, M.E.; Cruz-Antonio, L.; Arrieta-Baez, D.; Olivares-Corichi, I.M.; Rojas-Martínez, R.; Martínez-Cabrera, D.; Arrieta, J. Gastroprotective activity of methyleugenol from Peperomia hispidula on ethanol-induced gastric lesions in rats. Int. J. Pharmacol. 2015, 11, 697–704. [Google Scholar] [CrossRef]
- Leem, H.-H.; Kim, E.-O.; Seo, M.-J.; Choi, S.-W. Antioxidant and anti-inflammatory activities of eugenol and its derivatives from clove (Eugenia caryophyllata Thunb). J. Korean Soc. Food Sci. Nutr. 2011, 40, 1361–1370. [Google Scholar] [CrossRef]
- Hayder, N.; Bouhlel, I.; Skandrani, I.; Kadri, M.; Steiman, R.; Guiraud, P.; Mariotte, A.-M.; Ghedira, K.; Dijoux-Franca, M.-G.; Chekir-Ghedira, L. In vitro antioxidant and antigenotoxic potentials of myricetin-3-o-galactoside and myricetin-3-o-rhamnoside from Myrtus communis: Modulation of expression of genes involved in cell defence system using cDNA microarray. Toxicol. Vitr. 2008, 22, 567–581. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Azevedo, A.; Campos, J.J.; de Souza, G.G.; de Carvalho Veloso, C.; Duarte, I.D.G.; Braga, F.C.; de Castro Perez, A. Antinociceptive and anti-inflammatory effects of myricetin 3-O-β-galactoside isolated from Davilla elliptica: Involvement of the nitrergic system. J. Nat. Med. 2015, 69, 487–493. [Google Scholar] [CrossRef]
- Maatouk, M.; Elgueder, D.; Mustapha, N.; Chaaban, H.; Bzéouich, I.M.; Loannou, I.; Kilani, S.; Ghoul, M.; Ghedira, K.; Chekir-Ghedira, L. Effect of heated naringenin on immunomodulatory properties and cellular antioxidant activity. Cell Stress Chaperones 2016, 21, 1101–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, R.; Andrades, N.E.; Paulino, N.; Sawaya, A.C.; Eberlin, M.N.; Marcucci, M.C.; Favero, G.M.; Novak, E.M.; Bydlowski, S.P. Synthesis and characterization of a metal complex containing naringin and Cu, and its antioxidant, antimicrobial, antiinflammatory and tumor cell cytotoxicity. Molecules 2007, 12, 1352–1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, L.; Zhang, Z.-H.; Sun, E.; Jia, X.-B. Effect of β-cyclodextrin complexation on solubility and enzymatic conversion of naringin. Int. J. Mol. Sci. 2012, 13, 14251–14261. [Google Scholar] [CrossRef] [Green Version]
- Bueno-Silva, B.; Alencar, S.M.; Koo, H.; Ikegaki, M.; Silva, G.V.; Napimoga, M.H.; Rosalen, P.L. Anti-inflammatory and antimicrobial evaluation of neovestitol and vestitol isolated from Brazilian red propolis. J. Agric. Food Chem. 2013, 61, 4546–4550. [Google Scholar] [CrossRef]
- Bueno-Silva, B.; Rosalen, P.L.; Alencar, S.M.; Mayer, M.P. Anti-inflammatory mechanisms of neovestitol from Brazilian red propolis in LPS-activated macrophages. J. Funct. Foods 2017, 36, 440–447. [Google Scholar] [CrossRef]
- Zhu, H.; Liang, Q.-h.; Xiong, X.-g.; Wang, Y.; Zhang, Z.-h.; Sun, M.-j.; Lu, X.; Wu, D. Anti-inflammatory effects of p-coumaric acid, a natural compound of Oldenlandia diffusa, on arthritis model rats. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Godarzi, S.M.; Gorji, A.V.; Gholizadeh, B.; Mard, S.A.; Mansouri, E. Antioxidant effect of p-coumaric acid on interleukin 1-β and tumor necrosis factor-α in rats with renal ischemic reperfusion. Nefrologia 2020, 40, 311–319. [Google Scholar] [CrossRef]
- Zheng, Y.-Z.; Deng, G.; Chen, D.-F.; Liang, Q.; Guo, R.; Fu, Z.-M. Theoretical studies on the antioxidant activity of pinobanksin and its ester derivatives: Effects of the chain length and solvent. Food Chem. 2018, 240, 323–329. [Google Scholar] [CrossRef] [PubMed]
- El-Demerdash, A.A.; Menze, E.T.; Esmat, A.; Tadros, M.G.; Elsherbiny, D.A. Protective and therapeutic effects of the flavonoid “pinocembrin” in indomethacin-induced acute gastric ulcer in rats: Impact of anti-oxidant, anti-inflammatory, and anti-apoptotic mechanisms. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2021, 394, 1411–1424. [Google Scholar] [CrossRef] [PubMed]
- Abdelwahab, S.I.; Mohan, S.; Abdulla, M.A.; Sukari, M.A.; Abdul, A.B.; Taha, M.M.E.; Syam, S.; Ahmad, S.; Lee, K.-H. The methanolic extract of Boesenbergia rotunda (L.) Mansf. and its major compound pinostrobin induces anti-ulcerogenic property in vivo: Possible involvement of indirect antioxidant action. J. Ethnopharmacol. 2011, 137, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Jung, H.S.; Yoon, C.S.; Ko, J.H.; Chun, H.J.; Kim, T.K.; Kwon, M.J.; Lee, S.H.; Koh, K.S.; Rhee, B.D. EGCG and quercetin protected INS-1 cells in oxidative stress via different mechanisms. Front. Biosci. 2010, 2, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Coskun, O.; Kanter, M.; Korkmaz, A.; Oter, S. Quercetin, a flavonoid antioxidant, prevents and protects streptozotocin-induced oxidative stress and β-cell damage in rat pancreas. Pharmacol. Res. 2005, 51, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.-T.; Ding, C.; Zhou, N.; Xu, C. Quercetin protects gastric epithelial cell from oxidative damage in vitro and in vivo. Eur. J. Pharmacol. 2015, 754, 115–124. [Google Scholar] [CrossRef]
- Jnawali, H.N.; Lee, E.; Jeong, K.-W.; Shin, A.; Heo, Y.-S.; Kim, Y. Anti-inflammatory activity of rhamnetin and a model of its binding to c-Jun NH2-terminal kinase 1 and p38 MAPK. J. Nat. Prod. 2014, 77, 258–263. [Google Scholar] [CrossRef]
- Abdel-Raheem, I.T. Gastroprotective effect of rutin against indomethacin-induced ulcers in rats. Basic Clin. Pharmacol. Toxicol. 2010, 107, 742–750. [Google Scholar] [CrossRef]
- Dubey, S.; Ganeshpurkar, A.; Shrivastava, A.; Bansal, D.; Dubey, N. Rutin exerts antiulcer effect by inhibiting the gastric proton pump. Indian J. Pharmacol. 2013, 45, 415. [Google Scholar]
- Srinivasulu, C.; Ramgopal, M.; Ramanjaneyulu, G.; Anuradha, C.; Kumar, C.S. Syringic acid (SA)‒a review of its occurrence, biosynthesis, pharmacological and industrial importance. Biomed. Pharmacother. 2018, 108, 547–557. [Google Scholar] [CrossRef]
- Trombino, S.; Cassano, R.; Ferrarelli, T.; Barone, E.; Picci, N.; Mancuso, C. Trans-ferulic acid-based solid lipid nanoparticles and their antioxidant effect in rat brain microsomes. Colloids Surf. B Biointerfaces 2013, 109, 273–279. [Google Scholar] [CrossRef]
- Sgarbossa, A.; Giacomazza, D.; Di Carlo, M. Ferulic acid: A hope for Alzheimer’s disease therapy from plants. Nutrients 2015, 7, 5764–5782. [Google Scholar] [CrossRef]
- Shalini, V.; Jayalekshmi, A.; Helen, A. Mechanism of anti-inflammatory effect of tricin, a flavonoid isolated from Njavara rice bran in LPS induced hPBMCs and carrageenan induced rats. Mol. Immunol. 2015, 66, 229–239. [Google Scholar] [CrossRef]
- Duarte-Almeida, J.M.; Negri, G.; Salatino, A.; de Carvalho, J.E.; Lajolo, F.M. Antiproliferative and antioxidant activities of a tricin acylated glycoside from sugarcane (Saccharum officinarum) juice. Phytochemistry 2007, 68, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Dung, H.V.; Cuong, T.D.; Chinh, N.M.; Quyen, D.; Kim, J.A.; Byeon, J.S.; Woo, M.H.; Choi, J.S.; Min, B.S. Compounds from the aerial parts of Piper bavinum and their anti-cholinesterase activity. Arch. Pharm. Res. 2015, 38, 677–682. [Google Scholar] [CrossRef]
- Seo, P.J.; Kim, N.; Kim, J.-H.; Lee, B.H.; Nam, R.H.; Lee, H.S.; Park, J.H.; Lee, M.K.; Chang, H.; Jung, H.C. Comparison of indomethacin, diclofenac and aspirin-induced gastric damage according to age in rats. Gut Liver 2012, 6, 210. [Google Scholar] [CrossRef] [PubMed]
- Katary, M.; Salahuddin, A. Gastroprotective effect of vanillin on indomethacininduced gastric ulcer in rats: Protective pathways and anti-secretory mechanism. Clin. Exp. Pharmacol. 2017, 7, 232. [Google Scholar]
- Hiratsuka, T.; Futagami, S.; Shindo, T.; Hamamoto, T.; Ueki, N.; Suzuki, K.; Shinji, Y.; Kusunoki, M.; Shinoki, K.; Wada, K. Rebamipide reduces indomethacin-induced gastric injury in mice via down-regulation of ICAM-1 expression. Dig. Dis. Sci. 2005, 50, S84–S89. [Google Scholar] [CrossRef]
- Zhang, X.; Tajima, K.; Kageyama, K.; Kyoi, T. Irsogladine maleate suppresses indomethacin-induced elevation of proinflammatory cytokines and gastric injury in rats. World J. Gastroenterol. WJG 2008, 14, 4784. [Google Scholar] [CrossRef]
- Al-Wajeeh, N.S.; Hajerezaie, M.; Noor, S.M.; Halabi, M.F.; Al-Henhena, N.; Azizan, A.H.S.; Kamran, S.; Hassandarvish, P.; Shwter, A.N.; Ali, H.M. The gastro protective effects of Cibotium barometz hair on ethanol-induced gastric ulcer in Sprague-Dawley rats. BMC Vet. Res. 2016, 13, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Ashmawy, N.E.; Khedr, E.G.; El-Bahrawy, H.A.; Selim, H.M. Gastroprotective effect of garlic in indomethacin induced gastric ulcer in rats. Nutrition 2016, 32, 849–854. [Google Scholar] [CrossRef]
- Franchin, M.; da Cunha, M.G.; Denny, C.; Napimoga, M.H.; Cunha, T.M.; Bueno-Silva, B.; Matias de Alencar, S.; Ikegaki, M.; Luiz Rosalen, P. Bioactive fraction of geopropolis from Melipona scutellaris decreases neutrophils migration in the inflammatory process: Involvement of nitric oxide pathway. Evid.-Based Complement. Altern. Med. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.C.; Chu, K.H.; Liang, Y.C.; Lin, Y.L.; Chiang, B.L. Caffeic acid phenethyl ester inhibits nuclear factor-κB and protein kinase B signalling pathways and induces caspase-3 expression in primary human CD4+ T cells. Clin. Exp. Immunol. 2010, 160, 223–232. [Google Scholar] [CrossRef]
- Lima, V.H.M.d.; Almeida, K.d.C.R.; Alves, C.C.F.; Rodrigues, M.L.; Crotti, A.E.M.; Souza, J.M.d.; Ribeiro, A.B.; Squarisi, I.S.; Tavares, D.C.; Martins, C.H.G. Biological properties of volatile oil from Brazilian brown propolis. Rev. Bras. Farmacogn. 2019, 29, 807–810. [Google Scholar] [CrossRef]
- Alaribe, C.S.; Esposito, T.; Sansone, F.; Sunday, A.; Pagano, I.; Piccinelli, A.L.; Celano, R.; Cuesta Rubio, O.; Coker, H.A.; Nabavi, S.M. Nigerian propolis: Chemical composition, antioxidant activity and α-amylase and α-glucosidase inhibition. Nat. Prod. Res. 2019, 11, 1–5. [Google Scholar] [CrossRef]
- Chatterjee, A.; Khatua, S.; Chatterjee, S.; Mukherjee, S.; Mukherjee, A.; Paloi, S.; Acharya, K.; Bandyopadhyay, S.K. Polysaccharide-rich fraction of Termitomyces eurhizus accelerate healing of indomethacin induced gastric ulcer in mice. Glycoconj. J. 2013, 30, 759–768. [Google Scholar] [CrossRef]
- Min, Y.S.; Lee, S.E.; Hong, S.T.; Kim, H.S.; Choi, B.-C.; Sim, S.S.; Whang, W.K.; Sohn, U.D. The inhibitory effect of quercetin-3-o-β-d-glucuronopyranoside on gastritis and reflux esophagitis in rats. Korean J. Physiol. Pharmacol. Off. J. Korean Physiol. Soc. Korean Soc. Pharmacol. 2009, 13, 295. [Google Scholar] [CrossRef] [Green Version]
- Beil, W.; Birkholz, C.; Sewing, K.-F. Effects of flavonoids on parietal cell acid secretion, gastric mucosal prostaglandin production and Helicobacter pylori growth. Arzneimittel-Forschung 1995, 45, 697–700. [Google Scholar]
- Coelho, L.; Bastos, E.; Resende, C.C.; e Silva, P.; Sanches, B.; De Castro, F.J.; Moretzsohn, L.D.; Vieira, W.; Trindade, O.R. Brazilian green propolis on Helicobacter pylori infection. a pilot clinical study. Helicobacter 2007, 12, 572–574. [Google Scholar] [CrossRef]
- Jasprica, I.; Mornar, A.; Debeljak, Ž.; Smolčić-Bubalo, A.; Medić-Šarić, M.; Mayer, L.; Romić, Ž.; Bućan, K.; Balog, T.; Sobočanec, S. In vivo study of propolis supplementation effects on antioxidative status and red blood cells. J. Ethnopharmacol. 2007, 110, 548–554. [Google Scholar] [CrossRef]
- Diniz, D.P.; Lorencini, D.A.; Berretta, A.A.; Cintra, M.A.; Lia, E.N.; Jordão, A.A.; Coelho, E.B. Antioxidant effect of standardized extract of propolis (EPP-AF®) in healthy volunteers: A “before and after” clinical study. Evid.-Based Complement. Altern. Med. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Henshaw, F.R.; Bolton, T.; Nube, V.; Hood, A.; Veldhoen, D.; Pfrunder, L.; McKew, G.L.; Macleod, C.; McLennan, S.V.; Twigg, S.M. Topical application of the bee hive protectant propolis is well tolerated and improves human diabetic foot ulcer healing in a prospective feasibility study. J. Diabetes Its Complicat. 2014, 28, 850–857. [Google Scholar] [CrossRef] [Green Version]
- Samet, N.; Laurent, C.; Susarla, S.M.; Samet-Rubinsteen, N. The effect of bee propolis on recurrent aphthous stomatitis: A pilot study. Clin. Oral Investig. 2007, 11, 143–147. [Google Scholar] [CrossRef]
- Hamdy, A.; Ibrahem, M. Management of aphthous ulceration with topical quercetin: A randomized clinical trial. J. Contemp. Dent. Pract. 2010, 11, E009–E016. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Work | Model-Induced Ulcer and Dose | Animal Model and Characteristics | Experimental Groups and Route of Administration | Methodology | Results |
|---|---|---|---|---|---|
| de Barros, M.P. et al., 2007 [57] | Ethanol 99.5% (1 mL) Indomethacin (100 mg/kg) Stress (immersed in water at 25 °C for 17 h) | Male Wistar rats, weighing 200–250 g with 12 h of fasting | Five groups (n = 6):
| Ethanol-induced gastric ulcer: After 12 h of fasting, the experimental groups were treated orally according to their group. One hour after, all groups received 1 mL of 99.5% of ethanol to induce gastric ulcers. After 1 h, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. NSAID-induced gastric ulcer: After 12 h of fasting, the experimental groups were treated orally according to their group. One hour after, all groups received indomethacin (100 mg/kg p.o.) to induce gastric ulcers. After 4 h, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. Stress-induced gastric ulcer: Experimental groups were treated orally according to their group. After 30 min, animals were placed in tubes and immersed vertically until the water reached the neck region in a tank with water at 25 °C for 17 h. After this period, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. | In the ethanol-induced gastric ulcer, the three doses of green propolis and omeprazole reduced the lesion index, the total lesion area, and the percentage of the lesion in comparison with the vehicle group. In contrast, only the dose of 500 mg/kg of green propolis and the cimetidine group reduced gastric ulceration in the NSAID-induced gastric ulcer model. Whereas, in the stress-induced gastric ulcer, both the 200 mg/kg and 500 mg/kg green propolis doses reduced gastric ulceration. |
| El-Ghazaly, M.A. et al., 2011 [58] | Radiation exposure 6 Gy (0.48 Gy/min) and indomethacin (10 mg/kg) | Male Wistar rats, weighing 150–200 g with 48 h of fasting | Four groups (n = 8):
| Assessment of the effect of propolis against gastric ulcers in normal animals: After 48 h of fasting, animals were administered with propolis or lansoprazole. After 1 h, animals were submitted to pyloric ligation surgery. After that, all experimental groups were given indomethacin (10 mg/kg i.p) with the exception of the vehicle group. After 4 h, the animals were anesthetized with ether and sacrificed by decapitation, trunk blood was collected, and the stomachs were removed and opened along the greater curvature. Assessment of the effect of irradiation and treatment with propolis on gastric ulceration: Different groups of rats were randomly allocated to receive a single radiation dose with a level of 6 Gy 24 h before indomethacin injection. After radiation dose, animals were administered with propolis or lansoprazole. After 1 h, animals were submitted to pyloric ligation surgery. At the end of the surgery, all experimental groups were given indomethacin (10 mg/kg i.p) with exception of vehicle group. After 4 h, the animals were anesthetized with ether and sacrificed by decapitation, trunk blood was collected, and the stomachs were removed and opened along the greater curvature. | Effect of propolis against gastric ulcer in normal animals: The treatment with propolis and lansoprazole reduced gastric ulceration by 75% and 87%, respectively. Both treatments reduced the free acidity and acid output and increased the gastric mucin content compared to the indomethacin group. Moreover, propolis and omeprazole protected against the reduction in PGE2 content and protected against the increase in inflammatory TNF-α and IL-1β mediators. Finally, both treatments reduced the lipid peroxidation to the normal values. Effect of irradiation and treatment with propolis on gastric ulceration: Exposure of animals to radiation before indomethacin injection increased gastric acidity and acid output significantly. Nevertheless, propolis and lansoprazole treatment had similar action on the parameters measured in the previous experiment. |
| de Mendonça, M.A. et al., 2020 [59] | Ethanol 99.5% (1 mL) Indomethacin (100 mg/kg) | Male and female Wistar rats, weighing 280–320 g with 24 h of fasting | Six groups (n = 6):
| Ethanol-induced gastric ulcer: After 24 h of fasting, the experimental groups were treated orally according to their group. One hour after, all groups received 1 mL of 99.5% of ethanol to induce gastric ulcers. After 30 min, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. NSAID-induced gastric ulcer: After 24 h of fasting, the experimental groups were treated orally according to their group. After 30 min, all groups received indomethacin (100 mg/kg p.o.) to induce gastric ulcers. After 6 h, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. | Pre-treatments with the doses of red propolis inhibited the total lesion areas in a dose-dependent way; formononetin and omeprazole also reduced the area of total lesion significantly in the ethanol-induced gastric ulcer model. Moreover, histopathological damages induced by indomethacin in the gastric tissue were reduced with the treatments with red propolis. In the NSAID-induced gastric model, pre-treatments with the three doses of red propolis, formononetin, and cimetidine reduced the ulcer index with respect to the vehicle group; moreover, the 50 and 250 mg/kg doses of red propolis and formononetin reduced the secretion volume of gastric content; however, both treatments did not reduce the pH of gastric content. In contrast, the dose of 500 mg/kg of red propolis and formononetin increased mucus production in the stomach compared to the vehicle group. |
| Ruiz-Hurtado, P.A. et al., 2021 [60] | Indomethacin (20 mg/kg) | ICR mice weighing 25 ± 5 g with 12 h of fasting | Six groups (n = 6):
| NSAID-induced gastric ulcer: After 12 h of fasting, the experimental groups were treated orally according to their group. After 2 h, all groups received indomethacin (100 mg/kg p.o.) to induce gastric ulcers. After 6 h, animals were sacrificed by cervical dislocation, and the stomachs were removed and opened along the greater curvature. | The vehicle group did not develop gastric mucosal lesions, in contrast to the indomethacin group. Different doses of Chihuahua propolis and the treatment with omeprazole significantly decreased gastric injuries both macroscopically and histologically. Additionally, these treatments increased the mucus content in the gastric tissue and reduced lipid peroxidation. In line with this, the 150 mg/kg dose of Chihuahua propolis increased the SOD activity, and the 300 mg/kg dose increased GPx activity. On the other hand, the 150 and 300 mg/kg doses of Chihuahua propolis increased the PGE2 content, and both doses reduced the concentration of pro-inflammatory markers (TNF-α, IL-1β, and IL-6) as well as MPO content. |
| Compound | Activity Related to Gastroprotective Effect | Country of Origin of Propolis Sample | Activity References | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Ga | Au | As | Af | Im | Ax | Cp | |||
| 2,2-dimethyl-6-carboxyethenyl-2H-1-benzopirane | Brazil [67] | ||||||||
| 3-prenyl-4-dihydroxycinnamoiloxy cinnamic acid (baccharin) | Brazil [67,68] | ||||||||
| 3-prenyl-4-hidroxycinamic acid (drupanin) | X | X | X | X | X | Brazil [57,68] | [68,69] | ||
| 3,4-dimethoxycinnamic acid | X | Mexico [70] | [70] | ||||||
| 3,5-diprenyl-4-hidroxycinamic acid (artepillin C) | X | X | X | X | X | X | Brazil [57,67,68,71,72,73] | [68,74,75] | |
| 3.3-dimethylallyl caffeate | X | Mexico [70] | [70] | ||||||
| 5-methylchrysin ether | X | Mexico [76] | [76] | ||||||
| 5-methylgalangin ether | X | Mexico [76,77] | [76] | ||||||
| 5-methylpinobanksin ether | X | Mexico [76,77] | [76] | ||||||
| 7-O-methylvestitol | X | X | X | X | Brazil [63] | [63] | |||
| Acacetin | X | X | X | X | Mexico, Brazil [78,79,80] | [81,82] | |||
| Alnusin | Brazil [83] | ||||||||
| Alpinetin | X | X | X | Mexico [76,77] | [76,84] | ||||
| Alpinone | X | Mexico [77] | [85] | ||||||
| Anethole | X | X | X | Brazil [83] | [86,87] | ||||
| Anisaldehyde | Brazil [83] | ||||||||
| Apigenin | X | X | X | X | X | Mexico [60,79] | [88,89] | ||
| Aromadendrine-4′-O-metyl ether | X | X | Brazil [57,68] | [68] | |||||
| Baicalein | X | X | X | X | X | X | X | Mexico [60] | [55] |
| Benzoic acid | X | X | Brazil [71,83] | [90] | |||||
| Biochanin A | X | X | X | X | X | X | X | Brazil [83,91] | [92,93,94,95,96] |
| Cadinene | X | Brazil [83] | [97] | ||||||
| Caffeic acid | X | X | X | X | X | X | X | Brazil, Mexico [57,70,72,73,76,98,99] | [76,98,100,101,102,103] |
| Caffeic acid phenethyl ester (CAPE) | X | X | X | X | X | X | X | Denmark, Mexico, Brazil [58,73,79,104] | [105,106,107,108,109] |
| Calycosin | X | X | Brazil [80] | [110] | |||||
| Catechin | X | X | X | Mexico, Brazil [60,99,111] | [88,112,113] | ||||
| Catechol | X | X | X | X | Mexico [60] | [114,115] | |||
| Cholorgenic acid | X | X | X | X | X | X | Brazil [73] | [116] | |
| Chrysin | X | X | X | X | Mexico, Brazil [60,76,77,78,79,80,104,117] | [56,76] | |||
| Cinnamic acid | X | X | X | X | X | X | X | Brazil, Mexico [70,71,79,98] | [98,118,119] |
| Daidzein | X | X | Brazil [91] | [120,121] | |||||
| Dalbergin | Brazil [80] | ||||||||
| Dihydrocinnamic acid | Brazil [71] | ||||||||
| Dihydroxy-methoxy chalcone | Brazil [122] | ||||||||
| Dihydroxy-methoxy flavanone | Brazil [122] | ||||||||
| Dihydroxy-trimethoxyflavone | Brazil [122] | ||||||||
| Dillenetin | X | Mexico [76] | [76] | ||||||
| Dimethoxy-dihydrochalcone | Brazil [122] | ||||||||
| Elemicin | Brazil [83] | ||||||||
| Epicatechin | X | Brazil [99] | [123] | ||||||
| Epoxypinocembrin chalcone | X | Mexico [70] | [70] | ||||||
| Ferulic acid | X | X | X | X | X | X | X | Brazil, Mexico [76,79,98,111] | [76,98,103,124,125] |
| Formononetin | X | X | X | X | X | Brazil [59,83,91,99] | [59,95,126,127,128] | ||
| Galangin | X | X | X | X | Mexico [76,79,117] | [76,129,130] | |||
| Gallic acid | X | X | X | X | X | Mexico, Brazil [72,79,99] | [131] | ||
| Genkwanin | X | X | Brazil [80] | [132] | |||||
| Guaiacol | X | X | Brazil [83] | [133,134] | |||||
| Hesperetin | X | X | X | X | X | Mexico [104] | [135,136,137] | ||
| Hispidulin | X | X | Brazil [80] | [110] | |||||
| Isocholorgenic acid A | X | X | X | X | Brazil [73] | [138] | |||
| Isocholorgenic acid B | Brazil [73] | ||||||||
| Isocholorgenic acid C | Brazil [73] | ||||||||
| Isoelemicin | Brazil [83] | ||||||||
| Isopent-3-enyl caffeate | X | Mexico [70] | [70] | ||||||
| Isorhamnetin | X | X | X | Mexico [76,77] | [76,139] | ||||
| Isorhamnetin-3-O-glucosylgallate | Brazil [122] | ||||||||
| Isosakuranetin (ponciretin) | X | Brazil [57] | [140] | ||||||
| Izalpinin | X | Mexico [70] | [70] | ||||||
| Kaempferide | X | X | X | Brazil, Mexico [68,77] | [68] | ||||
| Kaempferol | X | X | X | X | Mexico, Brazil [60,70,78,79,99,122] | [53,54,70,88,120] | |||
| Liquiritigenin | X | X | X | X | Brazil [83] | [141,142,143] | |||
| Luteolin | X | X | X | X | X | Mexico, Brazil [78,79,111] | [89,112,135,144,145] | ||
| Medicarpin | X | X | X | X | Brazil [63,80,83] | [63,146] | |||
| Methoxy-dihydrochalcone | Brazil [122] | ||||||||
| Methoxyeugenol | X | Brazil [83] | [147] | ||||||
| Methyl eugenol | X | X | X | X | Brazil [83] | [148,149] | |||
| Myricetin-3-O-rhamnoside | X | X | Brazil [122] | [150,151] | |||||
| Naringenin | X | X | X | X | X | Mexico [60,78,79,104] | [88,120,152] | ||
| Naringin | X | X | X | X | Mexico [60,78] | [88,153,154] | |||
| Neovestitol | X | X | Brazil [63,155] | [155,156] | |||||
| Oblongifolin B | Brazil [63,80] | ||||||||
| p-coumaric acid | X | X | X | X | X | Brazil, Mexico [57,71,72,79,98,99] | [98,103,157,158] | ||
| Pentahydroxy-flavone-malonyl gallate | Brazil [122] | ||||||||
| Pinobanksin | X | Mexico, Brazil [77,80] | [159] | ||||||
| Pinobanksin-3-O-acetate | Mexico [79,117] | ||||||||
| Pinocembrin | X | X | X | X | X | X | X | Mexico, Brazil [60,70,72,76,77,78,79,91,104,117] | [70,76,77,85,129,160] |
| Pinostrobin | X | Mexico [70,77,79] | [161] | ||||||
| Prenyl-p-coumaric | X | X | Brazil [71] | [68] | |||||
| Prenyl-pentahydroxy-flavone | Brazil [122] | ||||||||
| Quercetin | X | X | X | X | X | X | X | Mexico, Brazil [78,79,99,122] | [89,120,162,163,164] |
| Retusapurpurin | Brazil [83] | ||||||||
| Rhamnetin | X | X | Mexico [70] | [165] | |||||
| Rutin | X | X | X | X | X | X | Mexico, Brazil [99,104] | [166,167] | |
| Syringic acid | X | X | X | Mexico [76] | [76,168] | ||||
| Tetrahydroxy flavonon | Brazil [71] | ||||||||
| Trans-ferulic acid | X | X | Brazil [99] | [169,170] | |||||
| Tricin | X | X | Brazil [80] | [171,172] | |||||
| Trihydroxy-dihydrocinnamic acid | Brazil [122] | ||||||||
| Trihydroxy-dimethoxy chalcone | Brazil [122] | ||||||||
| Tryhidroxymethoxy flavonon | Brazil [71] | ||||||||
| Vestitol | X | X | X | Mexico, Brazil [63,80,83] | [95,155] | ||||
| Vestitone | Brazil [80] | ||||||||
| Violanthin | X | Brazil [122] | [173] | ||||||
| Xanthochymol | Brazil [83] | ||||||||
| ε-caprolactone derivative | Mexico [70] | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Hurtado, P.A.; Garduño-Siciliano, L.; Domínguez-Verano, P.; Balderas-Cordero, D.; Gorgua-Jiménez, G.; Canales-Álvarez, O.; Canales-Martínez, M.M.; Rodríguez-Monroy, M.A. Propolis and Its Gastroprotective Effects on NSAID-Induced Gastric Ulcer Disease: A Systematic Review. Nutrients 2021, 13, 3169. https://doi.org/10.3390/nu13093169
Ruiz-Hurtado PA, Garduño-Siciliano L, Domínguez-Verano P, Balderas-Cordero D, Gorgua-Jiménez G, Canales-Álvarez O, Canales-Martínez MM, Rodríguez-Monroy MA. Propolis and Its Gastroprotective Effects on NSAID-Induced Gastric Ulcer Disease: A Systematic Review. Nutrients. 2021; 13(9):3169. https://doi.org/10.3390/nu13093169
Chicago/Turabian StyleRuiz-Hurtado, Porfirio Alonso, Leticia Garduño-Siciliano, Pilar Domínguez-Verano, Daniela Balderas-Cordero, Gustavo Gorgua-Jiménez, Octavio Canales-Álvarez, María Margarita Canales-Martínez, and Marco Aurelio Rodríguez-Monroy. 2021. "Propolis and Its Gastroprotective Effects on NSAID-Induced Gastric Ulcer Disease: A Systematic Review" Nutrients 13, no. 9: 3169. https://doi.org/10.3390/nu13093169
APA StyleRuiz-Hurtado, P. A., Garduño-Siciliano, L., Domínguez-Verano, P., Balderas-Cordero, D., Gorgua-Jiménez, G., Canales-Álvarez, O., Canales-Martínez, M. M., & Rodríguez-Monroy, M. A. (2021). Propolis and Its Gastroprotective Effects on NSAID-Induced Gastric Ulcer Disease: A Systematic Review. Nutrients, 13(9), 3169. https://doi.org/10.3390/nu13093169