
Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study
 , , , ,
, , , , 
Abstract
:
1. Introduction
2. Methods
2.1. Study Design and Ethical Issues
2.2. Settings, Participants, and Study Periods
2.3. Institutional Nutrition Protocol
2.4. Retrieved and Measured Variables
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
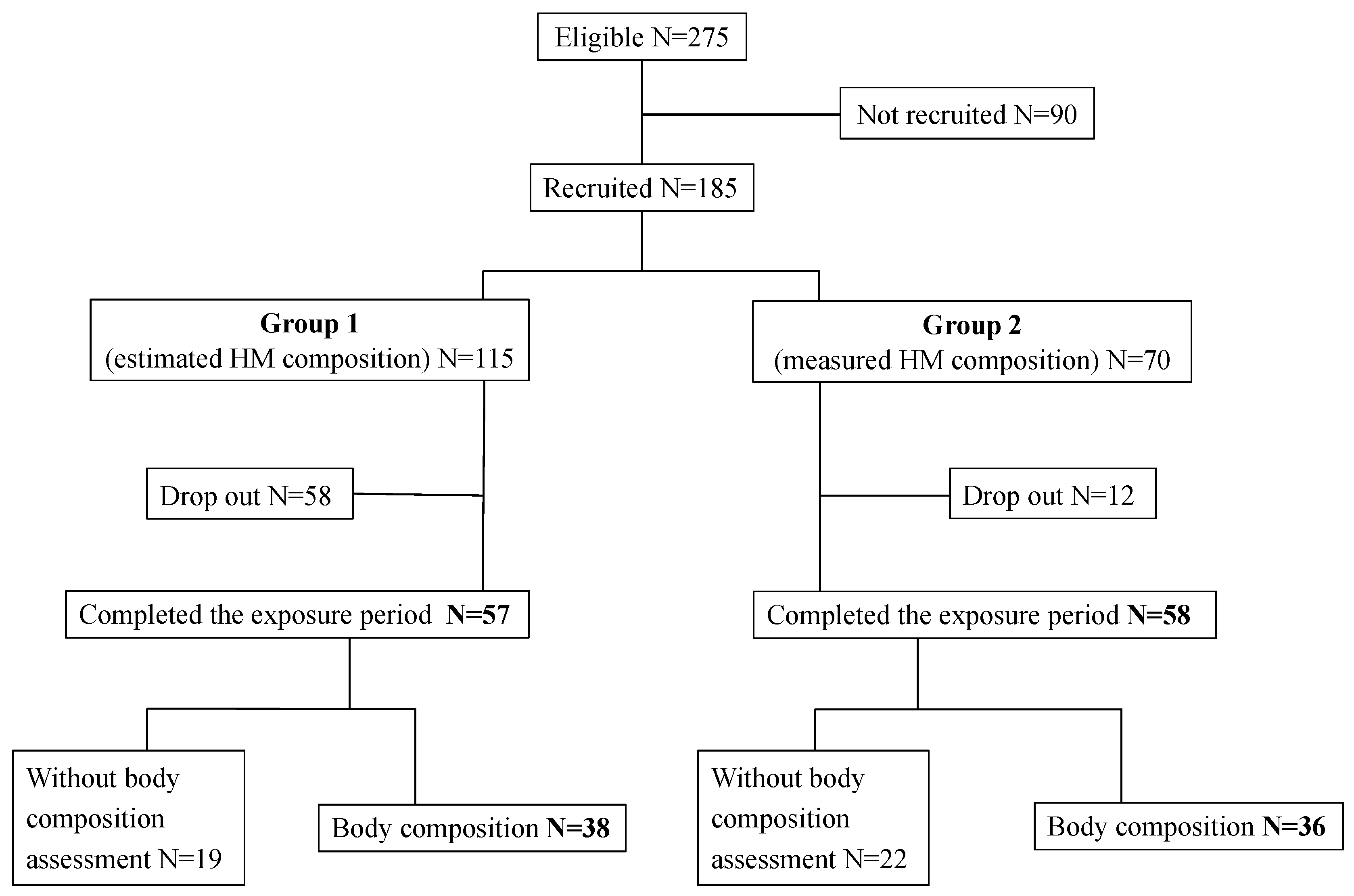
3.1. Study Flowchart
3.2. Characteristics of Infants Completing the Study
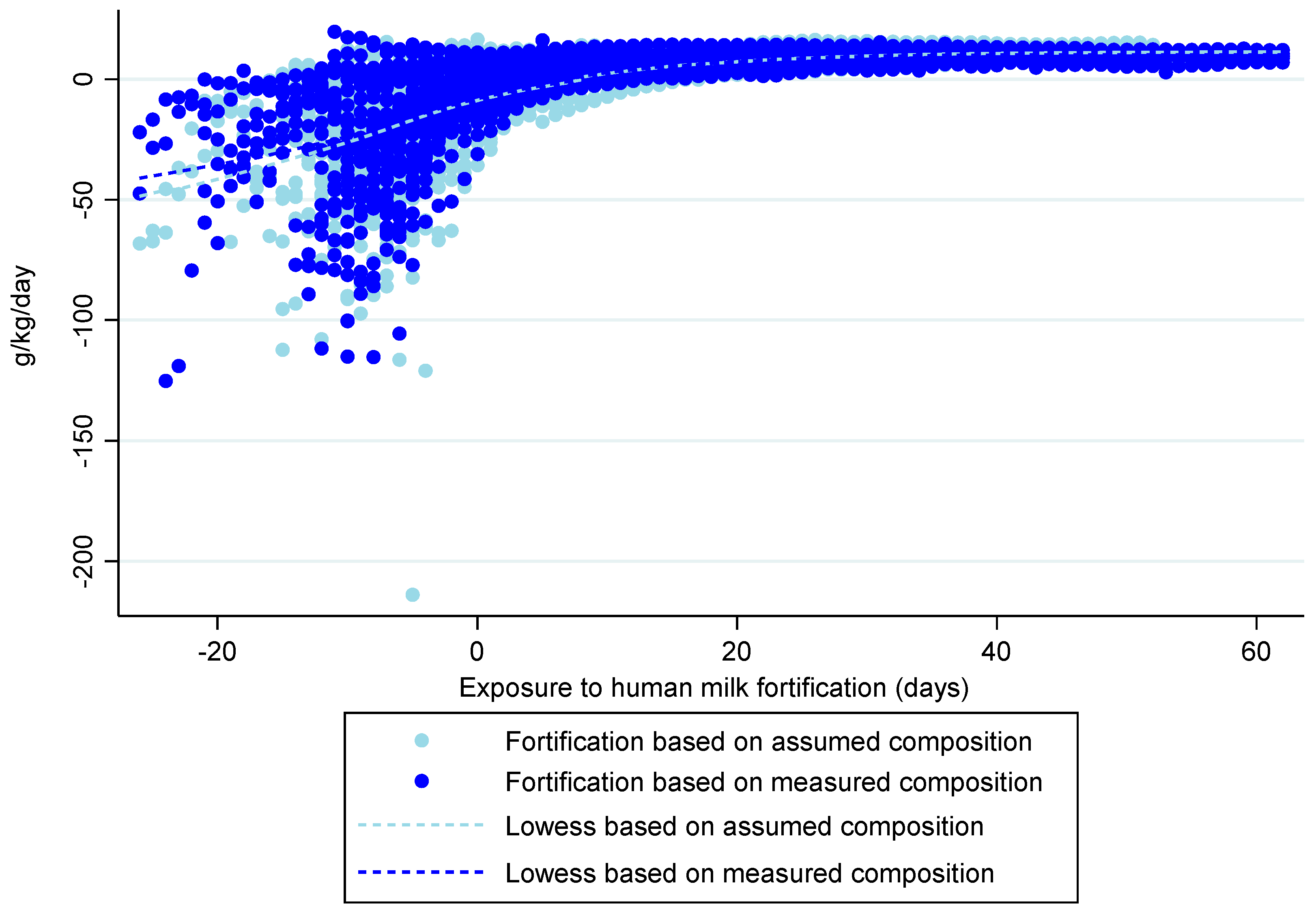
3.3. Nutritional Exposure
3.4. Anthropometry
3.4.1. Body Weight z-Score
3.4.2. Weight Gain Velocity
3.4.3. Length z-Score
3.4.4. Length Gain Velocity
3.4.5. Head Circumference z-Score
3.4.6. Head Circumference Gain Velocity
3.5. Body Composition
4. Discussion
4.1. Nutrient Intake According to the Fortification Method
4.2. Body Weight Gain
4.3. Linear Growth
4.4. Head Growth
4.5. Body Composition
4.6. Limitations
4.7. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| %FFM | Percentage fat-free mass |
| %FM | Percentage fat mass |
| DHM | Donor human milk |
| ESPGHAN | European Society for Paediatric Gastroenterology Hepatology and Nutrition |
| FFM | Fat-free mass |
| FM | Fat mass |
| FMI | Fat mass index |
| HM | Human milk |
| HC | Head circumference |
| IQR | Interquartile range |
| LOS | Late-onset sepsis |
| MCT | Mid-chain triglyceride |
| MOM | Mother’s own milk |
| NEC | Necrotizing enterocolitis |
| PER | Protein-to-energy ratio |
| PMA | Postmenstrual age |
| SD | Standard deviation |
| SNAPE II | Score for Neonatal Acute Physiology with Perinatal Extension-II |
| TEA | Term-equivalent age |
References
- Dutta, S.; Singh, B.; Chessell, L.; Wilson, J.; Janes, M.; McDonald, K.; Shahid, S.; Gardner, V.A.; Hjartarson, A.; Purcha, M.; et al. Guidelines for feeding very low birth weight infants. Nutrients 2015, 7, 423–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of human milk for preterm infants: Update and recommendations of the European milk bank association (EMBA) working group on human milk fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- Wagner, C.L.; Taylor, S.N.; Johnson, D. Host factors in amniotic fluid and breast milk that contribute to gut maturation. Clin. Rev. Allergy Immunol. 2008, 34, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Loui, A.; Eilers, E.; Strauss, E.; Pohl-Schickinger, A.; Obladen, M.; Koehne, P. Vascular endothelial growth factor (VEGF) and soluble VEGF receptor 1 (sFlt-1) levels in early and mature human milk from mothers of preterm versus term infants. J. Hum. Lact. 2012, 28, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Lewis, E.D.; Richard, C.; Larsen, B.M.; Field, C.J. The importance of human milk for immunity in preterm infants. Clin. Perinatol. 2017, 44, 23–47. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Dusick, A.M.; Vohr, B.R.; Wright, L.L.; Wrage, L.A.; Poole, W.K. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics 2006, 117, 1253–1261. [Google Scholar] [CrossRef] [Green Version]
- Tozzi, M.G.; Moscuzza, F.; Michelucci, A.; Lorenzoni, F.; Cosini, C.; Ciantelli, M.; Ghirri, P. ExtraUterine Growth Restriction (EUGR) in preterm infants: Growth patterns, nutrition, and epigenetic markers. A pilot study. Front. Pediatr. 2018, 6, 408. [Google Scholar] [CrossRef]
- Ziegler, E.E. Meeting the nutritional needs of the low-birth-weight infant. Ann. Nutr. Metab. 2011, 58, 8–18. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Zapanta, B.; Ali, A.; Barui, S.; Fusch, C. Target fortification of breast milk: How often should milk analysis be done? Nutrients 2015, 7, 2297–2310. [Google Scholar] [CrossRef] [Green Version]
- Radmacher, P.G.; Adamkin, D.H. Fortification of human milk for preterm infants. Semin. Fetal Neonatal Med. 2017, 22, 30–35. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Sun, R.; Maillart, L.; Schaefer, A.; Spence, E.H.; Perrin, M.T. Macronutrient variability in human milk from donors to a milk bank: Implications for feeding preterm infants. PLoS ONE 2019, 14, e0210610. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; et al. Target fortification of breast milk with fat, protein, and carbohydrates for preterm infants. J. Pediatr. 2013, 163, 1001–1007. [Google Scholar] [CrossRef]
- Faienza, M.F.; D’Amato, E.; Natale, M.P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic bone disease of prematurity: Diagnosis and management. Front. Pediatr. 2019, 7, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabrizio, V.; Trzaski, J.M.; Brownell, E.A.; Esposito, P.; Lainwala, S.; Lussier, M.M.; Hagadorn, J.I. Individualized versus standard diet fortification for growth and development in preterm infants receiving human milk. Cochrane Database Syst. Rev. 2020, 11, 1–64. [Google Scholar] [CrossRef]
- Morlacchi, L.; Mallardi, D.; Giannì, M.L.; Roggero, P.; Amato, O.; Piemontese, P.; Consonni, D.; Mosca, F. Is targeted fortification of human breast milk an optimal nutrition strategy for preterm infants? An interventional study. J. Transl. Med. 2016, 14, 195. [Google Scholar] [CrossRef] [Green Version]
- Quan, M.; Wang, D.; Gou, L.; Sun, Z.; Ma, J.; Zhang, L.; Wang, C.; Schibler, K.; Li, Z. Individualized Human Milk Fortification to improve the growth of hospitalized preterm infants. Nutr. Clin. Pract. 2020, 35, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Rochow, N.; Fusch, G.; Ali, A.; Bhatia, A.; So, H.Y.; Iskander, R.; Chessell, L.; Helou, S.E.; Fusch, C. Individualized target fortification of breast milk with protein, carbohydrates, and fat for preterm infants: A double-blind randomized controlled trial. Clin. Nutr. 2021, 40, 54–63. [Google Scholar] [CrossRef]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Johnson, M.J.; Wootton, S.A.; Leaf, A.A.; Jackson, A.A. Preterm birth and body composition at term equivalent age: A systematic review and meta-analysis. Pediatrics 2012, 130, e640–e649. [Google Scholar] [CrossRef] [Green Version]
- Bruckner, M.; Khan, Z.; Binder, C.; Morris, N.; Windisch, B.; Holasek, S.; Urlesberger, B. Extremely preterm infants have a higher fat mass percentage in comparison to very preterm infants at term-equivalent age. Front. Pediatr. 2020, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Hamatschek, C.; Yousuf, E.I.; Möllers, L.S.; So, H.Y.; Morrison, K.M.; Fusch, C.; Rochow, N. Fat and fat-free mass of preterm and term infants from birth to six months: A review of current evidence. Nutrients 2020, 12, 288. [Google Scholar] [CrossRef] [Green Version]
- Piemontese, P.; Liotto, N.; Mallardi, D.; Roggero, P.; Puricelli, V.; Giannì, M.L.; Morniroli, D.; Tabasso, C.; Perrone, M.; Menis, C.; et al. The effect of human milk on modulating the quality of growth in preterm infants. Front. Pediatr. 2018, 6, 291. [Google Scholar] [CrossRef]
- Cerasani, J.; Ceroni, F.; de Cosmi, V.; Mazzocchi, A.; Morniroli, D.; Roggero, P.; Mosca, F.; Agostoni, C.; Giannì, M.L. Human milk feeding and preterm infants’ growth and body composition: A literature review. Nutrients 2020, 12, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şimşek, G.K.; Dizdar, E.A.; Arayıcı, S.; Canpolat, F.E.; Sari, F.N.; Uras, N.; Oguz, S.S. Comparison of the effect of three different fortification methods on growth of very low birth weight infants. Breastfeed. Med. 2019, 14, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Minarski, M.; Maas, C.; Engel, C.; Heinrich, C.; Böckmann, K.; Bernhard, W.; Poets, C.F.; Franz, A.R. Calculating protein content of expressed breast milk to optimize protein supplementation in very low birth weight infants with minimal effort—A secondary analysis. Nutrients 2020, 12, 1231. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.T.; Schroder, P.E.; Poindexter, B.B. Macronutrient analysis of target-pooled donor breast milk and corresponding growth in very low birth weight infants. Nutrients 2019, 11, 1884. [Google Scholar] [CrossRef] [Green Version]
- McLeod, G.; Sherriff, J.; Hartmann, P.E.; Nathan, E.; Geddes, D.; Simmer, K. Comparing different methods of human breast milk fortification using measured v. assumed macronutrient composition to target reference growth a randomised controlled trial. Br. J. Nutr. 2016, 115, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Sánchez Luna, M.; Martin, S.C.; Gómez-de-Orgaz, C.S. Human milk bank and personalized nutrition in the NICU: A narrative review. Eur. J. Pediatr. 2021, 180, 1327–1333. [Google Scholar] [CrossRef]
- Strydom, K.; van Niekerk, E.; Dhansay, M.A. Factors affecting body composition in preterm infants: Assessment techniques and nutritional interventions. Pediatr. Neonatol. 2019, 60, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Andrews, E.T.; Beattie, R.M.; Johnson, M.J. Measuring body composition in the preterm infant: Evidence base and practicalities. Clin. Nutr. 2019, 38, 2521–2530. [Google Scholar] [CrossRef]
- Macedo, I.; Pereira-da-Silva, L.; Cardoso, M. The fortification method relying on assumed human milk composition overestimates the actual energy and macronutrient intakes in very preterm infants. Matern. Health Neonatol. Perinatol. 2018, 4, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macedo, I.; Pereira-da-Silva, L.; Cardoso, M. Associations of measured protein and energy intakes with growth and adiposity in human milk-fed preterm infants at term postmenstrual age: A cohort study. Am. J. Perinatol. 2018, 35, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.; Virella, D.; Macedo, I.; Silva, D.; Pereira-da-silva, L. Customized human milk fortification based on measured human milk composition to improve the quality of growth in very preterm infants: A mixed-cohort study protocol. Int. J. Environ. Res. Public. Health 2021, 18, 823. [Google Scholar] [CrossRef] [PubMed]
- Mimouni, F.B.; Lubetzky, R.; Yochpaz, S.; Mandel, D. Preterm human milk macronutrient and energy composition: A systematic review and meta-analysis. Clin. Perinatol. 2017, 44, 165–172. [Google Scholar] [CrossRef]
- Pereira-da-Silva, L.; Gomes, A.; Macedo, I.; Alexandrino, A.M.; Pissarra, S.; Cardoso, M. Nutrição entérica na criança nascida pré-termo: Revisão do Consenso Nacional. Acta Pediatr. Port. 2014, 45, 326–339. [Google Scholar]
- Mihatsch, W.; Shamir, R.; van Goudoever, J.B.; Fewtrell, M.; Lapillonne, A.; Lohner, S.; Mihályi, K.; Decsi, T. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Guideline development process for the updated guidelines. Clin. Nutr. 2018, 37, 2306–2308. [Google Scholar] [CrossRef] [Green Version]
- Pereira-da-silva, L.; Pissarra, S.; Alexandrino, A.M.; Malheiro, L.; Macedo, I.; Cardoso, M.; Silva, P.V.; Frutuoso, S.P.; Lau, H.; Soares, T. Guidelines for neonatal parenteral nutrition: 2019 update by the Portuguese Neonatal Society. Part I. General aspects, energy, and macronutrients. Port. J. Pediatr. 2019, 50, 209–219. [Google Scholar] [CrossRef]
- Pereira-da-Silva, L.; Pissarra, S.; Alexandrino, A.M.; Malheiro, L.; Macedo, I.; Cardoso, M.; Silva, P.V.; Frutuoso, S.P.; Lau, H.; Soares, T. Guidelines for neonatal parenteral nutrition: 2019 update by the Portuguese Neonatal Society. Part II. Micronutrients, ready-to-use solutions and particular conditions. Port. J. Pediatr. 2019, 50, 220–231. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.K.; Corcoran, J.D.; Escobar, G.J.; Lee, S.K. SNAP-II and SNAPPE-II: Simplified newborn illness severity and mortality risk scores. J. Pediatr. 2001, 138, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Modi, N.; Doré, C.J.; Saraswatula, A.; Richards, M.; Bamford, K.B.; Coello, R.; Holmes, A. A case definition for national and international neonatal bloodstream infection surveillance. Arch. Dis. Child.-Fetal Neonatal. Ed. 2009, 94, F8–F12. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.C.; Kliegman, R.M. Necrotizing enterocolitis: Treatment based on staging criteria. Pediatr. Clin. N. Am. 1986, 33, 179–201. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef] [PubMed]
- de Vries, L.S.; Eken, P.; Pierrat, V.; Daniels, H.; Casaer, P. Prediction of neurodevelopmental outcome in the preterm infant: Short latency cortical somatosensory evoked potentials compared with cranial ultrasound. Arch. Dis. Child. 1992, 67, 1177–1181. [Google Scholar] [CrossRef] [Green Version]
- Bancalari, E.; Claure, N. Definitions and diagnostic criteria for bronchopulmonary dysplasia. Semin. Perinatol. 2006, 30, 164–170. [Google Scholar] [CrossRef]
- Czosnykowska-łukacka, M.; Królak-Olejnik, B.; Orczyk-Pawiłowicz, M. Breast milk macronutrient components in prolonged lactation. Nutrients 2018, 10, 1893. [Google Scholar] [CrossRef] [Green Version]
- Pereira-da-Silva, L.; Virella, D.; Fusch, C. Nutritional assessment in preterm infants: A Practical Approach in the NICU. Nutrients 2019, 11, 1999. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Jegier, B.J.; Kimura, R.E. Calculating postnatal growth velocity in very low birth weight (VLBW) premature infants. J. Perinatol. 2009, 29, 618–622. [Google Scholar] [CrossRef] [Green Version]
- Goswami, I.; Rochow, N.; Fusch, G.; Liu, K.; Marrin, M.L.; Heckmann, M.; Nelle, M.; Fusch, C. Length normalized indices for fat mass and fat-free mass in preterm and term infants during the first six months of life. Nutrients 2016, 8, 417. [Google Scholar] [CrossRef] [Green Version]
- Norris, T.; Ramel, S.E.; Catalano, P.; Caoimh, C.N.; Roggero, P.; Murray, D.; Fields, D.A.; Demerath, E.W.; Johnson, W. New charts for the assessment of body composition, according to air-displacement plethysmography, at birth and across the first 6 mo of life. Am. J. Clin. Nutr. 2019, 109, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- de Halleux, V.; Rigo, J. Variability in human milk composition: Benefit of individualized fortification in very-low-birth-weight infants. Am. J. Clin. Nutr. 2013, 98, 529S–535S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parat, S.; Raza, P.; Kamleh, M.; Super, D.; Groh-Wargo, S. Targeted breast milk fortification for very low birth weight (VLBW) infants: Nutritional intake, growth outcome and body composition. Nutrients 2020, 12, 1156. [Google Scholar] [CrossRef] [Green Version]
- Fusch, S.; Fusch, G.; Yousuf, E.I.; Rochow, M.; So, H.Y.; Fusch, C.; Rochow, N. Individualized target fortification of breast milk: Optimizing macronutrient content using different fortifiers and approaches. Front. Nutr. 2021, 8, 652641. [Google Scholar] [CrossRef]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Jacobelli, S.; et al. Enteral nutrition in preterm infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and invited experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef]
- Goldberg, D.L.; Becker, P.J.; Brigham, K.; Carlson, S.; Fleck, L.; Gollins, L.; Sandrock, M.; Fullmer, M.; Van Poots, H.A. Identifying malnutrition in preterm and neonatal populations: Recommended indicators. J. Acad. Nutr. Diet. 2018, 118, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Koo, W.W.; Walters, J.C.; Hockman, E.M. Body composition in human infants at birth and postnatally. J. Nutr. 2000, 130, 2188–2194. [Google Scholar] [CrossRef] [Green Version]
- Rochow, N.; Landau-Crangle, E.; So, H.Y.; Pelc, A.; Fusch, G.; Däbritz, J.; Göpel, W.; Fusch, C. Z-score differences based on cross-sectional growth charts do not reflect the growth rate of very low birth weight infants. PLoS ONE 2019, 14, e0216048. [Google Scholar] [CrossRef] [Green Version]
- Fenton, T.R.; Dai, S.; Lalari, V.; Alshaikh, B. Neonatal and preterm infant growth assessment. Clin. Perinatol. 2022, 49, 295–311. [Google Scholar] [CrossRef]
- Fenton, T.R.; Griffin, I.J.; Hoyos, A.; Groh-Wargo, S.; Anderson, D.; Ehrenkrank, R.A.; Senterre, T. Accuracy of preterm infant weight gain velocity calculations vary depending on method used and infant age at time of measurement. Pediatr. Res. 2019, 85, 650–654. [Google Scholar] [CrossRef]
- Fenton, T.R.; Senterre, T.; Griffin, I.J. Time interval for preterm infant weight gain velocity calculation precision. Arch. Dis. Child.-Fetal Neonatal Ed. 2018, 104, F218–F219. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Anderson, D.; Groh-Wargo, S.; Hoyos, A.; Ehrenkranz, R.A.; Senterre, T. An attempt to standardize the calculation of growth velocity of preterm infants—evaluation of practical bedside methods. J. Pediatr. 2018, 196, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Zozaya, C.; Avila-Alvarez, A.; Arruza, L.; Rodrigo, F.G.M.; Fernandez-Perez, C.; Castro, A.; Cuesta, M.T.; Vacas, B.; Couce, M.L.; Torres, M.V.; et al. The effect of morbidity and sex on postnatal growth of very preterm infants: A multicenter cohort study. Neonatology 2019, 115, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Senterre, T.; Rigo, J. Reduction in postnatal cumulative nutritional deficit and improvement of growth in extremely preterm infants. Acta Paediatr. Int. J. Paediatr. 2012, 101, e64–e70. [Google Scholar] [CrossRef]
- Cheong, J.L.Y.; Hunt, R.W.; Anderson, P.J.; Howard, K.; Thompson, D.K.; Wang, H.X.; Bear, M.J.; Inder, T.E.; Doyle, L.W. Head growth in preterm infants: Correlation with magnetic resonance imaging and neurodevelopmental outcome. Pediatrics 2008, 121, e1534–e1540. [Google Scholar] [CrossRef]
- Bell, K.A.; Matthews, L.G.; Cherkerzian, S.; Prohl, A.K.; Warfield, S.K.; Inder, T.E.; Onishi, S.; Belfort, M.B. Associations of body composition with regional brain volumes and white matter microstructure in very preterm infants. Arch. Dis. Child.-Fetal Neonatal Ed. 2022, 107, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Binder, C.; Buchmayer, J.; Thajer, A.; Giordano, V.; Schmidbauer, V.; Harreiter, K.; Klebermass-Schrehof, K.; Berger, A.; Goeral, K. Association between fat-free mass and brain size in extremely preterm infants. Nutrients 2021, 13, 4205. [Google Scholar] [CrossRef]
- Lingwood, B.E.; Al-Theyab, N.; Eiby, Y.A.; Colditz, P.B.; Donovan, T.J. Body composition in very preterm infants before discharge is associated with macronutrient intake. Br. J. Nutr. 2020, 123, 800–806. [Google Scholar] [CrossRef]
- Al-Theyab, N.A.; Donovan, T.J.; Eiby, Y.A.; Colditz, P.B.; Lingwood, B.E. Fat trajectory after birth in very preterm infants mimics healthy term infants. Pediatr. Obes. 2019, 14, e12472. [Google Scholar] [CrossRef]
- Casirati, A.; Somaschini, A.; Perrone, M.; Vandoni, G.; Sebastiani, F.; Montagna, E.; Somaschini, M.; Caccialanza, R. Preterm birth and metabolic implications on later life: A narrative review focused on body composition. Front. Nutr. 2022, 9, 2151. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 |
|---|---|
|
|
|
| Group 1 | Group 2 | p-Value | |
|---|---|---|---|
| n = 57 | n = 58 | ||
| Gestational age in weeks, mean (SD) | 29.6 (1.99) | 29.7 (2.31) | 0.850 |
| Females, n (%) | 27 (47.4) | 23 (39.7) | 0.412 |
| Twins, n (%) | 15 (26.3) | 24 (41.4) | 0.047 |
| Extremely preterm, n (%) | 14 (24.6) | 12 (20.7) | 0.314 |
| Prenatal steroids, n (%) | 55 (96.5) | 53 (91.4) | 0.286 |
| Birth weight z-score, mean (SD) | −0.11 (0.70) | −0.19 (0.66) | 0.691 |
| Birth length z-score, mean (SD) | −0.48 (0.512) | −1.07 (0.740) | 0.001 |
| Birth HC z-score, mean (SD) | −0.83 (0.90) | −1.60 (0.778) | <0.001 |
| Postnatal steroids, n (%) | 1 (1.8) | 4 (6.9) | 0.102 |
| Severity risk (SNAPPE II), median (P25; P75) | 10 (0.22) | 10 (0.27) | 0.785 |
| Late-onset sepsis, n (%) | 12 (21.1) | 25 (43.1) | 0.001 |
| Necrotizing enterocolitis III, n (%) | 0 | 0 | - |
| Intraventricular hemorrhage I, n (%) | 2 (3.5) | 0 | 0.128 |
| Bronchopulmonary dysplasia, n (%) | 4 (7.0) | 6 (10.3) | 0.264 |
| Recommended [19] | Group 1 | Group 2 | p-Value | |
|---|---|---|---|---|
| n = 57 | n = 58 | |||
| Total energy intake, kcal/kg/d; mean (SD) | 110–135 kcal/kg/d | 121.3 (25.3) | 127.9 (17.4) | <0.001 |
| Protein intake, g/kg/d; median (P25; P75) | All | 4.2 (3.7; 4.7) | 4.1 (3.7; 4.6) | 0.109 |
| <1 kg body weight: 4.0–4.5 g/kg/d | 3.9 (3.2;4.8) | 4.1 (3.3; 4.9) | 0.162 | |
| 1–1.8 kg body weight: 3.5–4.0 g/kg/d | 4.2 (3.8; 4.6) | 4.1 (3.8; 4.5) | 0.004 | |
| PER intake, g/100 kcal; median (P25; P75) | All | 3.5 (3.2; 3.9) | 3.4 (3.0; 3.8) | 0.001 |
| <1 kg body weight: 3.6–4.1 | 3.5 (3.2; 4.0) | 3.3 (3.0; 3.7) | <0.001 | |
| 1–1.8 kg body weight: 3.2–3.6 | 3.4 (3.2; 3.8) | 3.5 (3.1; 3.9) | 0.315 | |
| Fat intake, g/kg/d; mean (SD) | 4.8–6.6 g/kg/d | 5.5 (1.54) | 6.7 (1.67) | <0.001 |
| Carbohydrate intake, g/kg/d; mean (SD) | 11.6–13.2 g/kg/d | 11.9 (1.93) | 13.0 (1.90) | <0.001 |
| Group 1 | Group 2 | p-Value | |
|---|---|---|---|
| n = 57 | n = 58 | ||
| Body weight z-score at discharge, mean (SD) | −1.73 (0.92) | −1.73 (0.870) | 0.693 |
| Δ body weight z-score, median (P25; P75) | −1.64 (−1.99; −1.28) | −1.47 (−1.79; −1.10) | 0.565 |
| Length z-score at discharge, median (perc. 25; perc. 75) | −1.47 (−1.685; −0.970) † | −1.49 (−2.135; −0.830) | 0.744 |
| Δ length z-score, median (P25; P75) | −0.71 (−1.69; −0.37) † | −0.27 (−2.14; −0.04) | 0.005 |
| HC z-score at discharge, median (P25; P75) | −1.17 (−1.70; −0.63) † | −0.80 (−1.390; −0.02) | 0.102 |
| Δ HC z-score, median (P25; P75) | −0.31 (−0.59; 0.04) † | 0.75 (0.41; 1.17) | <0.001 |
| Group 1 | Group 2 | p-Value | |
|---|---|---|---|
| n = 38 | n = 36 | ||
| FM (g), median (P25; P75) | 360.1 (260.0; 483.3) | 269.5 (169.1; 413.9) | 0.026 |
| FFM (g), median (P25; P75) | 2155.8 (1854.8; 2529.8) | 2034.9 (1834.5; 2253.4) | 0.173 |
| %FM, median (P25; P75) | 14.5 (12.2; 17.3) | 12.6 (8.3; 14.9) | 0.021 |
| FMI, median (P25; P75) | 1.8 (1.4; 2.3) | 1.4 (0.9; 1.8) | 0.004 |
| %FFM, median (P25; P75) | 85.5 (82.7; 87.6) | 87.4 (85.1; 91.0) | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, M.; Virella, D.; Papoila, A.L.; Alves, M.; Macedo, I.; e Silva, D.; Pereira-da-Silva, L. Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study. Nutrients 2023, 15, 1533. https://doi.org/10.3390/nu15061533
Cardoso M, Virella D, Papoila AL, Alves M, Macedo I, e Silva D, Pereira-da-Silva L. Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study. Nutrients. 2023; 15(6):1533. https://doi.org/10.3390/nu15061533
Chicago/Turabian StyleCardoso, Manuela, Daniel Virella, Ana Luísa Papoila, Marta Alves, Israel Macedo, Diana e Silva, and Luís Pereira-da-Silva. 2023. "Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study" Nutrients 15, no. 6: 1533. https://doi.org/10.3390/nu15061533
APA StyleCardoso, M., Virella, D., Papoila, A. L., Alves, M., Macedo, I., e Silva, D., & Pereira-da-Silva, L. (2023). Individualized Fortification Based on Measured Macronutrient Content of Human Milk Improves Growth and Body Composition in Infants Born Less than 33 Weeks: A Mixed-Cohort Study. Nutrients, 15(6), 1533. https://doi.org/10.3390/nu15061533