
Maternal Serum Vitamin B12 during Pregnancy and Offspring Autism Spectrum Disorder

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Nationwide Registers
2.2. Finnish Maternity Cohort
2.3. Information on Cases and Controls
2.4. Maternal Vitamin B12 Measurement
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Gardener, H.; Spiegelman, D.; Buka, S.L. Prenatal Risk Factors for Autism: Comprehensive Meta-Analysis. Br. J. Psychiatry 2009, 195, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The Changing Epidemiology of Autism Spectrum Disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [PubMed]
- Friel, C.; Leyland, A.H.; Anderson, J.J.; Havdahl, A.; Borge, T.; Shimonovich, M.; Dundas, R. Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2558. [Google Scholar] [CrossRef]
- Li, M.; Francis, E.; Hinkle, S.N.; Ajjarapu, A.S.; Zhang, C. Preconception and Prenatal Nutrition and Neurodevelopmental Disorders: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1628. [Google Scholar] [CrossRef] [PubMed]
- Sourander, A.; Upadhyaya, S.; Surcel, H.-M.; Hinkka-Yli-Salomäki, S.; Cheslack-Postava, K.; Silwal, S.; Sucksdorff, M.; McKeague, I.W.; Brown, A.S. Maternal Vitamin D Levels During Pregnancy and Offspring Autism Spectrum Disorder. Biol. Psychiatry 2021, 90, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Pepper, M.R.; Black, M.M. B12 in Fetal Development. Semin. Cell Dev. Biol. 2011, 22, 619–623. [Google Scholar] [CrossRef]
- Scott, J.M.; Molloy, A.M. The Discovery of Vitamin B. Ann. Nutr. Metab. 2012, 61, 239–245. [Google Scholar] [CrossRef]
- King, J.C. A Summary of Pathways or Mechanisms Linking Preconception Maternal Nutrition with Birth Outcomes. J. Nutr. 2016, 146, 1437S–1444S. [Google Scholar] [CrossRef]
- Lövblad, K.-O.; Ramelli, G.; Remonda, L.; Nirkko, A.C.; Ozdoba, C.; Schroth, G. Retardation of Myelination Due to Dietary Vitamin B12 Deficiency: Cranial MRI Findings. Pediatr. Radiol. 1997, 27, 155–158. [Google Scholar] [CrossRef]
- Craciunescu, C.N.; Brown, E.C.; Mar, M.-H.; Albright, C.D.; Nadeau, M.R.; Zeisel, S.H. Folic Acid Deficiency During Late Gestation Decreases Progenitor Cell Proliferation and Increases Apoptosis in Fetal Mouse Brain. J. Nutr. 2004, 134, 162–166. [Google Scholar] [CrossRef]
- Barua, S.; Kuizon, S.; Brown, W.T.; Junaid, M.A. DNA Methylation Profiling at Single-Base Resolution Reveals Gestational Folic Acid Supplementation Influences the Epigenome of Mouse Offspring Cerebellum. Front. Neurosci. 2016, 10, 168. [Google Scholar] [CrossRef]
- Mahajan, A.; Sapehia, D.; Thakur, S.; Mohanraj, P.S.; Bagga, R.; Kaur, J. Effect of Imbalance in Folate and Vitamin B12 in Maternal/Parental Diet on Global Methylation and Regulatory MiRNAs. Sci. Rep. 2019, 9, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Mahajan, A.; Sapehia, D.; Kaur, J.; Sandhir, R. Effects of Altered Maternal Folate and Vitamin B12 on Neurobehavioral Outcomes in F1 Male Mice. Brain Res. Bull. 2019, 153, 93–101. [Google Scholar] [CrossRef]
- Troen, A.M.; Shea-Budgell, M.; Shukitt-Hale, B.; Smith, D.E.; Selhub, J.; Rosenberg, I.H. B-Vitamin Deficiency Causes Hyperhomocysteinemia and Vascular Cognitive Impairment in Mice. Proc. Natl. Acad. Sci. USA 2008, 105, 12474–12479. [Google Scholar] [CrossRef]
- del Río Garcia, C.; Torres-Sánchez, L.; Chen, J.; Schnaas, L.; Hernández, C.; Osorio, E.; Portillo, M.G.; López-Carrillo, L. Maternal MTHFR 677C>T Genotype and Dietary Intake of Folate and Vitamin B (12): Their Impact on Child Neurodevelopment. Nutr. Neurosci. 2009, 12, 13–20. [Google Scholar] [CrossRef]
- Bhate, V.; Deshpande, S.; Bhat, D.; Joshi, N.; Ladkat, R.; Watve, S.; Fall, C.; de Jager, C.A.; Refsum, H.; Yajnik, C. Vitamin B 12 Status of Pregnant Indian Women and Cognitive Function in Their 9-Year-Old Children. Food Nutr. Bull. 2008, 29, 249–254. [Google Scholar] [CrossRef]
- Lai, J.S.; Mohamad Ayob, M.N.; Cai, S.; Quah, P.L.; Gluckman, P.D.; Shek, L.P.; Yap, F.; Tan, K.H.; Chong, Y.S.; Godfrey, K.M.; et al. Maternal Plasma Vitamin B12 Concentrations during Pregnancy and Infant Cognitive Outcomes at 2 Years of Age. Br. J. Nutr. 2019, 121, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Torsvik, I.; Ueland, P.M.; Markestad, T.; Bjørke-Monsen, A.-L. Cobalamin Supplementation Improves Motor Development and Regurgitations in Infants: Results from a Randomized Intervention Study. Am. J. Clin. Nutr. 2013, 98, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Rogne, T.; Tielemans, M.J.; Chong, M.F.-F.; Yajnik, C.S.; Krishnaveni, G.V.; Poston, L.; Jaddoe, V.W.V.; Steegers, E.A.P.; Joshi, S.; Chong, Y.-S.; et al. Associations of Maternal Vitamin B12 Concentration in Pregnancy With the Risks of Preterm Birth and Low Birth Weight: A Systematic Review and Meta-Analysis of Individual Participant Data. Am. J. Epidemiol. 2017, 185, 212–223. [Google Scholar] [CrossRef]
- Yajnik, C.S.; Deshpande, S.S.; Jackson, A.A.; Refsum, H.; Rao, S.; Fisher, D.J.; Bhat, D.S.; Naik, S.S.; Coyaji, K.J.; Joglekar, C.V.; et al. Vitamin B12 and Folate Concentrations during Pregnancy and Insulin Resistance in the Offspring: The Pune Maternal Nutrition Study. Diabetologia 2008, 51, 29–38. [Google Scholar] [CrossRef]
- Raghavan, R.; Riley, A.W.; Volk, H.; Caruso, D.; Hironaka, L.; Sices, L.; Hong, X.; Wang, G.; Ji, Y.; Brucato, M.; et al. Maternal Multivitamin Intake, Plasma Folate and Vitamin B12 Levels and Autism Spectrum Disorder Risk in Offspring. Paediatr. Perinat. Epidemiol. 2018, 32, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Froehlich, T.; Kalkbrenner, A.; Pfeiffer, C.M.; Fazili, Z.; Yolton, K.; Lanphear, B.P. Are Autistic-Behaviors in Children Related to Prenatal Vitamin Use and Maternal Whole Blood Folate Concentrations? J. Autism. Dev. Disord. 2014, 44, 2602–2607. [Google Scholar] [CrossRef]
- Egorova, O.; Myte, R.; Schneede, J.; Hägglöf, B.; Bölte, S.; Domellöf, E.; Ivars A’Roch, B.; Elgh, F.; Ueland, P.M.; Silfverdal, S.-A. Maternal Blood Folate Status during Early Pregnancy and Occurrence of Autism Spectrum Disorder in Offspring: A Study of 62 Serum Biomarkers. Mol. Autism 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Steenweg-de Graaff, J.; Ghassabian, A.; Jaddoe, V.W.V.; Tiemeier, H.; Roza, S.J.; Graaff, J.S.; Ghassabian, A.; Jaddoe, V.W.V.; Tiemeier, H.; Roza, S.J. Folate Concentrations during Pregnancy and Autistic Traits in the Offspring. The Generation R Study. Eur. J. Public Health 2015, 25, 431–433. [Google Scholar] [CrossRef]
- Moser, S.; Davidovitch, M.; Rotem, R.S.; Chodick, G.; Shalev, V.; Koren, G.; Sharman, M.S.; Davidovitch, M.; Rotem, R.; Chodick, G.; et al. High Dose Folic Acid during Pregnancy and the Risk of Autism; The Birth Order Bias: A Nested Case-Control Study. Reprod. Toxicol. 2019, 89, 173–177. [Google Scholar] [CrossRef]
- Levine, S.Z.; Kodesh, A.; Viktorin, A.; Smith, L.; Uher, R.; Reichenberg, A.; Sandin, S. Association of Maternal Use of Folic Acid and Multivitamin Supplements in the Periods Before and During Pregnancy With the Risk OfAutism Spectrum Disorder in Offspring. JAMA Psychiatry 2018, 75, 176–184. [Google Scholar] [CrossRef]
- Brieger, K.K.; Bakulski, K.M.; Pearce, C.L.; Baylin, A.; Dou, J.F.; Feinberg, J.I.; Croen, L.A.; Hertz-Picciotto, I.; Newschaffer, C.J.; Fallin, M.D.; et al. The Association of Prenatal Vitamins and Folic Acid Supplement Intake with Odds of Autism Spectrum Disorder in a High-Risk Sibling Cohort, the Early Autism Risk Longitudinal Investigation (EARLI). J. Autism Dev. Disord. 2021, 89, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Yang, T.; Zhu, J.; Li, Q.; Lai, X.; Li, Y.; Tang, T.; Chen, J.; Li, T. Maternal Folic Acid and Micronutrient Supplementation Is Associated with Vitamin Levels and Symptoms in Children with Autism Spectrum Disorders. Reprod. Toxicol. 2020, 91, 109–115. [Google Scholar] [CrossRef]
- Devilbiss, E.A.; Magnusson, C.; Gardner, R.M.; Rai, D.; Newschaffer, C.J.; Lyall, K.; Dalman, C.; Lee, B.K. Antenatal Nutritional Supplementation and Autism Spectrum Disorders in the Stockholm Youth Cohort: Population Based Cohort Study. BMJ 2017, 359, j4273. [Google Scholar] [CrossRef]
- Surén, P.; Roth, C.; Bresnahan, M.; Haugen, M.; Hornig, M.; Hirtz, D.; Lie, K.K.; Lipkin, W.I.; Magnus, P.; Reichborn-Kjennerud, T.; et al. Association between Maternal Use of Folic Acid Supplements and Risk of Autism Spectrum Disorders in Children. JAMA 2013, 309, 570–577. [Google Scholar] [CrossRef]
- Nilsen, R.M.; Surén, P.; Gunnes, N.; Alsaker, E.R.; Bresnahan, M.; Hirtz, D.; Hornig, M.; Lie, K.K.; Lipkin, W.I.; Reichborn-Kjennerud, T.; et al. Analysis of Self-Selection Bias in a Population-Based Cohort Study of Autism Spectrum Disorders. Paediatr. Perinat. Epidemiol. 2013, 27, 553–563. [Google Scholar] [CrossRef]
- Schmidt, R.J.; Iosif, A.M.; Guerrero Angel, E.; Ozonoff, S. Association of Maternal Prenatal Vitamin Use with Risk for Autism Spectrum Disorder Recurrence in Young Siblings. JAMA Psychiatry 2019, 76, 391–398. [Google Scholar] [CrossRef]
- Li, Y.; Shen, Y.; Li, Y.; Xun, G.; Liu, H.; Wu, R.; Xia, K.; Zhao, J.; Ou, J. Maternal Dietary Patterns, Supplements Intake and Autism Spectrum Disorders A Preliminary Case-Control Study. Medicine 2018, 97, e13902. [Google Scholar] [CrossRef]
- Strøm, M.; Granström, C.; Lyall, K.; Ascherio, A.; Olsen, S.F. Research Letter: Folic Acid Supplementation and Intake of Folate in Pregnancy in Relation to Offspring Risk of Autism Spectrum Disorder. Psychol. Med. 2018, 48, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Virk, J.; Liew, Z.; Olsen, J.; Nohr, E.A.; Catov, J.M.; Ritz, B. Preconceptional and Prenatal Supplementary Folic Acid and Multivitamin Intake and Autism Spectrum Disorders. Autism 2016, 20, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.J.; Tancredi, D.J.; Ozonoff, S.; Hansen, R.L.; Hartiala, J.; Allayee, H.; Schmidt, L.C.; Tassone, F.; Hertz-Picciotto, I. Maternal Periconceptional Folic Acid Intake and Risk of Autism Spectrum Disorders and Developmental Delay in the CHARGE (CHildhood Autism Risks from Genetics and Environment) Case-Control Study. Am. J. Clin. Nutr. 2012, 96, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Gammon, C.S.; von Hurst, P.R.; Coad, J.; Kruger, R.; Stonehouse, W. Vegetarianism, Vitamin B12 Status, and Insulin Resistance in a Group of Predominantly Overweight/Obese South Asian Women. Nutrition 2012, 28, 20–24. [Google Scholar] [CrossRef]
- Lampi, K.M.; Sourander, A.; Gissler, M.; Niemelä, S.; Rehnström, K.; Pulkkinen, E.; Peltonen, L.; Von Wendt, L. Brief Report: Validity of Finnish Registry-Based Diagnoses of Autism with the ADI-R. Acta Paediatr. 2010, 99, 1425–1428. [Google Scholar] [CrossRef]
- Behere, R.V.; Deshmukh, A.S.; Otiv, S.; Gupte, M.D.; Yajnik, C.S. Maternal Vitamin B12 Status During Pregnancy and Its Association With Outcomes of Pregnancy and Health of the Offspring: A Systematic Review and Implications for Policy in India. Front. Endocrinol. 2021, 12, 288. [Google Scholar] [CrossRef] [PubMed]
- Jokiranta, E.; Brown, A.S.; Heinimaa, M.; Cheslack-Postava, K.; Suominen, A.; Sourander, A. Parental Psychiatric Disorders and Autism Spectrum Disorders. Psychiatry Res. 2013, 207, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Lampi, K.M.; Hinkka-Yli-Salomäki, S.; Lehti, V.; Helenius, H.; Gissler, M.; Brown, A.S.; Sourander, A. Parental Age and Risk of Autism Spectrum Disorders in a Finnish National Birth Cohort. J. Autism Dev. Disord. 2013, 43, 2526–2535. [Google Scholar] [CrossRef]
- Polo-Kantola, P.; Lampi, K.M.; Hinkka-Yli-Salomäki, S.; Gissler, M.; Brown, A.S.; Sourander, A. Obstetric Risk Factors and Autism Spectrum Disorders in Finland. J. Pediatr. 2014, 164, 358–365. [Google Scholar] [CrossRef]
- Tran, P.L.; Lehti, V.; Lampi, K.M.; Helenius, H.; Suominen, A.; Gissler, M.; Brown, A.S.; Sourander, A. Smoking during Pregnancy and Risk of Autism Spectrum Disorder in a Finnish National Birth Cohort. Paediatr. Perinat. Epidemiol. 2013, 27, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Bergen, N.; Jaddoe, V.; Timmermans, S.; Hofman, A.; Lindemans, J.; Russcher, H.; Raat, H.; Steegers-Theunissen, R.; Steegers, E. Homocysteine and Folate Concentrations in Early Pregnancy and the Risk of Adverse Pregnancy Outcomes: The Generation R Study. BJOG: Int. J. Obstet. Gynaecol. 2012, 119, 739–751. [Google Scholar] [CrossRef]
- Adaikalakoteswari, A.; Vatish, M.; Lawson, A.; Wood, C.; Sivakumar, K.; McTernan, P.G.; Webster, C.; Anderson, N.; Yajnik, C.S.; Tripathi, G.; et al. Low Maternal Vitamin B12 Status Is Associated with Lower Cord Blood HDL Cholesterol in White Caucasians Living in the UK. Nutrients 2015, 7, 2401–2414. [Google Scholar] [CrossRef]
- Raubenheimer, D.; Lee, K.P.; Simpson, S.J. Does Bertrand’s Rule Apply to Macronutrients? Proc. R. Soc. B Biol. Sci. 2005, 272, 2429–2434. [Google Scholar] [CrossRef] [PubMed]
- Sourander, A.; Silwal, S.; Upadhyaya, S.; Surcel, H.-M.; Hinkka-Yli-Salomäki, S.; McKeague, I.W.; Cheslack-Postava, K.; Brown, A.S. Maternal Serum Vitamin B12 and Offspring Attention-Deficit/Hyperactivity Disorder (Adhd). Eur. Child Adolesc. Psychiatry 2020, 30, 1449–1462. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S.; Bottiglieri, T.; Schaefer, C.A.; Quesenberry, C.P.; Liu, L.; Bresnahan, M.; Susser, E.S. Elevated Prenatal Homocysteine Levels as a Risk Factor for Schizophrenia. Arch. Gen. Psychiatry 2007, 64, 31–39. [Google Scholar] [CrossRef]
- Choi, S.-Y. Synaptic and Circuit Development of the Primary Sensory Cortex. Exp. Mol. Med. 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Bourgeron, T. From the Genetic Architecture to Synaptic Plasticity in Autism Spectrum Disorder. Nat. Rev. Neurosci. 2015, 16, 551–563. [Google Scholar] [CrossRef]
- Rodriguez-Gomez, D.A.; Garcia-Guaqueta, D.P.; Charry-Sánchez, J.D.; Sarquis-Buitrago, E.; Blanco, M.; Velez-van-Meerbeke, A.; Talero-Gutiérrez, C. A Systematic Review of Common Genetic Variation and Biological Pathways in Autism Spectrum Disorder. BMC Neurosci. 2021, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M. Effects of Vitamin B12 and Folate Deficiency on Brain Development in Children. Food Nutr. Bull. 2008, 29, S126–S131. [Google Scholar] [CrossRef] [PubMed]
- McCullough, L.E.; Miller, E.E.; Mendez, M.A.; Murtha, A.P.; Murphy, S.K.; Hoyo, C. Maternal B Vitamins: Effects on Offspring Weight and DNA Methylation at Genomically Imprinted Domains. Clin. Epigenetics 2016, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Peker, E.; Demir, N.; Tuncer, O.; Üstyol, L.; Balahoroğlu, R.; Kaba, S.; Karaman, K. The Levels of Vitamin B 12, Folate and Homocysteine in Mothers and Their Babies with Neural Tube Defects. J. Matern. -Fetal Neonatal Med. 2016, 29, 2944–2948. [Google Scholar] [CrossRef] [PubMed]
- Reischl-Hajiabadi, A.T.; Garbade, S.F.; Feyh, P.; Weiss, K.H.; Mütze, U.; Kölker, S.; Hoffmann, G.F.; Gramer, G. Maternal Vitamin B12 Deficiency Detected by Newborn Screening-Evaluation of Causes and Characteristics. Nutrients 2022, 14, 3767. [Google Scholar] [CrossRef]
- Ünsür, E.; Kınaş, B.; Kutlusoy, F.; Aksoy, Ü.; Şahin, K.; Ünsür, T.; Aksoy, H.; Tekkeşin, N. The Relationship between Maternal and Neonatal Vitamin B12 and Folate Levels, Anthropometric Measurements, and Metabolic Indicators. J. Surg. Med. 2020, 4, 43–47. [Google Scholar] [CrossRef]


{kind=link}
| Covariates | Maternal Vitamin B12 | Maternal Vitamin B12 | p-Value | |||
|---|---|---|---|---|---|---|
| ≥Median | <Median | |||||
| Mean | SD | Mean | SD | |||
| t | ||||||
| Maternal age (years) | 29.35 | 5.23 | 29.69 | 5.08 | 1.30 | 0.195 |
| Gestational week of blood draw | 9.94 | 2.75 | 10.26 | 2.87 | 2.31 | 0.021 |
| n | % | n | % | χ2 | ||
| Maternal smoking | 1.78 | 0.409 | ||||
| No | 659 | 84.38 | 636 | 81.85 | ||
| Yes | 107 | 13.70 | 123 | 15.83 | ||
| Previous births 1 | ||||||
| 0 | 315 | 40.38 | 332 | 43.01 | 1.09 | 0.295 |
| ≥1 | 465 | 59.62 | 440 | 56.99 | ||
| History of maternal Psychopathology a | 0.07 | 0.795 | ||||
| No | 674 | 86.30 | 667 | 85.84 | ||
| Yes | 107 | 13.70 | 110 | 14.16 | ||
| History of paternal psychopathology b 2 | 0.04 | 0.834 | ||||
| No | 676 | 86.89 | 668 | 86.53 | ||
| Yes | 102 | 13.11 | 104 | 13.47 | ||
| Maternal SES | 8.32 | 0.081 | ||||
| Upper white collar | 107 | 13.70 | 117 | 15.06 | ||
| Lower white collar | 329 | 42.13 | 293 | 37.71 | ||
| Blue collar | 161 | 20.61 | 148 | 19.05 | ||
| Others | 116 | 14.85 | 122 | 15.70 | ||
| Missing | 68 | 8.71 | 97 | 12.48 | ||
| History of maternal substance abuse c | 1.16 | 0.282 | ||||
| No | 762 | 97.57 | 751 | 96.65 | ||
| Yes | 19 | 2.43 | 26 | 3.35 | ||
| Gestational age (weeks) 3 | 2.53 | 0.112 | ||||
| <37 | 20 | 2.57 | 31 | 4.01 | ||
| ≥37 | 759 | 97.43 | 743 | 95.99 | ||
| Weight for gestational age 4 | 3.91 | 0.141 | ||||
| <−2 SD | 13 | 1.67 | 15 | 1.94 | ||
| −2 SD to +2 SD | 733 | 94.09 | 739 | 95.60 | ||
| >+2 SD | 33 | 4.24 | 19 | 2.46 | ||
| Maternal immigration status | 7.41 | 0.007 | ||||
| No | 760 | 97.31 | 735 | 94.59 | ||
| Yes | 21 | 2.69 | 42 | 5.41 | ||
| Season of blood collection | 3.23 | 0.358 | ||||
| Spring | 191 | 24.46 | 196 | 25.23 | ||
| Summer | 212 | 27.14 | 186 | 23.94 | ||
| Autumn | 198 | 25.35 | 192 | 24.71 | ||
| Winter | 180 | 23.05 | 203 | 26.13 | ||
| Apgar Score 5 | ||||||
| 0–6 | 27 | 3.47 | 30 | 3.88 | 0.72 | 0.699 |
| 7–8 | 164 | 21.11 | 151 | 19.53 | ||
| 9–10 | 586 | 75.42 | 592 | 76.58 | ||
| Covariates | Cases | Controls | p-Value | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| t | ||||||
| Maternal age (years) | 29.91 | 5.45 | 29.53 | 5.16 | −2.00 | 0.046 |
| Gestational week of blood draw | 10.79 | 3.53 | 10.09 | 2.81 | −6.05 | <0.001 |
| n | % | n | % | χ2 | ||
| Maternal smoking | 2.25 | 0.325 | ||||
| No | 1273 | 81.71 | 1295 | 83.12 | ||
| Yes | 240 | 15.40 | 230 | 14.76 | ||
| Previous births 1 | 12.41 | <0.001 | ||||
| 0 | 746 | 47.97 | 647 | 41.69 | ||
| ≥ 1 | 809 | 52.03 | 905 | 58.31 | ||
| History of maternal psychopathology a | 91.44 | <0.001 | ||||
| No | 1124 | 72.14 | 1341 | 86.07 | ||
| Yes | 434 | 27.86 | 217 | 13.93 | ||
| History of paternal psychopathology b 2 | 36.19 | <0.001 | ||||
| No | 1201 | 78.50 | 1344 | 86.71 | ||
| Yes | 329 | 21.50 | 206 | 13.29 | ||
| Maternal SES | 9.83 | 0.043 | ||||
| Upper white collar | 197 | 12.64 | 224 | 14.38 | ||
| Lower white collar | 599 | 38.45 | 622 | 39.92 | ||
| Blue collar | 288 | 18.49 | 309 | 19.83 | ||
| Others | 297 | 19.06 | 238 | 15.28 | ||
| Missing | 177 | 11.36 | 165 | 10.59 | ||
| History of maternal substance abuse c | 13.39 | <0.001 | ||||
| No | 1472 | 94.48 | 1513 | 97.11 | ||
| Yes | 86 | 5.52 | 45 | 2.89 | ||
| Gestational age (weeks) 3 | 15.11 | <0.001 | ||||
| <37 | 97 | 6.26 | 51 | 3.28 | ||
| ≥37 | 1453 | 93.71 | 1502 | 96.72 | ||
| Weight for gestational age 4 | 7.68 | 0.022 | ||||
| <−2 SD | 52 | 3.36 | 28 | 1.80 | ||
| −2 SD to +2 SD | 1441 | 93.03 | 1472 | 94.85 | ||
| >+2 SD | 56 | 3.62 | 52 | 3.35 | ||
| Maternal immigration status | 0.14 | 0.712 | ||||
| No | 1499 | 96.21 | 1495 | 95.96 | ||
| Yes | 59 | 3.79 | 63 | 4.04 | ||
| Season of blood collection | 82.91 | 0.406 | ||||
| Spring | 350 | 22.46 | 387 | 24.84 | ||
| Summer | 411 | 26.38 | 398 | 25.55 | ||
| Autumn | 416 | 26.70 | 390 | 25.03 | ||
| Winter | 381 | 24.45 | 383 | 24.58 | ||
| Apgar Score 5 | ||||||
| 0–6 | 72 | 4.63 | 57 | 3.68 | 4.94 | 0.085 |
| 7–8 | 353 | 22.72 | 315 | 20.32 | ||
| 9–10 | 1129 | 72.65 | 1178 | 76.00 | ||
| Log-Transformed Maternal Vitamin B12 Levels (pmol/L) | Case (N = 1558) | Control (N = 1558) | Odds Ratio Unadjusted (95% CI) | p-Value | Odds Ratio Adjusted a (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Median | Median | |||||
| ASD | 4.74 | 4.74 | 0.90 (0.77–1.06) | 0.209 | 0.94 (0.79–1.10) | 0.441 |
| Childhood autism | (n = 491) | (n = 491) | ||||
| 4.78 | 4.75 | 0.94 (0.71–1.25) | 0.660 | 0.96 (0.72–1.28) | 0.774 | |
| Asperger’s | (n = 536) | (n = 536) | ||||
| 4.74 | 4.74 | 0.96 (0.72–1.27) | 0.759 | 1.05 (0.78–1.42) | 0.734 | |
| PDD/PDD-NOS | (n = 531) | (n = 531) | ||||
| 4.73 | 4.75 | 0.83 (0.64–1.08) | 0.169 | 0.87 (0.66–1.15) | 0.316 |
| Maternal Serum Vitamin B12 in Quintiles (pmol/L) | Cases n (%) | Controls n (%) | Odds Ratio Unadjusted (95% CI) | p-Value | Odds Ratio Adjusted a (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| (N = 1558) | (N = 1558) | ||||
| 0–20 (0–80.8) | 331 (21.25) | 312 (20.03) | 1.13 (0.91–1.41) | 0.278 | 1.06 (0.85–1.34) | 0.582 |
| 21–40 (80.9–105.4) | 328 (21.05) | 313 (20.09) | 1.12 (0.89–1.39) | 0.331 | 1.09 (0.87–1.36) | 0.455 |
| 41–60 (105.5–128.9) | 290 (18.61) | 310 (19.90) | Reference | Reference | ||
| 61–80 (128.8–164.9) | 310 (19.90) | 312 (20.03) | 1.06 (0.85–1.33) | 0.618 | 1.09 (0.87–1.36) | 0.853 |
| ≥81 (≥165) | 299 (19.19) | 311 (19.96) | 1.02 (0.82–1.28) | 0.849 | 1.02 (0.81–1.29) | 0.869 |
| (N = 491) | (N = 491) | ||||
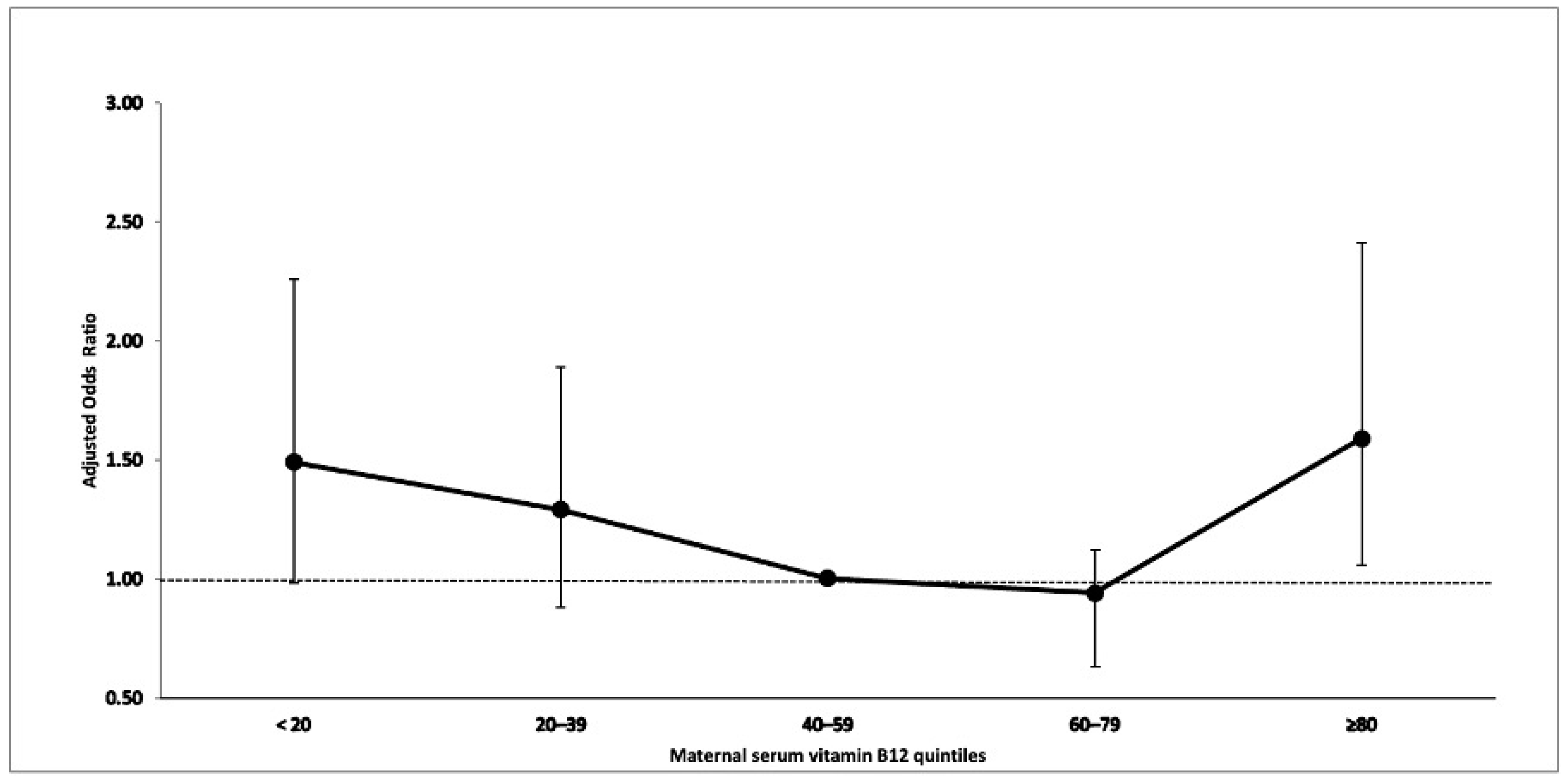
| 0–20 (0–80.8) | 104 (21.18) | 86 (17.52) | 1.52 (1.01–2.31) | 0.047 | 1.49 (0.98–2.26) | 0.064 |
| 21–40 (80.9–105.4) | 99 (20.16) | 94 (19.14) | 1.27 (0.87–1.86) | 0.212 | 1.29 (0.88–1.89) | 0.199 |
| 41–60 (105.5–128.9) | 90 (18.33) | 111 (22.61) | Reference | Reference | ||
| 61–80 (128.8–164.9) | 89 (18.33) | 111 (22.61) | 0.99 (0.67–1.49) | 0.997 | 0.94 (0.63–1.42) | 0.778 |
| ≥81 (≥165) | 109 (22.20) | 89 (18.13) | 1.52 (1.02–2.28) | 0.042 | 1.59 (1.06–2.41) | 0.026 |
| (N = 536) | (N = 536) | ||||
| 0–20 (0–80.8) | 110 (20.52) | 120 (22.39) | 0.97 (0.68–1.39) | 0.872 | 0.87 (0.60–1.27) | 0.477 |
| 21–40 (80.9–105.4) | 114 (21.27) | 109 (20.34) | 1.13 (0.77–1.66) | 0.528 | 1.03 (0.69–1.53) | 0.883 |
| 41–60 (105.5–128.9) | 98 (18.28) | 103 (19.22) | Reference | Reference | ||
| 61–80 (128.8–164.9) | 116 (21.64) | 97 (18.10) | 1.29 (0.87–1.90) | 0.205 | 1.25 (0.83–1.87) | 0.283 |
| ≥81 (≥165) | 98 (18.28) | 107 (19.96) | 0.98 (0.67–1.43) | 0.901 | 0.99 (0.67–1.47) | 0.965 |
| (N = 531) | (N = 531) | ||||
| 0–20 (0–80.8) | 117 (22.03) | 106 (19.96) | 1.04 (0.70–1.54) | 0.854 | 0.99 (0.65–1.51) | 0.965 |
| 21–40 (80.9–105.4) | 115 (21.66) | 110 (20.72) | 0.99 (0.68–1.45) | 0.954 | 0.99 (0.66–1.49) | 0.980 |
| 41–60 (105.5–128.9) | 102 (19.21) | 96 (18.08) | Reference | Reference | ||
| 61–80 (128.8–164.9) | 105 (19.77) | 104 (19.59) | 0.95 (0.64–1.39) | 0.789 | 0.99 (0.66–1.50) | 0.982 |
| ≥81 (≥165) | 92 (17.33) | 115 (21.66) | 0.76 (0.52–1.12) | 0.168 | 0.74 (0.49–1.12) | 0.159 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sourander, A.; Silwal, S.; Surcel, H.-M.; Hinkka-Yli-Salomäki, S.; Upadhyaya, S.; McKeague, I.W.; Cheslack-Postava, K.; Brown, A.S. Maternal Serum Vitamin B12 during Pregnancy and Offspring Autism Spectrum Disorder. Nutrients 2023, 15, 2009. https://doi.org/10.3390/nu15082009
Sourander A, Silwal S, Surcel H-M, Hinkka-Yli-Salomäki S, Upadhyaya S, McKeague IW, Cheslack-Postava K, Brown AS. Maternal Serum Vitamin B12 during Pregnancy and Offspring Autism Spectrum Disorder. Nutrients. 2023; 15(8):2009. https://doi.org/10.3390/nu15082009
Chicago/Turabian StyleSourander, Andre, Sanju Silwal, Heljä-Marja Surcel, Susanna Hinkka-Yli-Salomäki, Subina Upadhyaya, Ian W. McKeague, Keely Cheslack-Postava, and Alan S. Brown. 2023. "Maternal Serum Vitamin B12 during Pregnancy and Offspring Autism Spectrum Disorder" Nutrients 15, no. 8: 2009. https://doi.org/10.3390/nu15082009
APA StyleSourander, A., Silwal, S., Surcel, H. -M., Hinkka-Yli-Salomäki, S., Upadhyaya, S., McKeague, I. W., Cheslack-Postava, K., & Brown, A. S. (2023). Maternal Serum Vitamin B12 during Pregnancy and Offspring Autism Spectrum Disorder. Nutrients, 15(8), 2009. https://doi.org/10.3390/nu15082009