

Beneficial Effects of Oral Nutrition Supplements on the Nutritional Status and Physical Performance of Older Nursing Home Residents at Risk of Malnutrition

Abstract
:1. Introduction
2. Materials and Methods
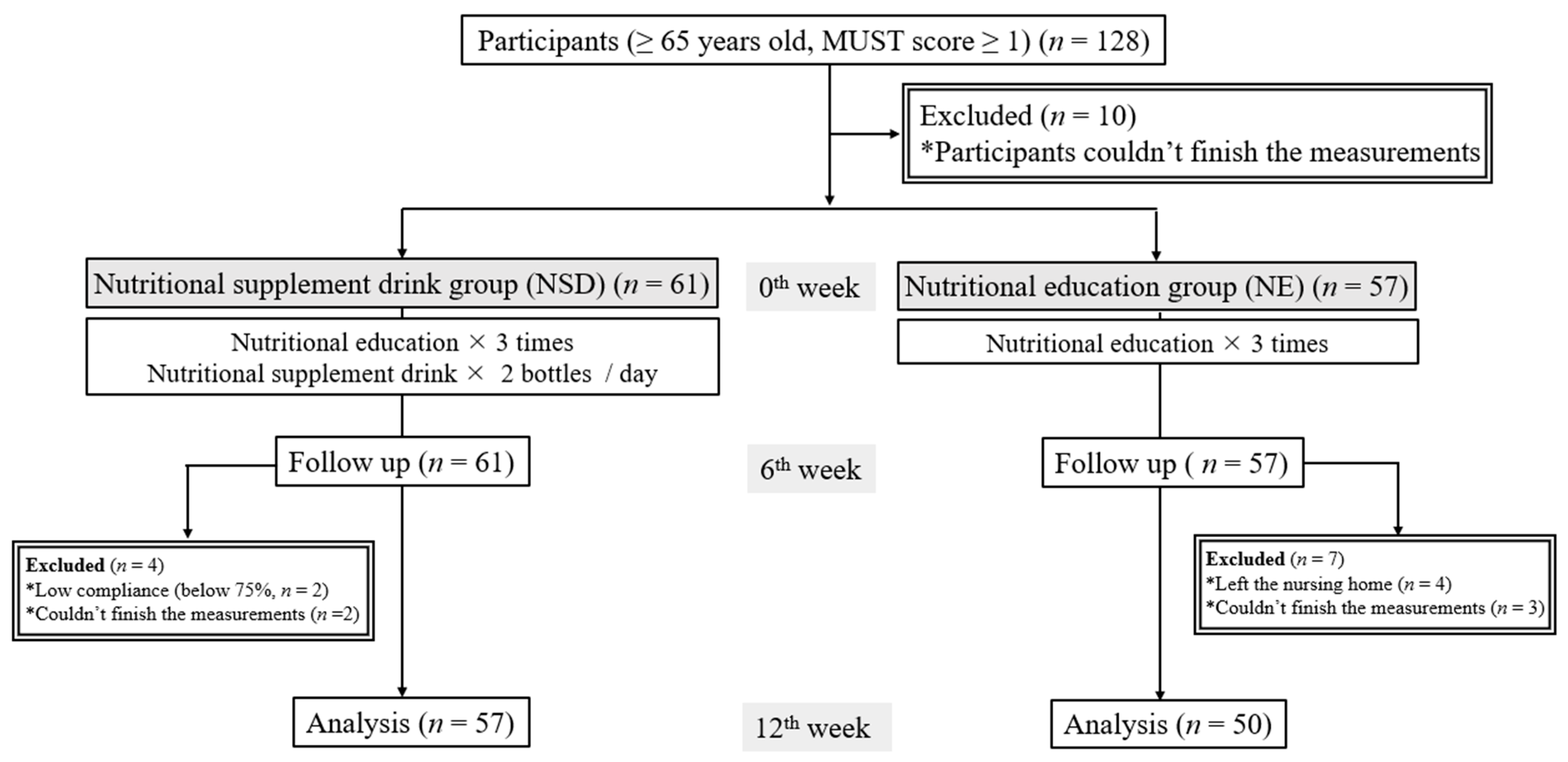
2.1. Study Design
2.2. Participant Recruitment
2.3. Anthropometric Data
2.4. Blood Pressure
2.5. Physical Performance
2.6. Dietary Calorie Intake and Nutritional Status
2.7. Blood Biochemical Analyses
2.8. QOL and Health Status
2.9. Statistical Analysis
3. Results
3.1. Basic Information
3.2. Baseline Demographics, Anthropometric Assessments, and Dietary Intake of Study Participants
3.3. Body Composition, Physical Performance, and Nutritional Status
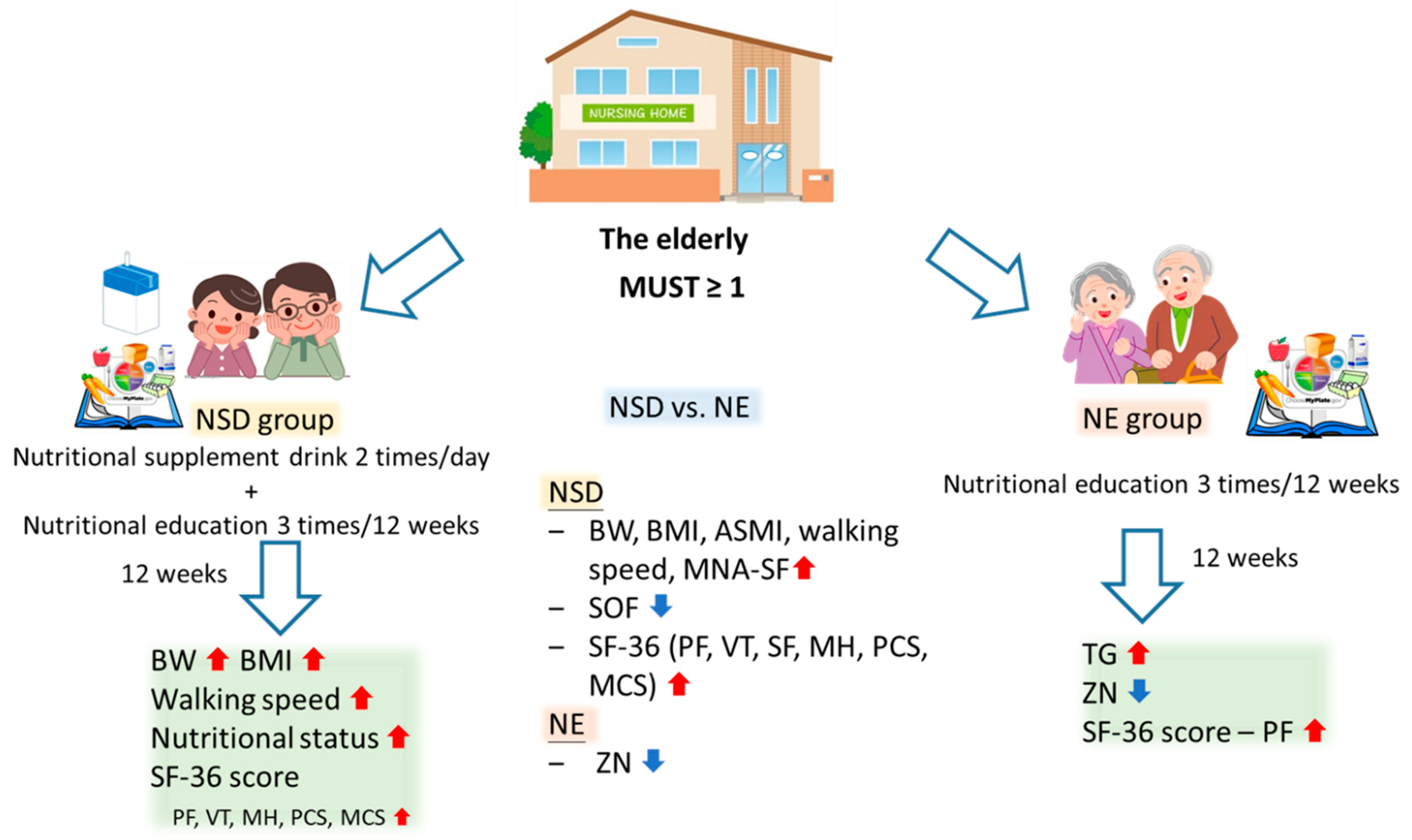
3.3.1. Changes after the NSD Intervention
3.3.2. Changes after the NE Intervention
3.3.3. Comparisons of the Effects between NSD and NE
3.4. Blood Biochemical Analysis
3.5. Vit. D and Zinc Deficiencies
3.5.1. Changes after the NSD Intervention
3.5.2. Changes after the NE Intervention
3.5.3. Comparison of the Vit. D and Zinc Statuses between the NSD and NE Groups
3.6. Effects of NSDs on Variables at Week 12, as Analyzed by a Multiple Linear Regression
3.6.1. Body Composition, Physical Performance, and Nutritional Status
3.6.2. Blood Biochemical Analysis
3.7. Odds Ratio (OR)
3.8. QOL and SF-36 Questionnaire
3.8.1. Effects of the NSD or NE Interventions
3.8.2. Changes in SF-36 Questionnaire Scores after the NSD and NE Interventions
3.9. Correlations among the SF-36 Questionnaire, the Nutritional Status, Physical Performance, Vit. D, and the Intervention
4. Discussion
4.1. ONSs, BW, Body Composition, and Physical Performance
4.2. Effects of the NSD on Related Variables
4.3. Blood Albumin Levels and Related Variables
4.4. Vit. D and Zn Deficiencies
4.5. Crude and Adjusted ORs
4.6. Nutritional Status and QoL
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The World Health Report 2008: Primary Health Care Now More than Ever. Available online: https://apps.who.int/iris/handle/10665/43949 (accessed on 20 July 2023).
- Watanabe, Y.; Hirano, H.; Arai, H.; Morishita, S.; Ohara, Y.; Edahiro, A.; Murakami, M.; Shimada, H.; Kikutani, T.; Suzuki, T. Relationship between frailty and oral function in community-dwelling elderly adults. J. Am. Geriatr. Soc. 2017, 65, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Umegaki, H.; Asai, A.; Kanda, S.; Maeda, K.; Shimojima, T.; Nomura, H.; Kuzuya, M. Factors associated with unexpected admissions and mortality among low-functioning older patients receiving home medical care. Geriatr. Gerontol. Int. 2017, 17, 1623–1627. [Google Scholar] [CrossRef]
- World Health Organization. Evidence Profile: Malnutrition. Integrated Care for Older People (ICOPE). 2017. Available online: https://www.who.int/publications/i/item/WHO-MCA-17.06.06 (accessed on 5 October 2023).
- Algra, Y.; Haverkort, E.; Kok, W.; Etten-Jamaludin, F.V.; Schoot, L.V.; Hollaar, V.; Naumann, E.; Schueren, M.V.; Jerković-Ćosić, K. The Association between Malnutrition and Oral Health in Older People: A Systematic Review. Nutrients 2021, 13, 3584. [Google Scholar] [CrossRef] [PubMed]
- Stechmiller, J.K. Early nutritional screening of older adults: Review of nutritional support. J. Infus. Nurs. Off. Publ. Infus. Nurses Soc. 2003, 26, 170–177. [Google Scholar] [CrossRef]
- Chan, L.C.; Kao, S.y.; Chin, H.M.L.; Lee, M.S. Nutritional status assessment and predictors of community-dwelling and in-stitutionalized elderly in northern Taiwan. Nutr. Sci. J. 2002, 27, 147–158. [Google Scholar] [CrossRef]
- Lin, C.H.; Chang, H.Y.; Li, T.C.; Liu, C.S.; Lin, W.Y.; Lee, M.C.; Liao, L.N.; Li, C.I.; Hsiao, C.Y.; Fang, H.L.; et al. Trends in energy and macronutrient intake among Taiwanese older adults in 1999–2000, 2005–2008 and 2013–2016 periods. BMC Public Health 2023, 23, 871. [Google Scholar] [CrossRef]
- Wu, S.C. A new turning point of long term care policy in Taiwan. J. Long-Term Care 2017, 21, 1–7. [Google Scholar]
- Cramer, J.T.; Cruz-Jentoft, A.J.; Landi, F.; Hickson, M.; Zamboni, M.; Pereira, S.L.; Hustead, D.S.; Mustad, V.A. Impacts of high-protein oral nutritional supplements among malnourished men and women with sarcopenia: A multicenter, randomized, double-blinded, controlled trial. J. Am. Med. Dir. Assoc. 2016, 17, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Nasser, R.; Banow, T.; Cockburn, T.; Voegeli, L.; Wilson, O.; Coleman, J. Use of oral nutrition supplements in long-term care facilities. Can. J. Diet. Pract. Res. A Publ. Dietit. Can. 2009, 70, 194–198. [Google Scholar] [CrossRef]
- Chew, S.T.H.; Tan, N.C.; Cheong, M.; Oliver, J.; Baggs, G.; Choe, Y.; How, C.H.; Chow, W.L.; Tan, C.Y.L.; Kwan, S.C.; et al. Impact of specialized oral nutritional supplement on clinical, nutritional, and functional outcomes: A randomized, placebo-controlled trial in community-dwelling older adults at risk of malnutrition. Clin. Nutr. 2021, 40, 1879–1892. [Google Scholar] [CrossRef]
- Rea, J.; Walters, K.; Avgerinou, C. How effective is nutrition education aiming to prevent or treat malnutrition in community-dwelling older adults? A systematic review. Eur. Geriatr. Med. 2019, 10, 339–358. [Google Scholar]
- Lyons, B.P. Nutrition education intervention with community-dwelling older adults: Research challenges and opportunities. J. Community Health 2014, 39, 810–818. [Google Scholar] [CrossRef]
- Mann, T.; Heuberger, R.; Wong, H. The association between chewing and swallowing difficulties and nutritional status in older adults. Aust. Dent. J. 2013, 58, 200–206. [Google Scholar] [CrossRef]
- Zhou, X.; Perez-Cueto, F.J.A.; Santos, Q.D.; Monteleone, E.; Giboreau, A.; Appleton, K.M.; Bjørner, T.; Bredie, W.L.P.; Hartwell, H. A systematic review of behavioural interventions promoting healthy eating among older people. Nutrients 2018, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- de van der Schueren, M.A. Use and effects of oral nutritional supplements in patients with cancer. Nutrition 2019, 67, 110550. [Google Scholar]
- Parsons, E.L.; Stratton, R.J.; Cawood, A.L.; Smith, T.R.; Elia, M. Oral nutritional supplements in a randomised trial are more effective than dietary advice at improving quality of life in malnourished care home residents. Clin. Nutr. 2017, 36, 134–142. [Google Scholar] [CrossRef]
- Perna, S.; Rondanelli, M.; Spadaccini, D.; Lenzi, A.; Donini, L.; Poggiogalle, E. Are the therapeutic strategies in anorexia of ageing effective on nutritional status? A systematic review with meta-analysis. J. Hum. Nutr. Diet. 2019, 32, 128–138. [Google Scholar] [PubMed]
- Ensrud, K.E.; Ewing, S.K.; Cawthon, P.M.; Fink, H.A.; Taylor, B.C.; Cauley, J.A.; Dam, T.T.; Marshall, L.M.; Orwoll, E.S.; Cummings, S.R. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J. Am. Geriatr. Soc. 2009, 57, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Jenkinson, C.; Coulter, A.; Wright, L. Short form 36 (SF36) health survey questionnaire: Normative data for adults of working age. BMJ Clin. Res. Ed. 1993, 306, 1437–1440. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Hébuterne, X.; Bermon, S.; Schneider, S.M. Ageing and muscle: The effects of malnutrition, re-nutrition, and physical exercise. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Roberts, S.L.; Halmi, K.A.; Goldberg, S.C. Caloric requirements for weight gain in anorexia nervosa. Am. J. Clin. Nutr. 1979, 32, 1396–1400. [Google Scholar] [CrossRef]
- Hébuterne, X.; Broussard, J.F.; Rampal, P. Acute renutrition by cyclic enteral nutrition in elderly and younger patients. JAMA 1995, 273, 638–643. [Google Scholar] [CrossRef]
- Loman, B.R.; Luo, M.; Baggs, G.E.; Mitchell, D.C.; Nelson, J.L.; Ziegler, T.R.; Deutz, N.E.; Matarese, L.E. Specialized high-protein oral nutrition supplement improves home nutrient intake of malnourished older adults without decreasing usual food intake. JPEN J. Parenter. Enter. Nutr. 2019, 43, 794–802. [Google Scholar] [CrossRef]
- Anton, S.D.; Hida, A.; Mankowski, R.; Layne, A.; Solberg, L.M.; Mainous, A.G.; Buford, T. Nutrition and exercise in sarcopenia. Curr. Protein Pept. Sci. 2018, 19, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.B.; Foley, A.L.; Barnard, R.; Isenring, E.A.; Miller, M.D. Nutritional screening in community-dwelling older adults: A systematic literature review. Asia Pac. J. Clin. Nutr. 2010, 19, 440–449. [Google Scholar]
- Nakamura, H.; Kita, N.; Tanimoto, K.; Kunikata, C.; Taoka, T. Usefulness of nutrition screening tools for sarcopenia screening with chronic obstructive pulmonary disease in JAPAN. Eur. Respir. Soc. 2018, 52, PA70. [Google Scholar]
- Poulia, K.A.; Yannakoulia, M.; Karageorgou, D.; Gamaletsou, M.; Panagiotakos, D.B.; Sipsas, N.V.; Zampelas, A. Evaluation of the efficacy of six nutritional screening tools to predict malnutrition in the elderly. Clin. Nutr. 2012, 31, 378–385. [Google Scholar] [CrossRef]
- Gom, I.; Fukushima, H.; Shiraki, M.; Miwa, Y.; Ando, T.; Takai, K.; Moriwaki, H. Relationship between serum albumin level and aging in community-dwelling self-supported elderly population. J. Nutr. Sci. Vitaminol. 2007, 53, 37–42. [Google Scholar] [CrossRef]
- Cabrerizo, S.; Cuadras, D.; Gomez-Busto, F.; Artaza-Artabe, I.; Marín-Ciancas, F.; Malafarina, V. Serum albumin and health in older people: Review and meta analysis. Maturitas 2015, 81, 17–27. [Google Scholar] [CrossRef]
- Kitamura, K.; Nakamura, K.; Nishiwaki, T.; Ueno, K.; Nakazawa, A.; Hasegawa, M. Determination of whether the association between serum albumin and activities of daily living in frail elderly people is causal. Environ. Health Prev. Med. 2012, 17, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Pilz, S.; Hoffmann, H.; März, W. Vitamin D and airway infections: A European perspective. Eur. J. Med. Res. 2016, 21, 14. [Google Scholar] [CrossRef] [PubMed]
- Arnljots, R.; Thorn, J.; Elm, M.; Moore, M.; Sundvall, P.D. Vitamin D deficiency was common among nursing home residents and associated with dementia: A cross sectional study of 545 Swedish nursing home residents. BMC Geriatr. 2017, 17, 229. [Google Scholar] [CrossRef]
- Lee, M.J.; Hsu, H.J.; Wu, I.W.; Sun, C.Y.; Ting, M.K.; Lee, C.C. Vitamin D deficiency in northern Taiwan: A community-based cohort study. BMC Public Health 2019, 19, 337. [Google Scholar] [CrossRef]
- Sales, M.C.; de Oliveira, L.P.; de Araújo Cabral, N.L.; de Sousa, S.E.S.; das Graças Almeida, M.; Lemos, T.; de Oliveira Lyra, C.; de Lima, K.C.; Sena-Evangelista, K.C.M.; de Fatima Campos Pedrosa, L. Plasma zinc in institutionalized elderly individuals: Relation with immune and cardiometabolic biomarkers. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. (GMS) 2018, 50, 615–621. [Google Scholar] [CrossRef]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lönnerdal, B.; Ruel, M.T.; Sandtröm, B.; Wasantwisut, E.; Hotz, C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar]
- Kyle, U.G.; Genton, L.; Hans, D.; Pichard, C. Validation of a bioelectrical impedance analysis equation to predict appendicular skeletal muscle mass (ASMM). Clin. Nutr. 2003, 22, 537–543. [Google Scholar] [CrossRef]
- Gallagher, D.; Visser, M.; De Meersman, R.E.; Sepúlveda, D.; Baumgartner, R.N.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. Appendicular skeletal muscle mass: Effects of age, gender, and ethnicity. J. Appl. Physiol. 1997, 83, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Wang, M.; Jiang, C.M.; Zhang, Y.M. Anthropometric equation for estimation of appendicular skeletal muscle mass in Chinese adults. Asia Pac. J. Clin. Nutr. 2011, 20, 551–556. [Google Scholar] [PubMed]
- Kuriyan, R. Body composition techniques. Indian J. Med. Res. 2018, 148, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Liu, L.K.; Hwang, A.C.; Lin, M.H.; Peng, L.N.; Chen, L.K.; Lan, C.F.; Chang, P.L. Impact of malnutrition on physical, cognitive function and mortality among older men living in veteran homes by minimum data set: A prospective cohort study in Taiwan. J. Nutr. Health Aging 2016, 20, 41–47. [Google Scholar] [CrossRef]
- Kung, Y.L.; Cai, M.T.; Liu, C.H. Impact of aboriginal operational capacity on nutrition and melancholy in long term care. J. Health Manag. 2018, 16, 23–42. [Google Scholar]
- Adeel, M.; Lai, C.H.; Wu, C.W.; Kang, J.H.; Liou, J.C.; Chen, H.C.; Hong, M.J.; Peng, C.W. Energy expenditure during acute weight training exercises in healthy participants: A preliminary study. Appl. Sci. 2021, 11, 6687. [Google Scholar]
- Adeel, M.; Lai, C.H.; Wu, C.W.; Kang, J.H.; Liou, J.C.; Chen, H.C.; Lin, B.S.; Hong, M.J.; Feng, C.T.; Peng, C.W. Modeling of metabolic equivalents (Mets) during moderate resistance training exercises. Appl. Sci. 2021, 11, 8773. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 125 mL per Pack | |||||
|---|---|---|---|---|---|
| Energy | 203 kcal | ||||
| 1.62 kcal/mL | Vitamin B12 | 1.2 μg | |||
| Protein | 7.5 g | Folic acid | 60 mg | ||
| Branched-chain amino acids 1 | 1580 mg | Pantothenic acid | 1.2 mg | ||
| Leucine | 720mg | Biotin | 30 μg | ||
| Fat | 5.6 g | Vitamin C | 100 mg | ||
| Saturated fat | 1.2 g | Choline | 1.5 mg | ||
| Trans-fat | 0 g | Potassium | (sweet flavor 2) | 180 mg | |
| Carbohydrates | 31.8 g | (corn soup flavor) | 200 mg | ||
| Sugar | 5.8 g | Chlorine | (sweet flavor 2) | 120 mg | |
| Dietary fiber | 2.5 g | (corn soup flavor) | 220 mg | ||
| Sodium | (sweet flavor 2) | 130 mg | Calcium | 120 mg | |
| (corn soup flavor) | 180 mg | Phosphorus | 140 mg | ||
| Vitamin A | 120 μg RE | Magnesium | 40 mg | ||
| Vitamin D | 1.2 μg | Iron | 1.5 mg | ||
| Vitamin E | 6 mg α-TE | Zinc | 2 mg | ||
| Vitamin K | 19 μg | Manganese | 0.46 mg | ||
| Vitamin B1 | 0.3 mg | Iodine | 30 μg | ||
| Vitamin B2 | 0.4 mg | Selenium | 12 μg | ||
| Niacin | 5.4 mg NE | Molybdenum | 10 μg | ||
| Vitamin B6 | 0.6 mg | Chromium | 6 μg | ||
| NSD (N = 57) | NE (N = 50) | p-Value | |
|---|---|---|---|
| Age (years) | 80.67 ± 9.03 | 75.86 ± 8.21 | 0.007 |
| <75, n (%) | 38 (66.7) | 24 (48.0) | 0.051 |
| ≥75, n (%) | 19 (33.3) | 26 (52.0) | |
| Sex | |||
| Male n, (%) | 46 (80.7) | 32 (64.0) | 0.052 |
| Female n, (%) | 11 (19.3) | 18 (36.0) | |
| Height (cm) | 162.04 ± 7.61 | 162.47 ± 9.39 | 0.793 |
| BW (kg) | 53.73 ± 8.31 | 62.91 ± 13.57 | <0.001 |
| BMI (kg/m2) | 20.47 ± 3.03 | 23.74 ± 4.30 | <0.001 |
| Body fat (%) | 25.97 ± 5.92 | 27.03 ± 5.08 | 0.326 |
| ASMI (kg/m2) | 5.38 ± 0.95 | 6.38 ± 1.38 | <0.001 |
| Normal, n (%) | 5 (8.8) | 24 (48.0) | <0.001 |
| Low, n (%) | 52 (91.2) | 26 (52.0) | |
| Calf circumference (cm) | 31.98 ± 3.40 | 32.95 ± 4.05 | 0.177 |
| Normal, n (%) | 20 (35.1) | 25 (50.0) | 0.169 |
| Low, n (%) | 37 (64.9) | 25 (50.0) | |
| SBP (mmHg) | 133 ± 17 | 132 ± 17 | 0.871 |
| DBP (mmHg) | 78 ± 11 | 77 ± 10 | 0.609 |
| MUST | |||
| 1, n (%) | 37 (64.9) | 41 (82.0) | 0.007 |
| 2, n (%) | 19 (17.8) | 9 (18.0) | |
| 3, n (%) | 10 (9.3) | 0 (0.0) | |
| MNA-SF | 9.07 ± 1.83 | 10.66 ± 1.92 | <0.001 |
| Normal 12–14, n (%) | 7 (12.3) | 20 (40.0) | 0.002 |
| Low 0–11, n (%) | 50 (87.7) | 30 (60.0) | |
| Total energy intake (kcal) | 1213.86 ± 69.53 | 1219.00 ± 67.68 | 0.315 |
| SOF | 0.98 ± 0.64 | 0.50 ± 0.61 | <0.001 |
| Normal, n (%) | 12 (21.1) | 28 (56.0) | <0.001 |
| pre-frailty & frailty, n (%) | 45 (78.9) | 22 (44.0) | |
| Grip strength (kg) | 21.66 ± 6.14 | 21.64 ± 8.09 | 0.991 |
| Normal, n (%) | 13 (22.8) | 16 (32.0) | 0.384 |
| Low, n (%) | 44 (77.2) | 34 (68.0) | |
| Walking speed (m/s) | 0.73 ± 0.30 | 0.83 ± 0.20 | 0.089 |
| Normal, n (%) | 13 (21.1) | 8 (16.0) | 0.467 |
| Slow, n (%) | 44 (77.2) | 42 (84.0) | |
| Hypertension, n (%) | 47 (82.0) | 41 (82.0) | 1.000 |
| Hypercholesterolemia, n (%) | 6 (10.5) | 12 (24.0) | 0.074 |
| Hyperglyceridemia, n (%) | 7 (12.3) | 8 (16.0) | 0.591 |
| NSD (N = 57) | NE (N = 50) | |||||
|---|---|---|---|---|---|---|
| p-Value | p-Value | |||||
| Baseline | End | Baseline × End | Baseline | End | Baseline × End | |
| Body composition | ||||||
| BW (kg) | 53.73 ± 8.31 | 54.94 ± 8.50 | <0.001 | 62.91 ± 13.57 | 62.73 ± 12.67 | 0.574 |
| BMI (kg/m2) | 20.47 ± 3.03 | 20.97 ± 3.03 | <0.001 | 23.74 ± 4.30 | 23.67 ± 3.98 | 0.603 |
| Body fat (%) | 25.97 ± 5.92 | 26.58 ± 6.13 | 0.273 | 27.03 ± 5.08 | 27.43 ± 4.16 | 0.356 |
| Muscle mass (%) | 26.31 ± 3.03 | 26.15 ± 3.13 | 0.499 | 26.81 ± 2.81 | 26.49 ± 2.92 | 0.313 |
| ASMI (kg/m2) | 5.38 ± 0.95 | 5.46 ± 0.97 | 0.189 | 6.38 ± 1.38 | 6.30 ± 1.33 | 0.263 |
| Calf circumference (cm) | 31.98 ± 3.40 | 32.14 ± 3.01 | 0.842 | 32.95 ± 4.05 | 32.57 ± 3.91 | 0.065 |
| Physical performance | ||||||
| SOF | 0.98 ± 0.64 | 0.23 ± 0.42 | <0.001 | 0.50 ± 0.61 | 0.56 ± 0.58 | 0.180 |
| Grip strength (kg) | 21.66 ± 6.14 | 21.97 ± 6.21 | 0.481 | 21.64 ± 8.09 | 21.88 ± 7.74 | 0.621 |
| 6-m walking speed (s) | 10.02 ± 5.04 | 8.56 ± 4.79 | 0.001 | 7.71 ± 2.12 | 8.16 ± 2.89 | 0.111 |
| Walking speed (m/s) | 0.73 ± 0.30 | 0.89 ± 0.38 | <0.001 | 0.83 ± 0.20 | 0.83 ± 0.32 | 0.363 |
| Blood pressure | ||||||
| SBP (mmHg) | 133 ± 17 | 133 ± 15 | 0.857 | 132 ± 17 | 131 ± 14 | 0.251 |
| DBP (mmHg) | 78 ± 11 | 76 ± 8 | 0.079 | 77 ± 10 | 76 ± 9 | 0.574 |
| Nutritional status | ||||||
| MUST | ||||||
| 0, n (%) | 0 (0.0) | 34 (59.6) | <0.001 | 0 (0.0) | 2 (3.8) | 0.355 |
| 1, n (%) | 37 (64.9) | 12 (21.1) | 41 (78.8) | 40 (76.9) | ||
| 2, n (%) | 10 (17.5) | 9 (15.8) | 9 (17.3) | 8 (15.4) | ||
| 3, n (%) | 10 (17.5) | 2 (3.5) | 0 (0.0) | 0 (0.0) | ||
| MNA-SF | 9.07 ± 1.83 | 12.04 ± 1.31 | <0.001 | 10.66 ± 1.92 | 10.58 ± 1.93 | 0.773 |
| Total energy intake (kcal) | 1213.9 ± 69.53 | 1611.8 ± 71.21 | <0.001 | 1219.0 ± 67.68 | 1223.0 ± 59.08 | 0.417 |
| NSD (N = 57) | NE (N = 50) | NSD × NE | |
|---|---|---|---|
| Week12-Baseline | Week12-Baseline | p-Value | |
| Body composition | |||
| BW (kg) | 1.21 ± 1.83 | −0.17 ± 2.17 | <0.001 |
| BMI (kg/m2) | 0.5 ± 0.78 | −0.07 ± 0.88 | <0.001 |
| Body fat (%) | 0.62 ± 4.21 | 0.40 ± 3.06 | 0.783 |
| Muscle mass (%) | −0.16 ± 1.83 | −0.33 ± 2.26 | 0.685 |
| ASMI (kg/m2) | 0.09 ± 0.48 | −0.08 ± 0.54 | 0.016 |
| Calf circumference (cm) | 0.17 ± 2.77 | −0.39 ± 1.46 | 0.191 |
| Physical performance | |||
| SOF | −0.75 ± 0.69 | 0.06 ± 0.31 | <0.001 |
| Grip strength (kg) | 0.31 ± 3.34 | 0.19 ± 2.02 | 0.428 |
| 6-m walking speed (s) | −1.47 ± 3.23 | 0.45 ± 2.12 | 0.001 |
| Walking speed (m/s) | 0.15 ± 0.24 | 0.00 ± 0.29 | 0.004 |
| Nutritional status | |||
| Total energy intake (kcal) | 397.92 ± 29.90 | 4.00 ± 31.68 | <0.001 |
| MNA-SF | 2.96 ± 1.86 | −0.08 ± 1.28 | <0.001 |
| NSD | NE | NSD × NE | ||||||
|---|---|---|---|---|---|---|---|---|
| p-Value | p-Value | p-Value | ||||||
| Baseline | End | Baseline × End | Baseline | End | Baseline × End | Baseline | End | |
| 25-OH Vit. D (ng/mL) | ||||||||
| Deficiency (≤20 ng/mL), n (%) | 24 (42.1) | 23 (40.4) | 0.923 | 21 (42.0) | 21 (42.0) | 0.956 | 0.348 | 0.355 |
| Insufficiency (21~29.9 ng/mL), n (%) | 18 (31.6) | 20 (35.1) | 21 (42.0) | 22(44.0) | ||||
| Sufficiency (≥30 ng/mL), n (%) | 15 (26.3) | 14 (24.6) | 8 (16.0) | 7 (14.0) | ||||
| Zinc (μg/L) | ||||||||
| Deficiency (<700 μg/L), n (%) | 28 (49.1) | 23 (40.4) | 0.451 | 12 (24.0) | 23 (46.0) | 0.035 | 0.009 | 0.565 |
| Sufficiency (≥700 μg/L), n (%) | 29 (50.9) | 34 (59.6) | 38 (76.0) | 27 (54.0) | ||||
| 12th Week | β | p-Value | R2 |
|---|---|---|---|
| Body composition | |||
| BW (kg) | 0.041 | 0.030 | 0.971 |
| BMI (kg/m2) | 0.048 | 0.040 | 0.956 |
| Body fat (%) | 0.067 | 0.511 | 0.135 |
| Muscle mass (%) | 0.008 | 0.938 | 0.191 |
| ASMI (kg/m2) | 0.020 | 0.722 | 0.726 |
| Calf circumference (cm) | 0.253 | 0.002 | 0.476 |
| Physical performance | |||
| SOF | −0.326 | 0.002 | 0.080 |
| Grip strength (kg) | 0.160 | 0.090 | 0.258 |
| Walking speed (m/s) | 0.094 | 0.026 | 0.094 |
| Blood pressure | |||
| SBP (mmHg) | 0.034 | 0.755 | 0.003 |
| DBP (mmHg) | −0.079 | 0.472 | −0.003 |
| Nutritional status | |||
| MNA-SF | 0.705 | <0.001 | 0.512 |
| 12th Week | β | p-Value | R2 |
|---|---|---|---|
| Blood sugar (AC) (mg/dL) | 0.181 | 0.093 | 0.043 |
| Lipid profile | |||
| Cholesterol (mg/dL) | 0.041 | 0.698 | 0.055 |
| Triglycerides (mg/dL) | 0.034 | 0.741 | 0.104 |
| Kidney function | |||
| Uric acid (mg/dL) | −0.048 | 0.653 | 0.027 |
| Creatinine (mg/dL) | −0.157 | 0.154 | −0.014 |
| Liver function | |||
| AST (U/L) | 0.056 | 0.615 | −0.024 |
| ALT (U/L) | 0.175 | 0.103 | 0.039 |
| Nutritional status | |||
| Albumin (g/dL) | 0.247 | 0.014 | 0.178 |
| Vitamin (Vit.) D status | |||
| Total 25-OH Vit. D (ng/mL) | 0.159 | 0.140 | 0.035 |
| Zinc status | |||
| Zinc (μg/L) | 0.165 | 0.165 | 0.016 |
| Hematology | |||
| RBCs (106/μL) | 0.097 | 0.321 | 0.199 |
| WBCs (103/μL) | 0.148 | 0.180 | −0.011 |
| Hemoglobin (g/dL) | 0.166 | 0.087 | 0.222 |
| Hematocrit (%) | 0.136 | 0.159 | 0.222 |
| Platelets (103/μL) | 0.084 | 0.434 | 0.041 |
| MCH (pg) | 0.098 | 0.376 | −0.027 |
| MCHC (g/dL) | 0.186 | 0.087 | 0.020 |
| MCV (fL) | −0.025 | 0.698 | −0.025 |
| Neutrophil Seg. (%) | 0.072 | 0.517 | −0.022 |
| Lymphocytes (%) | −0.023 | 0.836 | −0.006 |
| Monocytes (%) | −0.011 | 0.955 | −0.011 |
| Eosinophils (%) | −0.250 | 0.022 | 0.030 |
| Basophils (%) | 0.002 | 0.985 | −0.014 |
| RDW-CV (%) | −0.006 | 0.957 | 0.015 |
| Crude | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| Adjusted | Adjusted | Adjusted | ||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Total 25-OH Vitamin D (ng/mL) | ||||||||
| Sufficiency (≥30 ng/mL) | 1 | 1 | 1 | 1 | ||||
| Insufficiency (20.1~29.9 ng/mL) | 0.455 | (0.153, 1.353) | 0.416 | (0.132, 1.315) | 0.374 | (0.108, 1.299) | 0.316 | (0.085, 1.174) |
| Deficiency (≤20 ng/mL) | 0.548 | (0.185, 1.618) | 0.446 | (0.141, 1.409) | 0.373 | (0.108, 1.284) | 0.369 | (0.101, 1.346) |
| Zinc (μg/L) | ||||||||
| Sufficiency (≥700 μg/L) | 1 | 1 | 1 | 1 | ||||
| Deficiency (<700 μg/L) | 0.794 | (0.369, 1.711) | 0.587 | (0.248, 1.391) | 0.429 | (0.165, 1.117) | 0.356 | (0.128, 0.990) |
| SOF | ||||||||
| Score = 0 | 1 | 1 | 1 | 1 | ||||
| Score ≥ 1 | 0.273 | (0.119, 0.626) | 0.301 | (0.126, 0.721) | 0.299 | (0.086, 0.612) | 0.192 | (0.067, 0.551) |
| MNA-SF | ||||||||
| Score 12~14 | 1 | 1 | 1 | 1 | ||||
| Score 6~11 | 0.381 | (0.174, 0.833) | 0.301 | (0.126, 0.721) | 0.076 | (0.020, 0.282) | 0.058 | (0.014, 0.250) |
| Calf circumference (cm) | ||||||||
| Normal | 1 | 1 | 1 | 1 | ||||
| Low calf circumference | 1.704 | (0.779, 3.727) | 2.213 | (0.906, 5.407) | 0.991 | (0.332, 2.957) | 0.793 | (0.248, 2.538) |
| Walking speed (m/s) | ||||||||
| ≥1.0 m/s | 1 | 1 | 1 | 1 | ||||
| <1.0 m/s | 0.262 | (0.104, 0.658) | 0.214 | (0.078, 0.591) | 0.089 | (0.022, 0.360) | 0.104 | (0.026, 0.426) |
| Hemoglobin (g/dL) | ||||||||
| Normal range | 1 | 1 | 1 | 1 | ||||
| Below normal range | 1.093 | (0.473, 2.528) | 0.936 | (0.358, 2.447) | 0.616 | (0.217, 1.744) | 0.739 | (0.250, 2.185) |
| ASMI (kg/m2) | ||||||||
| Normal | 1 | 1 | 1 | 1 | ||||
| Low ASMI | 7.846 | (2.853, 21.577) | 6.783 | (2.416, 19.040) | 3.703 | (1.067, 12.857) | 1.954 | (0.445, 8.581) |
| Grip strength (kg) | ||||||||
| Normal | 1 | 1 | 1 | 1 | ||||
| Low grip strength | 1.194 | (0.504, 2.831) | 0.905 | (0.358, 2.287) | 0.876 | (0.319, 2.406) | 0.727 | (0.249, 2.117) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Lee, C.-Y.; Chen, J.-R.; Ding, M.-Y.; Liang, F.-Q.; Yang, S.-C. Beneficial Effects of Oral Nutrition Supplements on the Nutritional Status and Physical Performance of Older Nursing Home Residents at Risk of Malnutrition. Nutrients 2023, 15, 4291. https://doi.org/10.3390/nu15194291
Chen Y-H, Lee C-Y, Chen J-R, Ding M-Y, Liang F-Q, Yang S-C. Beneficial Effects of Oral Nutrition Supplements on the Nutritional Status and Physical Performance of Older Nursing Home Residents at Risk of Malnutrition. Nutrients. 2023; 15(19):4291. https://doi.org/10.3390/nu15194291
Chicago/Turabian StyleChen, Yi-Hsiu, Che-Yu Lee, Jiun-Rong Chen, Min-Yu Ding, Feng-Qi Liang, and Suh-Ching Yang. 2023. "Beneficial Effects of Oral Nutrition Supplements on the Nutritional Status and Physical Performance of Older Nursing Home Residents at Risk of Malnutrition" Nutrients 15, no. 19: 4291. https://doi.org/10.3390/nu15194291
APA StyleChen, Y. -H., Lee, C. -Y., Chen, J. -R., Ding, M. -Y., Liang, F. -Q., & Yang, S. -C. (2023). Beneficial Effects of Oral Nutrition Supplements on the Nutritional Status and Physical Performance of Older Nursing Home Residents at Risk of Malnutrition. Nutrients, 15(19), 4291. https://doi.org/10.3390/nu15194291