
Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Subjects and Methods
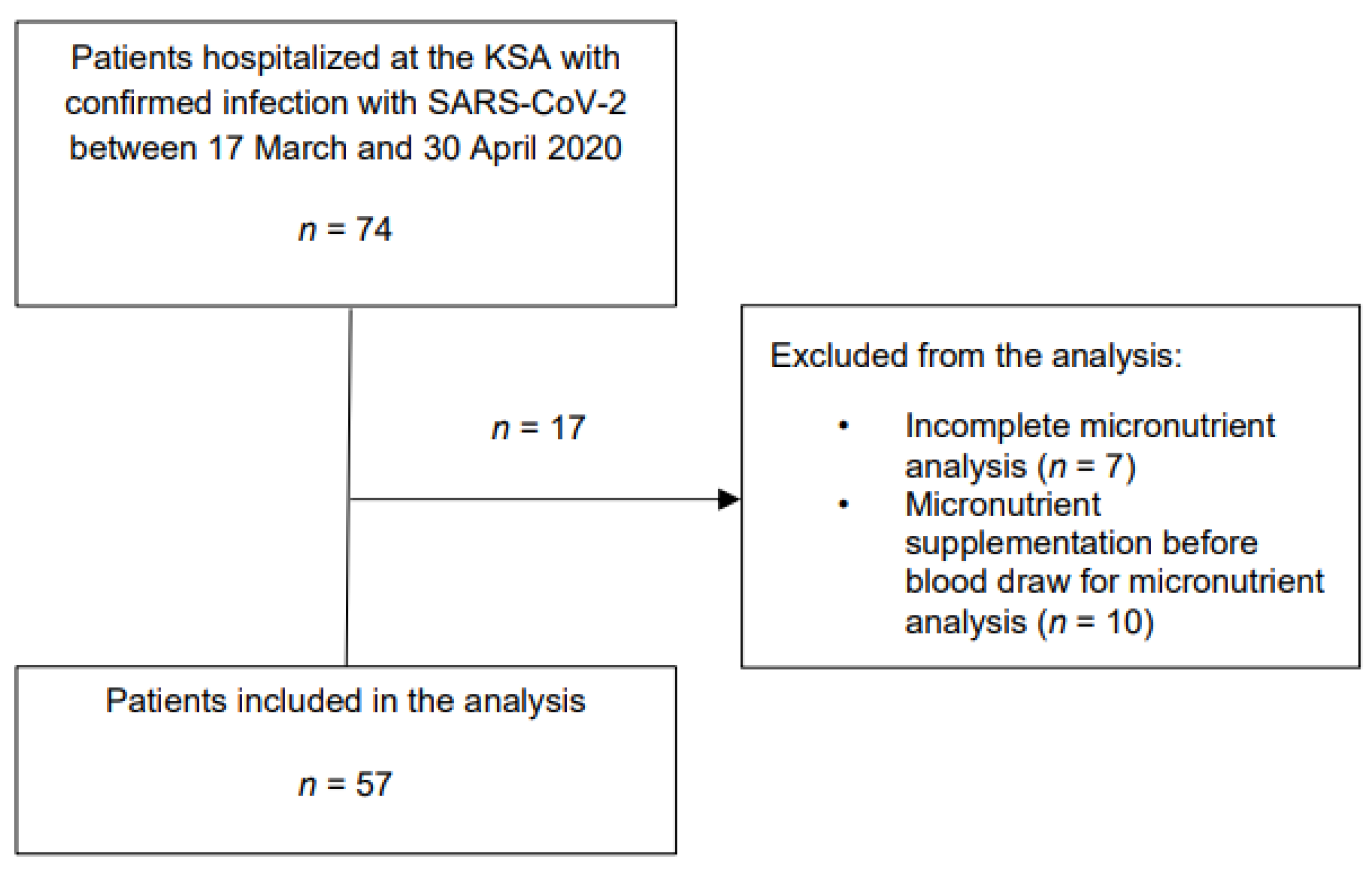
2.1. Patient Population
2.2. Data Collection
2.3. Laboratory Analysis
2.4. Outcomes
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Correlation of Different Micronutrient Values
3.3. Association of Micronutrient Levels with ICU Admission and In-Hospital Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 24 February 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef] [PubMed]
- Conzade, R.; Koenig, W.; Heier, M.; Schneider, A.; Grill, E.; Peters, A.; Thorand, B. Prevalence and Predictors of Subclinical Micronutrient Deficiency in German Older Adults: Results from the Population-Based KORA-Age Study. Nutrients 2017, 9, 1276. [Google Scholar] [CrossRef] [Green Version]
- Chandra, R.K. Nutrition and the immune system from birth to old age. Eur. J. Clin. Nutr. 2002, 56 (Suppl. S3), S73–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.M.; Herter-Aeberli, I.; Zimmermann, M.B.; Spieldenner, J.; Eggersdorfer, M. Strengthening the immunity of the Swiss population with micronutrients: A narrative review and call for action. Clin. Nutr. ESPEN 2021, 43, 39–48. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System-Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [Green Version]
- Stephensen, C.B. Vitamin A, infection, and immune function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef]
- Wintergerst, E.S.; Maggini, S.; Hornig, D.H. Immune-enhancing role of vitamin C and zinc and effect on clinical conditions. Ann. Nutr. Metab. 2006, 50, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Gammoh, N.Z.; Rink, L. Zinc in Infection and Inflammation. Nutrients 2017, 9, 624. [Google Scholar] [CrossRef] [Green Version]
- Gombart, A.F. The vitamin D-antimicrobial peptide pathway and its role in protection against infection. Future Microbiol. 2009, 4, 1151–1165. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.; Li, W. The Roles of Vitamin D and Its Analogs in Inflammatory Diseases. Curr. Top. Med. Chem. 2016, 16, 1242–1261. [Google Scholar] [CrossRef]
- Baktash, V.; Hosack, T.; Patel, N.; Shah, S.; Kandiah, P.; Van den Abbeele, K.; Mandal, A.K.J.; Missouris, C.G. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad. Med. J. 2021, 97, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low vitamin D levels do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Jothimani, D.; Kailasam, E.; Danielraj, S.; Nallathambi, B.; Ramachandran, H.; Sekar, P.; Manoharan, S.; Ramani, V.; Narasimhan, G.; Kaliamoorthy, I.; et al. COVID-19: Poor outcomes in patients with zinc deficiency. Int. J. Infect. Dis. 2020, 100, 343–349. [Google Scholar] [CrossRef]
- Tomasa-Irriguible, T.M.; Bielsa-Berrocal, L.; Bordeje-Laguna, L.; Tural-Llacher, C.; Barallat, J.; Manresa-Dominguez, J.M.; Toran-Monserrat, P. Low Levels of Few Micronutrients May Impact COVID-19 Disease Progression: An Observational Study on the First Wave. Metabolites 2021, 11, 565. [Google Scholar] [CrossRef]
- Du Laing, G.; Petrovic, M.; Lachat, C.; De Boevre, M.; Klingenberg, G.J.; Sun, Q.; De Saeger, S.; De Clercq, J.; Ide, L.; Vandekerckhove, L.; et al. Course and Survival of COVID-19 Patients with Comorbidities in Relation to the Trace Element Status at Hospital Admission. Nutrients 2021, 13, 3304. [Google Scholar] [CrossRef]
- Razeghi Jahromi, S.; Moradi Tabriz, H.; Togha, M.; Ariyanfar, S.; Ghorbani, Z.; Naeeni, S.; Haghighi, S.; Jazayeri, A.; Montazeri, M.; Talebpour, M.; et al. The correlation between serum selenium, zinc, and COVID-19 severity: An observational study. BMC Infect. Dis. 2021, 21, 899. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Gregoriano, C.; Keller, U. Supplementation of the population during the COVID-19 pandemic with vitamins and micronutrients—How much evidence is needed? Swiss Med Wkly 2021, 151, w20522. [Google Scholar] [CrossRef]
- Federal Commission for Nutrition. Vitamin D Deficiency: Evidence, Safety, and Recommendations for the Swiss Population; Expert Report of the FCN; Federal Office for Public Health: Zurich, Switzerland, 2012. [Google Scholar]
- Schupbach, R.; Wegmuller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Gregoriano, C.; Koch, D.; Haubitz, S.; Conen, A.; Fux, C.A.; Mueller, B.; Bernasconi, L.; Hammerer-Lercher, A.; Oberle, M.; Burgermeister, S.; et al. Characteristics, predictors and outcomes among 99 patients hospitalised with COVID-19 in a tertiary care centre in Switzerland: An observational analysis. Swiss Med. Wkly. 2020, 150, w20316. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronovirus (nCov) Infection Is Suspected; Interim Guidance. 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 2 February 2022).
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Juma, S.; Taabazuing, M.M.; Montero-Odasso, M. Clinical Frailty Scale in an Acute Medicine Unit: A Simple Tool That Predicts Length of Stay. Can. Geriatr. J. 2016, 19, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z.; Ad Hoc, E.W.G. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Greaves, R.F.; Woollard, G.A.; Hoad, K.E.; Walmsley, T.A.; Johnson, L.A.; Briscoe, S.; Koetsier, S.; Harrower, T.; Gill, J.P. Laboratory medicine best practice guideline: Vitamins a, e and the carotenoids in blood. Clin. Biochem. Rev. 2014, 35, 81–113. [Google Scholar]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2021, 93, 733–740. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Bitarafan, S.; Abdollahi, A.; Amoozadeh, L.; Salahshour, F.; Mahmoodi Ali Abadi, M.; Soltani, D.; Motallebnejad, Z.A. The association between serum levels of micronutrients and the severity of disease in patients with COVID-19. Nutrition 2021, 91–92, 111400. [Google Scholar] [CrossRef]
- Elham, A.S.; Azam, K.; Azam, J.; Mostafa, L.; Nasrin, B.; Marzieh, N. Serum vitamin D, calcium, and zinc levels in patients with COVID-19. Clin. Nutr. ESPEN 2021, 43, 276–282. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef] [PubMed]
- Jaun, F.; Boesing, M.; Luthi-Corridori, G.; Abig, K.; Makhdoomi, A.; Bloch, N.; Lins, C.; Raess, A.; Grillmayr, V.; Haas, P.; et al. High-dose vitamin D substitution in patients with COVID-19: Study protocol for a randomized, double-blind, placebo-controlled, multi-center study-VitCov Trial. Trials 2022, 23, 114. [Google Scholar] [CrossRef] [PubMed]
- Im, J.H.; Je, Y.S.; Baek, J.; Chung, M.H.; Kwon, H.Y.; Lee, J.S. Nutritional status of patients with COVID-19. Int. J. Infect. Dis. 2020, 100, 390–393. [Google Scholar] [CrossRef]
- Zhang, J.; Taylor, E.W.; Bennett, K.; Saad, R.; Rayman, M.P. Association between regional selenium status and reported outcome of COVID-19 cases in China. Am. J. Clin. Nutr. 2020, 111, 1297–1299. [Google Scholar] [CrossRef] [PubMed]
- Tepasse, P.R.; Vollenberg, R.; Fobker, M.; Kabar, I.; Schmidt, H.; Meier, J.A.; Nowacki, T.; Husing-Kabar, A. Vitamin A Plasma Levels in COVID-19 Patients: A Prospective Multicenter Study and Hypothesis. Nutrients 2021, 13, 2173. [Google Scholar] [CrossRef] [PubMed]
- Sarohan, A.R.; Kizil, M.; Inkaya, A.C.; Mahmud, S.; Akram, M.; Cen, O. A novel hypothesis for COVID-19 pathogenesis: Retinol depletion and retinoid signaling disorder. Cell Signal. 2021, 87, 110121. [Google Scholar] [CrossRef]
- Mucida, D.; Park, Y.; Kim, G.; Turovskaya, O.; Scott, I.; Kronenberg, M.; Cheroutre, H. Reciprocal TH17 and regulatory T cell differentiation mediated by retinoic acid. Science 2007, 317, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghi, A.; Tahmasebi, S.; Mahmood, A.; Kuznetsova, M.; Valizadeh, H.; Taghizadieh, A.; Nazemiyeh, M.; Aghebati-Maleki, L.; Jadidi-Niaragh, F.; Abbaspour-Aghdam, S.; et al. Th17 and Treg cells function in SARS-CoV2 patients compared with healthy controls. J. Cell Physiol. 2021, 236, 2829–2839. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.M.; Haskell, M.J.; Raqib, R.; Stephensen, C.B. Markers of innate immune function are associated with vitamin a stores in men. J. Nutr. 2009, 139, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Broman, N.; Rantasarkka, K.; Feuth, T.; Valtonen, M.; Waris, M.; Hohenthal, U.; Rintala, E.; Karlsson, A.; Marttila, H.; Peltola, V.; et al. IL-6 and other biomarkers as predictors of severity in COVID-19. Ann. Med. 2021, 53, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Berardicurti, O.; Ruscitti, P.; Ursini, F.; D'Andrea, S.; Ciaffi, J.; Meliconi, R.; Iagnocco, A.; Cipriani, P.; Giacomelli, R. Mortality in tocilizumab-treated patients with COVID-19: A systematic review and meta-analysis. Clin. Exp. Rheumatol. 2020, 38, 1247–1254. [Google Scholar] [PubMed]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef]
- Fromonot, J.; Gette, M.; Ben Lassoued, A.; Gueant, J.L.; Gueant-Rodriguez, R.M.; Guieu, R. Hypozincemia in the early stage of COVID-19 is associated with an increased risk of severe COVID-19. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Liuzzi, J.P.; Lichten, L.A.; Rivera, S.; Blanchard, R.K.; Aydemir, T.B.; Knutson, M.D.; Ganz, T.; Cousins, R.J. Interleukin-6 regulates the zinc transporter Zip14 in liver and contributes to the hypozincemia of the acute-phase response. Proc. Natl. Acad. Sci. USA 2005, 102, 6843–6848. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, J.J.; Cousins, R.J. Interleukin 6 regulates metallothionein gene expression and zinc metabolism in hepatocyte monolayer cultures. Proc. Natl. Acad. Sci. USA 1990, 87, 3137–3141. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C. Feeding the immune system. Proc. Nutr. Soc. 2013, 72, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Sun, R.R.; Yan, Z.X.; Yi, W.X.; Yue, B. Correlation of serum vitamin A, D, and E with recurrent respiratory infection in children. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8133–8138. [Google Scholar] [CrossRef]
- Koekkoek, W.A.C.; Hettinga, K.; de Vries, J.H.M.; van Zanten, A.R.H. Micronutrient deficiencies in critical illness. Clin. Nutr. 2021, 40, 3780–3786. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All | No Deficiency | One Deficiency | Two Deficiencies | Multiple Deficiencies | p-Value ° | |
|---|---|---|---|---|---|---|
| n = 57 | n = 12 | n = 10 | n = 16 | n = 19 | ||
| Socio-demographics | ||||||
| Age (years), median (IQR) | 67.0 (60.0, 74.2) | 64.5 (57.8, 74.3) | 71.0 (65.1, 72.4) | 63.6 (58.9, 73.4) | 67.5 (55.9, 76.6) | 0.87 |
| Gender (male), n (%) | 34 (60) | 6 (50) | 7 (70) | 10 (63) | 11 (58) | 0.80 |
| Nationality | ||||||
| Swiss, n (%) | 37 (65) | 9 (75) | 8 (80) | 11 (69) | 9 (47) | 0.46 |
| Others, n (%) | 13 (23) | 3 (25) | 1 (10) | 3 (19) | 6 (32) | |
| Unknown, n (%) | 7 (12) | 0 (0) | 1 (10) | 2 (13) | 4 (21) | |
| Pre-existing risk-factors | ||||||
| Active smoker, n (%) | 5 (12) | 1 (11) | 1 (14) | 1 (7) | 2 (15) | 0.92 |
| Immunosuppressant, n (%) | 1 (2) | 0 (0) | 1 (10) | 0 (0) | 0 (0) | 0.19 |
| Pre-admission history | ||||||
| Transfer from another hospital, n (%) | 14 (25) | 0 (0) | 1 (10) | 6 (38) | 7 (37) | 0.05 |
| Symptom onset before admission (days), median (IQR) | 7.0 (5.0, 11.0) | 8.0 (6.0, 11.0) | 9.0 (6.0, 14.0) | 7.5 (4.5, 12.5) | 5.5 (3.0, 9.0) | 0.38 |
| Comorbidities | ||||||
| Cancer, n (%) | 5 (9) | 0 (0) | 1 (10) | 2 (13) | 2 (11) | 0.68 |
| Hypertension, n (%) | 35 (61) | 6 (50) | 7 (70) | 11 (69) | 11 (58) | 0.70 |
| Coronary artery disease, n (%) | 16 (28) | 3 (25) | 6 (60) | 3 (19) | 4 (21) | 0.10 |
| Chronic heart failure, n (%) | 3 (5) | 1 (8) | 2 (20) | 0 (0) | 0 (0) | 0.09 |
| Asthma, n (%) | 11 (19) | 2 (17) | 3 (30) | 3 (19) | 3 (16) | 0.82 |
| Chronic obstructive pulmonary disease, n (%) | 3 (5) | 0 (0) | 2 (20) | 0 (0) | 1 (5) | 0.12 |
| Obstructive sleep apnea syndrome, n (%) | 10 (18) | 2 (17) | 3 (30) | 2 (13) | 3 (16) | 0.71 |
| Active rheumatic disease, n (%) | 1 (2) | 0 (0) | 1 (10) | 0 (0) | 0 (0) | 0.19 |
| Chronic kidney disease, n (%) | 17 (30) | 3 (25) | 5 (50) | 5 (31) | 4 (21) | 0.42 |
| Diabetes, n (%) | 18 (32) | 4 (33) | 5 (50) | 3 (19) | 6 (32) | 0.42 |
| Age-adjusted Charlson comorbidity index, median (IQR) | 3.0 (2.0, 6.0) | 2.0 (1.0, 6.5) | 6.5 (2.0, 9.0) | 3.0 (2.0, 5.0) | 3.0 (2.0, 5.0) | 0.21 |
| Clinical frailty score, median (IQR) | 3.0 (2.0, 4.0) | 2.5 (2.0, 3.5) | 3.0 (3.0, 5.0) | 3.0 (3.0, 5.0) | 3.0 (2.0, 4.0) | 0.51 |
| Outcomes | ||||||
| Length of hospital stay (days), median (IQR) | 9.0 (5.0, 14.0) | 5.0 (4.0, 8.5) | 5.0 (4.0, 10.0) | 10.0 (8.0, 11.5) | 19.0 (6.0, 22.0) | 0.02 |
| ICU admission, n (%) | 12 (21) | 0 (0) | 0 (0) | 3 (19) | 9 (47) | <0.01 |
| Need for mechanical ventilation, n (%) | 10 (18) | 0 (0) | 0 (0) | 2 (13) | 8 (42) | <0.01 |
| In-hospital death, n (%) | 6 (11) | 0 (0) | 3 (30) | 1 (6) | 2 (11) | 0.12 |
| Micronutrients | ||||||
| Vitamin A | ||||||
| Median (μmol/L), (IQR) | 1.2 (0.8, 1.7) | 1.8 (1.6, 2.5) | 1.9 (1.4, 2.4) | 1.0 (0.7, 1.4) | 0.8 (0.6, 1.1) | <0.01 |
| Deficiency, n (%) | 22 (39) | 0 (0) | 1 (10) | 8 (50) | 13 (68) | <0.01 |
| Vitamin B12 | ||||||
| Median (pmol/L), (IQR) | 292.0 (207.0, 548.0) | 255.0 (213.0, 560.0) | 268.0 (171.0, 493.0) | 545.0 (335.5, 706.0) | 237.0 (182.0, 310.0) | 0.04 |
| Deficiency, n (%) | 4 (7) | 0 (0) | 0 (0) | 1 (6) | 3 (16) | 0.27 |
| Vitamin D | ||||||
| Median (nmol/L), (IQR) | 34.6 (24.3, 62.2) | 61.0 (51.2, 80.2) | 65.0 (36.4, 70.0) | 32.4 (26.8, 52.0) | 23.6 (15.2, 31.5) | <0.01 |
| Deficiency, n (%) | 23 (40) | 0 (0) | 2 (20) | 7 (44) | 14 (74) | <0.01 |
| Vitamin E | ||||||
| Mean (μmol/L), (SD) | 32.9 (8.6) | 35.7 (7.5) | 31.6 (8.3) | 35.2 (10.1) | 30.0 (7.7) | 0.19 |
| Deficiency, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | n.a. |
| Folic acid | ||||||
| Median (nmol/L), (IQR) | 15.0 (10.2, 23.3) | 18.4 (13.6, 23.9) | 19.6 (11.7, 27.6) | 15.3 (9.7, 21.6) | 11.8 (8.2, 17.9) | 0.07 |
| Deficiency, n (%) | 3 (5) | 0 (0) | 0 (0) | 0 (0) | 3 (16) | 0.10 |
| Zinc | ||||||
| Median (μmol/L), (IQR) | 10.9 (8.8, 12.8) | 13.9 (12.4, 16.0) | 12.6 (11.4, 14.4) | 10.7 (8.5, 11.7) | 9.3 (8.3, 10.7) | <0.01 |
| Deficiency, n (%) | 22 (39) | 0 (0) | 2 (20) | 7 (44) | 13 (68) | <0.01 |
| Selenium | ||||||
| Mean (μmol/L), (SD) | 0.96 (0.29) | 1.20 (0.18) | 1.06 (0.28) | 0.92 (0.26) | 0.78 (0.24) | <0.01 |
| Deficiency, n (%) | 29 (51) | 0 (0) | 5 (50) | 9 (56) | 15 (79) | <0.01 |
| Copper | ||||||
| Mean (μmol/L), (SD) | 21.2 (4.0) | 21.3 (3.3) | 22.1 (3.6) | 21.3 (4.4) | 20.7 (4.4) | 0.85 |
| Deficiency, n (%) | 1 (2) | 0 (0) | 0 (0) | 0 (0) | 1 (5) | 0.57 |
| Nutritional assessment | ||||||
| NRS ≥ 3, n (%) | 8 (19) | 0 (0) | 3 (38) | 2 (20) | 3 (19) | 0.27 |
| BMI | ||||||
| 18.5–24.9 kg/m2, n (%) | 15 (33) | 3 (33) | 0 (0) | 6 (46) | 6 (38) | 0.36 |
| 25–29.9 kg/m2, n (%) | 17 (37) | 4 (44) | 5 (63) | 4 (31) | 4 (25) | |
| ≥30 kg/m2, n (%) | 14 (30) | 2 (22) | 3 (38) | 3 (23) | 6 (38) |
| Vitamin A | Vitamin B12 | Vitamin D | Vitamin E | Folic Acid | Zinc | Selenium | Copper | |
|---|---|---|---|---|---|---|---|---|
| Vitamin A | 1 | |||||||
| Vitamin B12 | −0.28, p = 0.04 | 1 | ||||||
| Vitamin D | 0.27, p = 0.04 | −0.04, p = 0.75 | 1 | |||||
| Vitamin E | 0.24, p = 0.08 | 0.19, p = 0.15 | 0.08, p = 0.56 | 1 | ||||
| Folic acid | 0.21, p = 0.11 | −0.008, p = 0.95 | 0.39, p = 0.002 | 0.04, p = 0.79 | 1 | |||
| Zinc | 0.42, p = 0.001 | −0,17, p = 0.22 | 0.19, p = 0.16 | 0.18, p = 0.18 | −0.03, p = 0.83 | 1 | ||
| Selenium | 0.20, p = 0.13 | 0.07, p = 0.59 | 0.32, p = 0.02 | 0.25, p = 0.06 | 0.30, p = 0.02 | 0.26, p = 0.05 | 1 | |
| Copper | −0.07, p = 0.58 | −0.04, p = 0.75 | −0.14, p = 0.28 | 0.26, p = 0.05 | 0.05, p = 0.72 | 0.37, p = 0.004 | 0.29, p = 0.03 | 1 |
| Mild Disease | Severe Disease | p-Value ° | Univariable OR (95% CI), p-Value | Adjusted OR * (95% CI), p-Value | |
|---|---|---|---|---|---|
| n = 42 | n = 15 | ||||
| Vitamin A | |||||
| Median (μmol/L), (IQR) | 1.5 (1.0, 2.0) | 0.7 (0.4, 1.1) | <0.01 | 0.17 (0.05–0.66), p = 0.01 | 0.18 (0.05–0.69), p = 0.01 |
| Deficiency, n (%) | 11 (26) | 11 (73) | <0.01 | 7.75 (2.04–29.46), p = 0.003 | 7.41 (1.91–28.68), p = 0.004 |
| Vitamin B12 | |||||
| Median (pmol/L), (IQR) | 290.0 (200.0, 597.0) | 310.0 (220.0, 497.0) | 0.82 | 1.00 (0.99–1.00), p = 0.91 | 1.00 (0.99–1.00), p = 0.91 |
| Deficiency, n (%) | 4 (10) | 0 (0) | 0.22 | n.a. | n.a. |
| Vitamin D | |||||
| Median (nmol/L), (IQR) | 34.4 (24.3, 65.0) | 34.6 (16.2, 46.8) | 0.31 | 0.99 (0.96–1.01), p = 0.32 | 0.99 (0.96–1.01), p = 0.38 |
| Deficiency, n (%) | 16 (38) | 7 (47) | 0.56 | 1.42 (0.43–4.68), p = 0.56 | 1.44 (0.43–4.79), p = 0.55 |
| Vitamin E | |||||
| Mean (μmol/L), (SD) | 33.1 (9.0) | 32.5 (7.7) | 0.81 | 0.99 (0.92–1.06), p = 0.81 | 0.99 (0.93–1.07), p = 0.88 |
| Deficiency, n (%) | 0 (0) | 0 (0) | n.a. | n.a. | n.a. |
| Folic acid | |||||
| Median (nmol/L), (IQR) | 16.6 (11.4, 24.0) | 10.2 (8.2, 14.4) | <0.01 | 0.88 (0.79–0.98), p = 0.02 | 0.88 (0.78–0.98), p = 0.02 |
| Deficiency, n (%) | 0 (0) | 3 (20) | <0.01 | n.a. | n.a. |
| Zinc | |||||
| Median (μmol/L), (IQR) | 11.7 (9.8, 13.5) | 9.3 (8.3, 11.4) | 0.03 | 0.77 (0.60–0.99), p = 0.04 | 0.73 (0.55–0.98), p = 0.03 |
| Deficiency, n (%) | 12 (29) | 10 (67) | <0.01 | 5 (1.41–17.72), p = 0.01 | 7.18 (1.73–29.76), p = 0.007 |
| Selenium | |||||
| Mean (μmol/L), (SD) | 0.9 (0.3) | 1.0 (0.3) | 0.66 | 1.62 (0.20–13.11), p = 0.65 | 1.39 (0.16–12.27), p = 0.77 |
| Deficiency, n (%) | 21 (50) | 8 (53) | 0.82 | 1.14 (0.35–3.72), p = 0.83 | 1.19 (0.36–3.93), p = 0.77 |
| Copper | |||||
| Mean (μmol/L), (SD) | 21.2 (4.4) | 21.3 (2.9) | 0.93 | 1.00 (0.87–1.17), p = 0.92 | 1.00 (0.86–1.16), p = 0.99 |
| Deficiency, n (%) | 1 (2) | 0 (0) | 0.55 | n.a. | n.a. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voelkle, M.; Gregoriano, C.; Neyer, P.; Koch, D.; Kutz, A.; Bernasconi, L.; Conen, A.; Mueller, B.; Schuetz, P. Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study. Nutrients 2022, 14, 1862. https://doi.org/10.3390/nu14091862
Voelkle M, Gregoriano C, Neyer P, Koch D, Kutz A, Bernasconi L, Conen A, Mueller B, Schuetz P. Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study. Nutrients. 2022; 14(9):1862. https://doi.org/10.3390/nu14091862
Chicago/Turabian StyleVoelkle, Manyola, Claudia Gregoriano, Peter Neyer, Daniel Koch, Alexander Kutz, Luca Bernasconi, Anna Conen, Beat Mueller, and Philipp Schuetz. 2022. "Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study" Nutrients 14, no. 9: 1862. https://doi.org/10.3390/nu14091862
APA StyleVoelkle, M., Gregoriano, C., Neyer, P., Koch, D., Kutz, A., Bernasconi, L., Conen, A., Mueller, B., & Schuetz, P. (2022). Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study. Nutrients, 14(9), 1862. https://doi.org/10.3390/nu14091862