PIM-1 Is Overexpressed at a High Frequency in Circulating Tumor Cells from Metastatic Castration-Resistant Prostate Cancer Patients


 ,
, 
Abstract
:1. Introduction
2. Results
2.1. TCGA Analysis
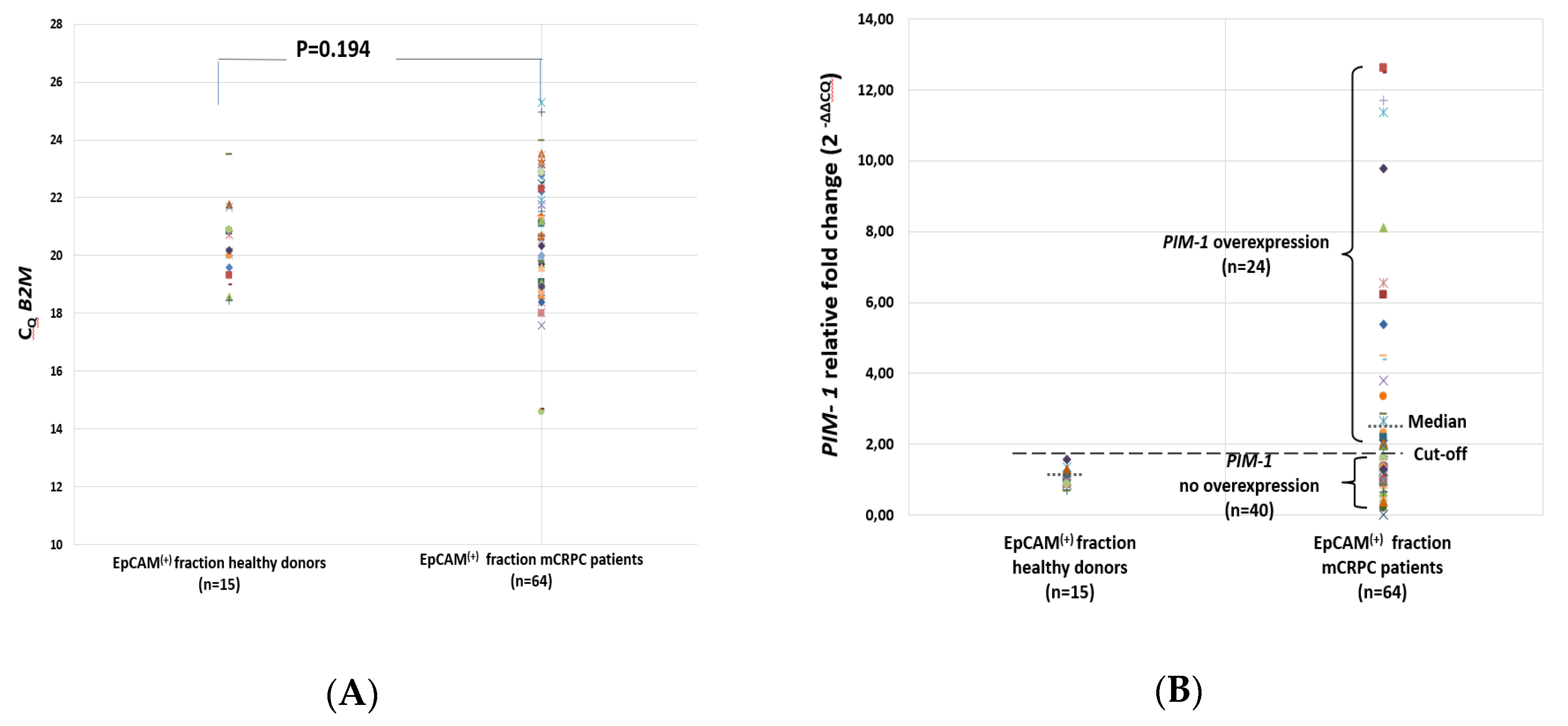
2.2. PIM-1 Overexpression in EpCAM(+) CTC Fraction
2.3. PIM-1 Overexpression in the EpCAM(+) CTC Fraction before and after Treatment
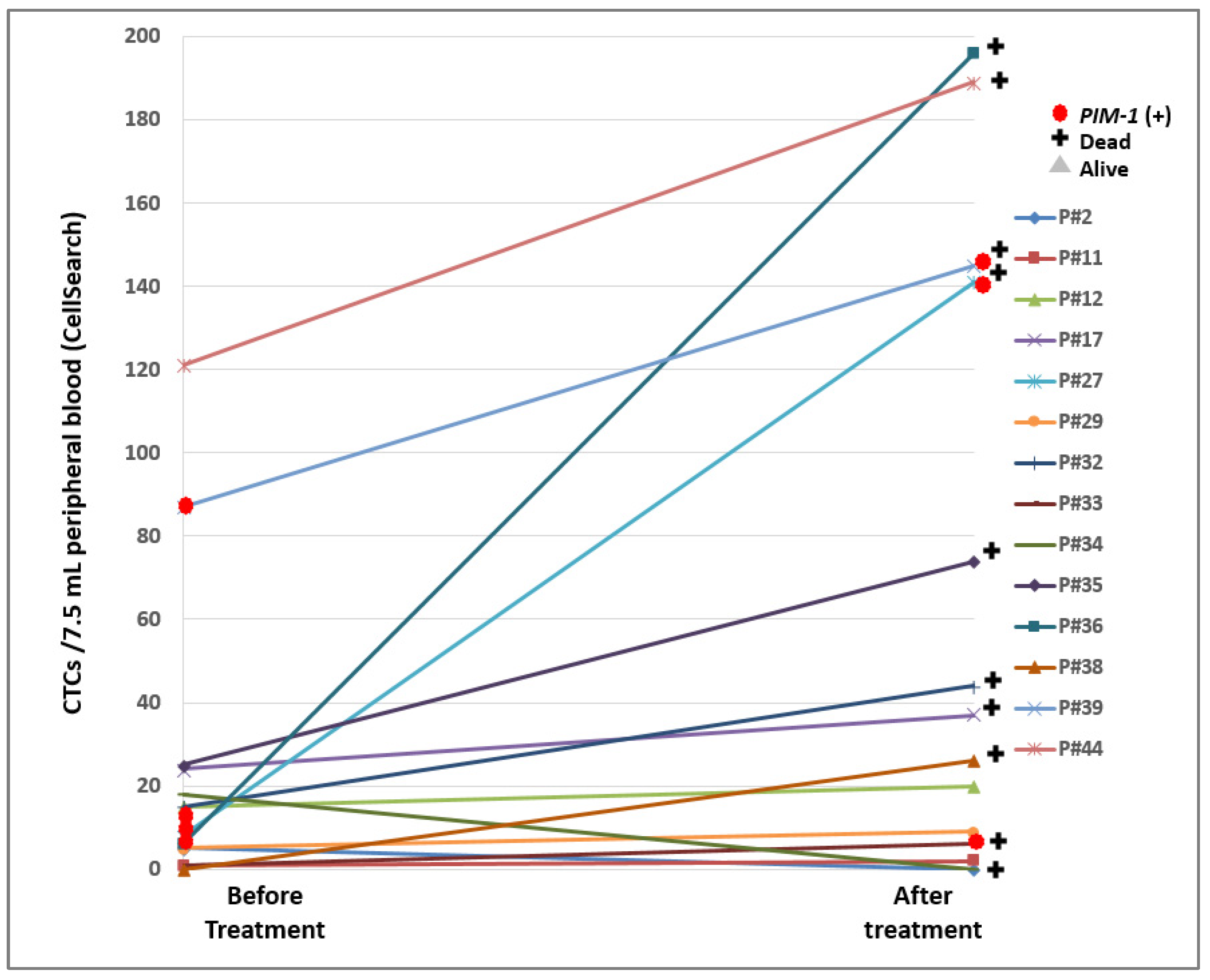
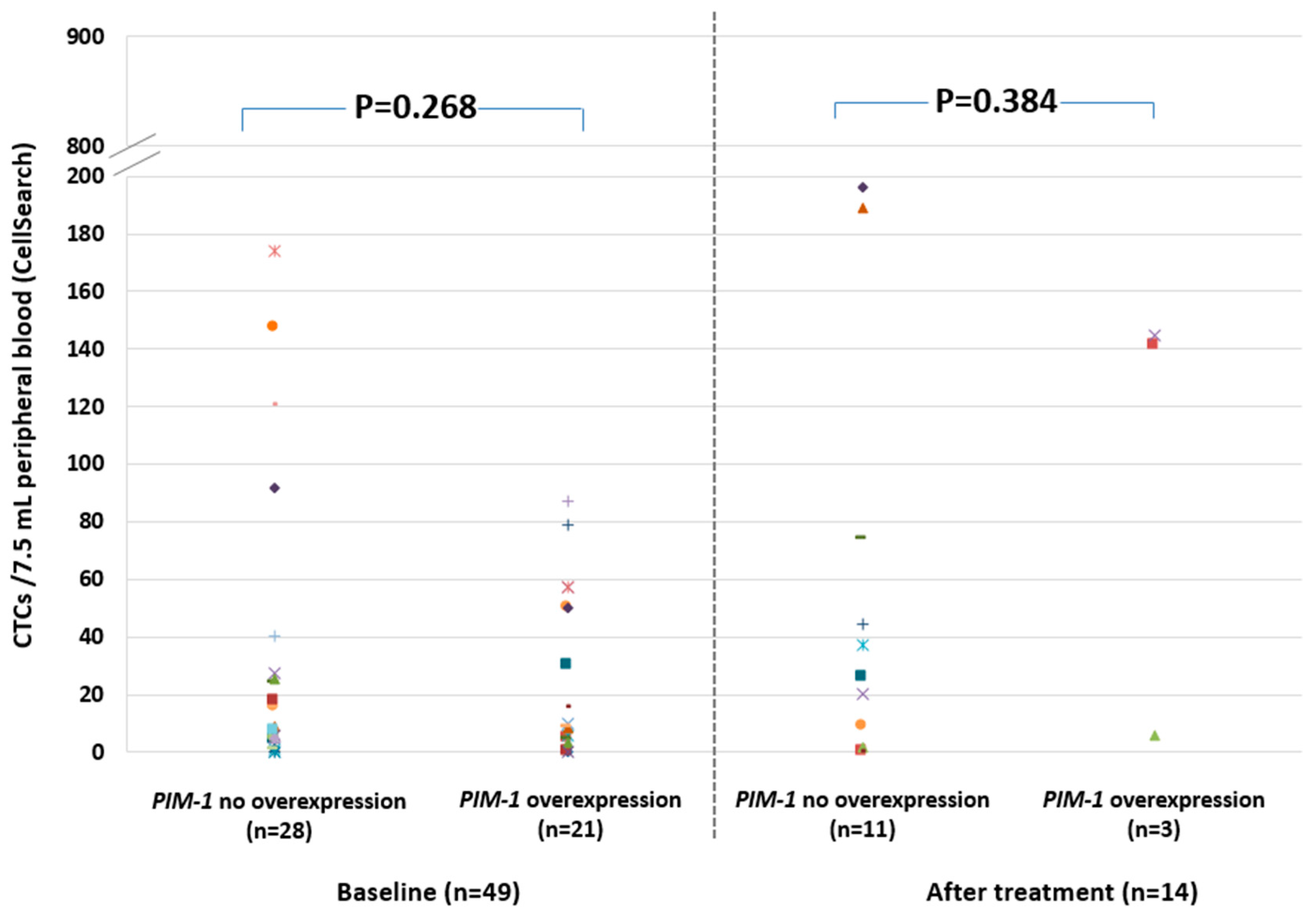
2.4. PIM-1 Overexpression in Relation to CTC Enumeration in the CellSearch® System
2.5. PIM-1 Overexpression in Relation to AR-V7 Expression
3. Discussion
4. Materials and Methods
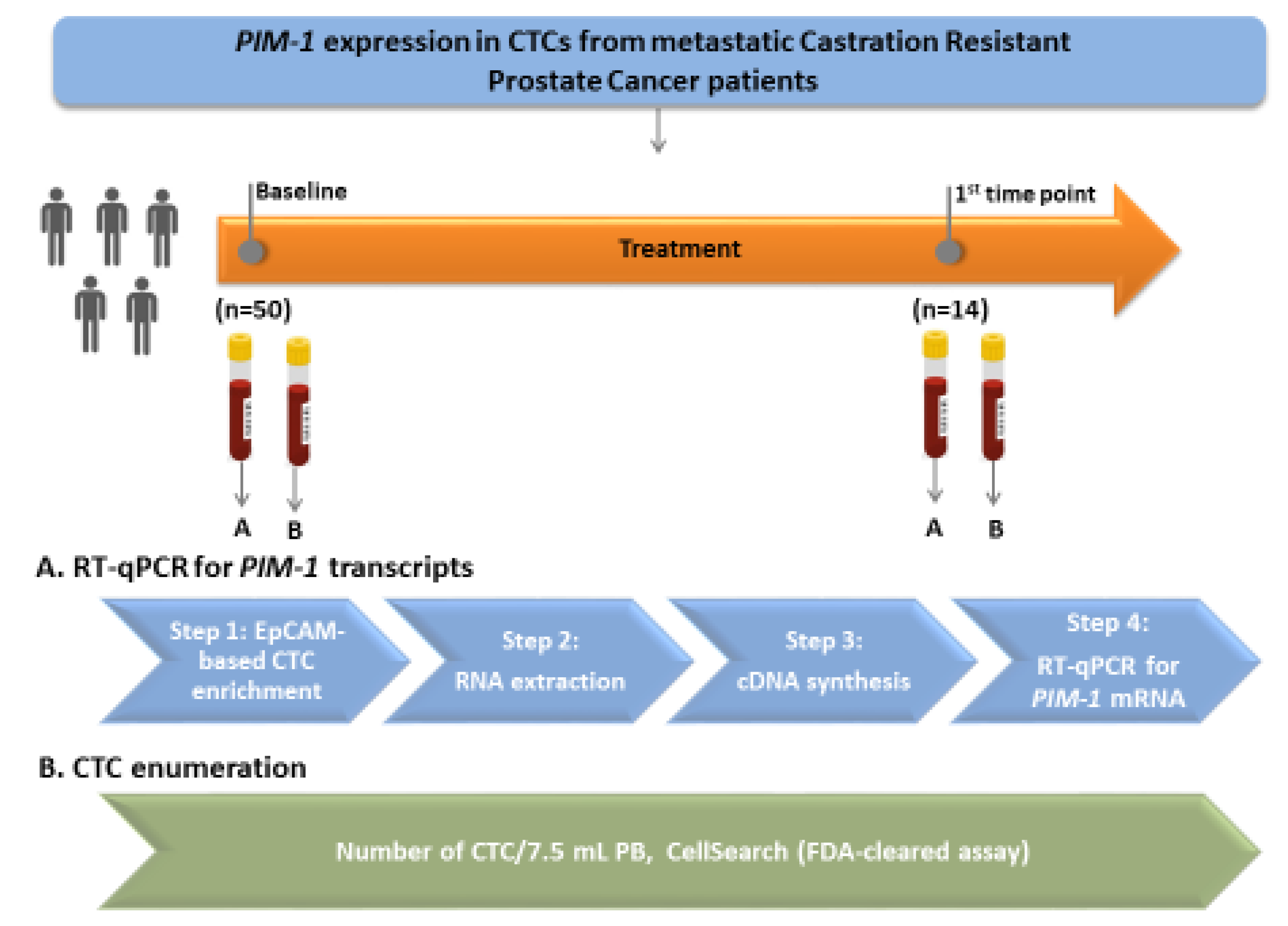
4.1. Clinical Samples
4.2. CTC Enumeration in the CellSearch®
4.3. CTC Immunomagnetic Enrichment and RNA-Based Analysis
4.4. RT-qPCR Assay for PIM-1 Expression
4.5. RT-qPCR Assay for AR-V7 Expression
4.6. Quality Control
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ADT | Androgen Deprivation Therapy |
| AR | Androgen Receptor |
| AR-V7 | Androgen Receptor splice variant 7 |
| CTCs | Circulating Tumor Cells |
| CtDNA | Circulating tumor DNA |
| EMT | Epithelial Mesenchymal Transition |
| EVs | Extracellular Vesicles |
| HD | Healthy Donors |
| CRPC | Castration-Resistant Prostate Cancer |
| PB | Peripheral Blood |
| PCa | Prostate Cancer |
| PRAD | Prostate Adenocarcinoma |
| TPM | Transcripts Per Million |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- PDQ Adult Treatment Editorial Board. Prostate Cancer Treatment (PDQ®): Patient Version. 30 April 2018. In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2002. [Google Scholar]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantel, K.; Hille, C.; Scher, H.I. Circulating Tumor Cells in Prostate Cancer: From Discovery to Clinical Utility. Clin. Chem. 2019, 65, 87–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumanasuriya, S.; De Bono, J. Treatment of Advanced Prostate Cancer-A Review of Current Therapies and Future Promise. Cold Spring Harb. Perspect Med. 2018, 8, a030635. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, R.J.; Van Oort, I.M.; Schalken, J.A. Blood-based and urinary prostate cancer biomarkers: A review and comparison of novel biomarkers for detection and treatment decisions. Prostate Cancer Prostatic Dis. 2017, 20, 12–19. [Google Scholar] [CrossRef]
- Filella, X.; Albaladejo, M.D.; Allué, J.A.; Castaño, M.A.; Morell-Garcia, D.; Ruiz, M.À.; Santamaría, M.; Torrejón, M.J.; Giménez, N. Prostate cancer screening: Guidelines review and laboratory issues. Clin. Chem. Lab. Med. 2019, 57, 1474–1487. [Google Scholar] [CrossRef]
- Lianidou, E.; Hoon, D. Circulating Tumor Cells and circulating Tumor DNA. In Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 6th ed.; Rifai, N., Horvath, A.-R., Wittwer, C., Eds.; Elsevier B.V.: Amsterdam, The Netherlands, 2017; pp. 1111–1144. [Google Scholar]
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease-latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef]
- Castro-Giner, F.; Aceto, N. Tracking cancer progression: From circulating tumor cells to metastasis. Genome Med. 2020, 12, 31. [Google Scholar] [CrossRef] [Green Version]
- Alix-Panabières, C. “Circulating Tumor Cells: Finding Rare Events for a Huge Knowledge of Cancer Dissemination”. Cells 2020, 3, 661. [Google Scholar] [CrossRef] [Green Version]
- De Bono, J.; Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.; Terstappen, L.W.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [Green Version]
- Scher, H.I.; Jia, X.; De Bono, J.S.; Fleisher, M.; Pienta, K.J.; Raghavan, D.; Heller, G. Circulating tumour cells as prognostic markers in progressive, castration-resistant prostate cancer: A reanalysis of IMMC38 trial data. Lancet Oncol. 2009, 10, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Wang, H.; Chen, Y.; Nakazawa, M.; Nadal, R.; Paller, C.J.; Denmeade, S.R.; Carducci, M.A.; et al. Androgen receptor splice variant 7 and efficacy of taxane chemotherapy in patients with metastatic castration-resistant prostate cancer. JAMA Oncol. 2015, 1, 582–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strati, A.; Zavridou, M.; Bournakis, E.; Mastoraki, S.; Lianidou, E. Expression pattern of androgen receptors, AR-V7 and AR-567es, in circulating tumor cells and paired plasma-derived extracellular vesicles in metastatic castration resistant prostate cancer. Analyst 2019, 144, 6671–6680. [Google Scholar] [CrossRef] [PubMed]
- Narlik-Grassow, M.; Blanco-Aparicio, C.; Carnero, A. The PIM family of serine/threonine kinases in cancer. Med. Res. Rev. 2014, 34, 136–159. [Google Scholar] [CrossRef] [PubMed]
- Warfel, N.A.; Kraft, A.S. PIM kinase (and Akt) biology and signaling in tumors. Pharmacol. Ther. 2015, 151, 41–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cen, B.; Mahajan, S.; Wang, W.; Kraft, A.S. Elevation of receptor tyrosine kinases by small molecule AKT inhibitors in prostate cancer is mediated by Pim-1. Cancer Res. 2013, 73, 3402–3411. [Google Scholar] [CrossRef] [Green Version]
- Tursynbay, Y.; Zhang, J.; Li, Z.; Tokay, T.; Zhumadilov, Z.; Wu, D.; Xie, Y. Pim-1 kinase as cancer drug target: An update. Biomed. Rep. 2016, 4, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casillas, A.L.; Toth, R.K.; Sainz, A.G.; Singh, N.; Desai, A.A. Hypoxia-Inducible PIM kinase expression promotes resistance to antiangiogenic agents. Clin. Cancer Res. 2018, 24, 169–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, M.G.; Obinata, D.; Sandhu, S.; Selth, L.A.; Wong, S.Q.; Porter, L.H.; Lister, N.; Pook, D.; Pezaro, C.J.; Goode, D.L.; et al. Patient-derived Models of Abiraterone- and Enzalutamide-resistant Prostate Cancer Reveal Sensitivity to Ribosome-directed Therapy. Eur. Urol. 2018, 74, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Qie, Y.; Yang, T.; Wang, L.; Du, E.; Liu, Y.; Xu, Y.; Qiao, B.; Zhang, Z. Kinase PIM1 promotes prostate cancer cell growth via c-Myc-RPS7-driven ribosomal stress. Carcinogenesis 2019, 40, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Kim, J.; Roh, M.; Franco, O.E.; Hayward, S.W.; Wills, M.L.; Abdulkadir, S.A. Pim1 kinase synergizes with c-MYC to induce advanced prostate carcinoma. Oncogene 2010, 29, 2477–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhanasekaran, S.M.; Barrette, T.R.; Ghosh, D.; Shah, R.; Varambally, S.; Kurachi, K.; Pienta, K.J.; Rubin, M.A.; Chinnaiyan, A.M. Delineation of prognostic biomarkers in prostate cancer. Nature 2001, 412, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Valdman, A.; Fang, X.; Pang, S.T.; Ekman, P.; Egevad, L. Pim-1 expression in prostatic intraepithelial neoplasia and human prostate cancer. Prostate 2004, 60, 367–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cibull, T.L.; Jones, T.D.; Li, L.; Eble, J.N.; Ann Baldridge, L.; Malott, S.R.; Luo, Y.; Cheng, L. Overexpression of Pim-1 during progression of prostatic adenocarcinoma. J. Clin. Pathol. 2006, 59, 285–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holder, S.L.; Abdulkadir, S.A. PIM1 kinase as a target in prostate cancer: Roles in tumorigenesis, castration resistance, and docetaxel resistance. Curr. Cancer Drug Targets 2014, 14, 105–114. [Google Scholar] [CrossRef]
- Luszczak, S.; Kumar, C.; Sathyadevan, V.K.; Simpson, B.S.; Gately, K.A.; Whitaker, H.C.; Heavey, S. PIM kinase inhibition: Co-targeted therapeutic approaches in prostate cancer. Signal. Transduct. Target Ther. 2020, 5, 7. [Google Scholar] [CrossRef]
- Moreno, J.G.; Gomella, L.G. Evolution of the Liquid Biopsy in Metastatic Prostate Cancer. Urology 2019, 132. [Google Scholar] [CrossRef]
- Scher, H.I.; Graf, R.P.; Schreiber, N.A.; Jayaram, A.; Winquist, E.; McLaughlin, B.; Lu, D.; Fleisher, M.; Orr, S.; Lowes, L.; et al. Assessment of the validity of nuclear-localized androgen receptor splice variant 7 in circulating tumor cells as a predictive biomarker for castration-resistant prostate cancer. JAMA Oncol. 2018, 4, 1179–1186. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Halabi, S.; Luo, J.; Nanus, D.M.; Giannakakou, P.; Szmulewitz, R.Z.; Danila, D.C.; Healy, P.; Anand, M.; Rothwell, C.J.; et al. Prospective multicenter validation of androgen receptor splice variant 7 and hormone therapy resistance in high-risk castration-resistant prostate cancer: The PROPHECY study. J. Clin. Oncol. 2019, 37, 1120–1129. [Google Scholar] [CrossRef]
- Markou, A.; Lazaridou, M.; Paraskevopoulos, P.; Chen, S.; Świerczewska, M.; Budna, J.; Kuske, A.; Gorges, T.M.; Joosse, S.A.; Kroneis, T.; et al. Multiplex Gene Expression Profiling of in Vivo Isolated Circulating Tumor Cells in High-Risk Prostate Cancer Patients. Clin. Chem. 2018, 64, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Josefsson, A.; Larsson, K.; Freyhult, E.; Damber, J.E.; Welén, K. Gene Expression Alterations during Development of Castration-Resistant Prostate Cancer Are Detected in Circulating Tumor Cells. Cancers 2019, 12, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chimonidou, M.; Strati, A.; Malamos, N.; Georgoulias, V.; Lianidou, E.S. SOX17 promoter methylation in circulating tumor cells and matched cell-free DNA isolated from plasma of patients with BrCa. Clin. Chem. 2013, 59, 270–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastoraki, S.; Strati, A.; Tzanikou, E.; Chimonidou, M.; Politaki, E.; Voutsina, A.; Psyrri, A.; Georgoulias, V.; Lianidou, E. ESR1 Methylation: A Liquid Biopsy–Based Epigenetic Assay for the Follow-up of Patients with Metastatic Breast Cancer Receiving Endocrine Treatment. Clin. Cancer Res. 2018, 24, 1500–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedlander, T.W.; Ngo, V.T.; Dong, H.; Premasekharan, G.; Weinberg, V.; Doty, S.; Zhao, Q.; Gilbert, E.G.; Ryan, C.J.; Chen, W.T.; et al. Detection and characterization of invasive circulating tumor cells derived from men with metastatic castration-resistant prostate cancer. Int. J. Cancer 2014, 134, 2284–2293. [Google Scholar] [CrossRef] [Green Version]
- Pixberg, C.F.; Raba, K.; Müller, F.; Behrens, B.; Honisch, E.; Niederacher, D.; Neubauer, H.; Fehm, T.; Goering, W.; Schulz, W.; et al. Analysis of DNA methylation in single circulating tumor cells. Oncogene 2017, 36, 3223–3231. [Google Scholar] [CrossRef]
- El-Heliebi, A.; Hille, C.; Laxman, N.; Svedlund, J.; Haudum, C.; Ercan, E.; Kroneis, T.; Chen, S.; Smolle, M.; Rossmann, C.; et al. In Situ Detection and Quantification of AR-V7, AR-FL, PSA, and KRAS Point Mutations in Circulating Tumor Cells. Clin. Chem. 2018, 64, 536–546. [Google Scholar] [CrossRef] [Green Version]
- Faugeroux, V.; Lefebvre, C.; Pailler, E.; Pierron, V.; Marcaillou, C.; Tourlet, S.; Billiot, F.; Dogan, S.; Oulhen, M.; Vielh, P.; et al. An Accessible and Unique Insight into Metastasis Mutational Content Through Whole-exome Sequencing of Circulating Tumor Cells in Metastatic Prostate Cancer. Eur. Urol. Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Markou, A.; Farkona, S.; Schiza, C.; Efstathiou, T.; Kounelis, S.; Malamos, N.; Georgoulias, V.; Lianidou, E. PIK3CA mutational status in circulating tumor cells can change during disease recurrence or progression in patients with breast cancer. Clin. Cancer Res. 2014, 20, 5823–5834. [Google Scholar] [CrossRef] [Green Version]
- Tzanikou, E.; Markou, A.; Politaki, E.; Koutsopoulos, A.; Psyrri, A.; Mavroudis, D.; Georgoulias, V.; Lianidou, E. PIK3CA hotspot mutations in circulating tumor cells and paired circulating tumor DNA in breast cancer: A direct comparison study. Mol. Oncol. 2019, 13, 2515–2530. [Google Scholar] [CrossRef] [Green Version]
- Arrouchi, H.; Lakhlili, W.; Ibrahimi, A. A review on PIM kinases in tumors. Bioinformation 2019, 15, 40–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnuson, N.S.; Wang, Z.; Ding, G.; Reeves, R. Why target PIM-1 for cancer diagnosis and treatment? Future Oncol. 2010, 9, 1461–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asati, V.; Mahapatra, D.K.; Bharti, S.K. PIM kinase inhibitors: Structural and pharmacological perspectives. Eur. J. Med. Chem. 2019, 172, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Arrouchi, H.; Lakhlili, W.; Ibrahimi, A. Re-positioning of known drugs for Pim-1 kinase target using molecular docking analysis. Bioinformation 2019, 15, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Casuscelli, F.; Ardini, E.; Avanzi, N.; Casale, E.; Cervi, G.; D’Anello, M.; Donati, D.; Faiardi, D.; Ferguson, R.D.; Fogliatto, G.; et al. Discovery and optimization of pyrrolo[1,2-a]pyrazinones leads to novel and selective inhibitors of PIM kinases. Bioorg. Med. Chem. 2013, 21, 7364–7380. [Google Scholar] [CrossRef] [PubMed]
- Suchaud, V.; Gavara, L.; Giraud, F.; Nauton, L.; Thery, V.; Anizon, F.; Moreau, P. Synthesis of pyrazolo[4,3-a]phenanthridines, a new scaffold for PIM kinase inhibition. Bioorg. Med. Chem. 2014, 22, 4704–4710. [Google Scholar] [CrossRef] [PubMed]
- El-Nassan, H.B.; Naguib, B.H.; Beshay, E.A. Synthesis of new pyridothienopyrimidinone and pyridothienotriazolopyrimidine derivatives as pim-1 inhibitors. J. Enzym. Inhib. Med. Chem. 2018, 33, 58–66. [Google Scholar] [CrossRef]
- Abouzid, K.A.M.; Al-Ansary, G.H.; El-Naggar, A.M. Eco-friendly synthesis of novel cyanopyridine derivatives and their anticancer and PIM-1 kinase inhibitory activities. Eur. J. Med. Chem. 2017, 134, 357–365. [Google Scholar] [CrossRef]
- Bataille, C.J.R.; Brennan, M.B.; Byrne, S.; Davies, S.G.; Durbin, M.; Fedorov, O.; Huber, K.V.M.; Jones, A.M.; Knapp, S.; Liu, G.; et al. Thiazolidine derivatives as potent and selective inhibitors of the PIM kinase family. Bioorg. Med. Chem. 2017, 25, 2657–2665. [Google Scholar] [CrossRef]
- Nishiguchi, G.A.; Atallah, G.; Bellamacina, C.; Burger, M.T.; Ding, Y.; Feucht, P.H.; Garcia, P.D.; Han, W.; Klivansky, L.; Lindvall, M. Discovery of novel 3,5- disubstituted indole derivatives as potent inhibitors of PIM-1, PIM-2, and PIM-3 protein kinases. Bioorg. Med. Chem. Lett. 2011, 21, 6366–6369. [Google Scholar] [CrossRef]
- Fan, Y.B.; Li, K.; Huang, M.; Cao, Y.; Li, Y.; Jin, S.Y.; Liu, W.B.; Wen, J.C.; Liu, D.; Zhao, L.X. Design and synthesis of substituted pyrido[3,2-d]-1,2,3-triazines as potential PIM-1 inhibitors. Bioorg. Med. Chem. Lett. 2016, 26, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Wurz, R.P.; Pettus, L.H.; Jackson, C.; Wu, B.; Wang, H.L.; Herberich, B.; Cee, V.; Lanman, B.A.; Reed, A.B.; Chavez, F.J.; et al. The discovery and optimization of aminooxadiazoles as potent PIM kinase inhibitors. Bioorg. Med. Chem. Lett. 2015, 25, 847–855. [Google Scholar] [CrossRef]
- Li, K.; Li, Y.; Zhou, D.; Fan, Y.; Guo, H.; Ma, T.; Wen, J.; Liu, D.; Zhao, L. Synthesis and biological evaluation of quinoline derivatives as potential anti-prostate cancer agents and PIM-1 kinase inhibitors. Bioorg. Med. Chem. 2016, 24, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Zavridou, M.; Mastoraki, S.; Strati, A.; Tzanikou, E.; Chimonidou, M.; Lianidou, E. Evaluation of Preanalytical Conditions and Implementation of Quality Control Steps for Reliable Gene Expression and DNA Methylation Analyses in Liquid Biopsies. Clin. Chem. 2018, 64, 1522–1533. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta DeltaC(T)) method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient’s ID | CTCs/7.5 mL PB (CellSearch® Analysis) | PIM-1 in CTCs | AR-V7 in CTCs | Therapy | Clinical Outcome | Death | |||
|---|---|---|---|---|---|---|---|---|---|
| Before Therapy | After Therapy | Before Treatment | After Treatment | Before Treatment | After Treatment | ||||
| P#2 | 5 | 0 | + | - | + | - | Enzalutamide | SD | No |
| P#11 | 1 | 2 | - | - | - | - | Enzalutamide | CR | No |
| P#12 | 15 | 20 | - | - | - | + | Docetaxel | PR | No |
| P#17 | 24 | 37 | - | - | + | - | Docetaxel | PR | Yes |
| P#27 | 8 | 141 | + | + | - | + | Docetaxel | PR | Yes |
| P#29 | 5 | 9 | - | - | - | - | Abiraterone | CR | No |
| P#32 | 15 | 44 | - | - | + | - | Docetaxel | PR | Yes |
| P#33 | 1 | 6 | - | + | - | - | Abiraterone | PR | Yes |
| P#34 | 18 | 0 | - | - | - | + | Abiraterone | PD | Yes |
| P#35 | 25 | 74 | - | - | - | + | Docetaxel | PR | Yes |
| P#36 | 6 | 196 | - | - | - | + | Docetaxel | PR | Yes |
| P#38 | 0 | 26 | + | - | + | + | Docetaxel | PR | Yes |
| P#39 | 87 | 145 | + | + | + | - | Docetaxel | PD | Yes |
| P#44 | 121 | 189 | - | - | + | + | Abiraterone | PD | Yes |
| PIM-1 Overexpression and/or AR-V7 Expression | Patient Status | Total | |
|---|---|---|---|
| Alive | Dead | ||
| NO | 10 (62.5%) | 6 (37.5%) | 16 |
| YES | 8 (28.6%) | 20 (71.4%) | 28 |
| Total | 18 (40.9%) | 26 (59.1%) | 44 |
| Chi-square p = 0.030 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markou, A.; Tzanikou, E.; Strati, A.; Zavridou, M.; Mastoraki, S.; Bournakis, E.; Lianidou, E. PIM-1 Is Overexpressed at a High Frequency in Circulating Tumor Cells from Metastatic Castration-Resistant Prostate Cancer Patients. Cancers 2020, 12, 1188. https://doi.org/10.3390/cancers12051188
Markou A, Tzanikou E, Strati A, Zavridou M, Mastoraki S, Bournakis E, Lianidou E. PIM-1 Is Overexpressed at a High Frequency in Circulating Tumor Cells from Metastatic Castration-Resistant Prostate Cancer Patients. Cancers. 2020; 12(5):1188. https://doi.org/10.3390/cancers12051188
Chicago/Turabian StyleMarkou, Athina, Eleni Tzanikou, Areti Strati, Martha Zavridou, Sophia Mastoraki, Evangelos Bournakis, and Evi Lianidou. 2020. "PIM-1 Is Overexpressed at a High Frequency in Circulating Tumor Cells from Metastatic Castration-Resistant Prostate Cancer Patients" Cancers 12, no. 5: 1188. https://doi.org/10.3390/cancers12051188
APA StyleMarkou, A., Tzanikou, E., Strati, A., Zavridou, M., Mastoraki, S., Bournakis, E., & Lianidou, E. (2020). PIM-1 Is Overexpressed at a High Frequency in Circulating Tumor Cells from Metastatic Castration-Resistant Prostate Cancer Patients. Cancers, 12(5), 1188. https://doi.org/10.3390/cancers12051188