
The Simpson Grading: Is It Still Valid?

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of Original Manuscript
3.2. Simpson Grade 0
3.3. Simpson Grades I–III

{kind=link}
| Author/Year/Study Design | No of Patients | Simpson Grade (SG) | RFS | Median/Mean Follow-Up Months | WHO Grades | Location | SG Associated with Recurrence |
|---|---|---|---|---|---|---|---|
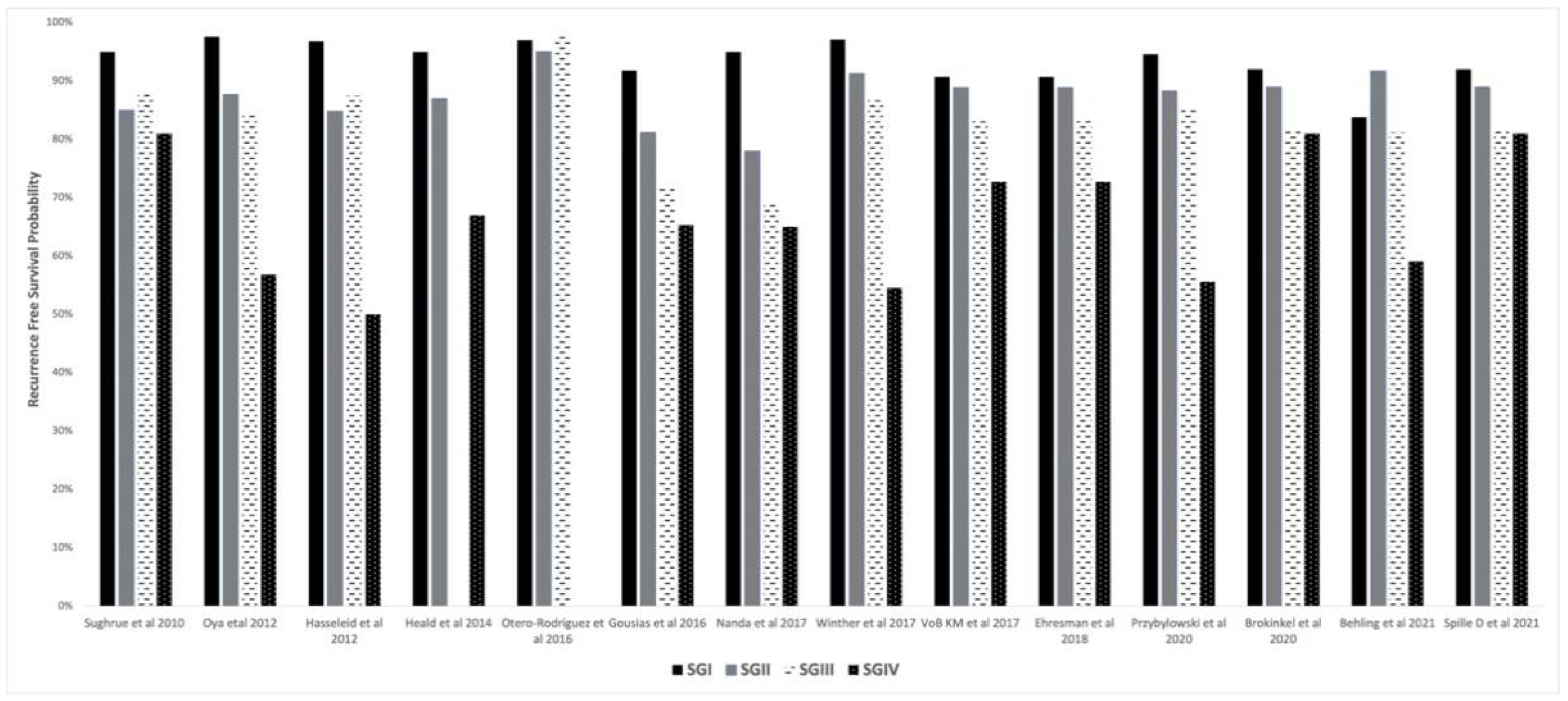
| Sughrue et al. [17] 2010 Retrospective | 373 | SG I: 88, SG II: 114, SG III: 57, SG IV: 114 | (5-yr) SG I: 95%, SG II: 85%, SG III: 88%, SG IV: 81% | 44.4 (median) (6 m–18 yrs) | I | Convexity, Skull base, parasagittal | No |
| Alvernia et al. [42] Retrospective | 100 | SG I: 91 SG II: 0 SG III: 9 | RFS NR Recurrence rate SG I: 2.2% SG IIIa: 0 SG IIIb: 22% | 86 m (median) (2–16 yrs) | I, II | Convexity | Yes |
| Oya et al. [37] 2012 Retrospective | 240 | SG I: 63, SG II: 104, SG III: 35, SG IV: 43 | (5-yr) SG I: 97.6%, SG II: 87.7%, SG III: 84.1%, SG IV: 56.8% | NR | I | Convexity, Skull base, parasagittal | SG IV: shorter RFS No difference in RFS between SG: I–III |
| Hasseleid et al. [40] 2012 Retrospective | 391 | SG I: 315, SG II: 46, SG III: 16, SG4 IV: 12, | Overall: SG I: 96.8%, SG II: 84.8%, SG III: 87.5%, SG IV: 50% | 85.2 (median) 45.6 m (6 m–108 m) | I, II, III | Convexity, excluded tumor involving sagittal sinus | Simpson II + III and IV + V had higher recurrence than Grade I |
| Heald et al. [39] 2014 Retrospective | 183 | SG I: 71, SG II: 74, SG III: 0, SG IV: 33 | (3-yr) SG I: 95%, SG II: 87%, SG III: NA, SG IV: 67% | 35.3 (mean) (6 m–81.6 m) | I | Convexity, Skull base, parasagittal | Yes |
| Otero-Rodriguez et al. [10] 2016 Retrospective | 224 | SG I: 54, SG II: 86, SG III: 84 | (5-yr) SG I: 97%, SG II: 95%, SG III: 98%, | 60 (median) (NR) | I | Convexity, Skull base, parasagittal | No difference in recurrence rates between SG I–III |
| Gousias et al. [43] 2016 Retrospective | 901 | SG I: 570, SG II: 197, SG III: 92, SG IV: 35 | (10-yr) SG I: 91.8%, SG II: 81.2%, SG III: 71.8%, SG IV: 65.3% | 62 (median) (NR) | I, II, III | Convexity, Skull base, parasagittal | Yes |
| Nanda et al. [41] 2017 Retrospective | 458 | SG I: 80, SG II: 294, SG III: 32, SG IV: 52 | Overall SG I: 95%, SG II: 78%, SG III: 69%, SG IV: 65% | 54 (mean) (1 m–250 m) | I | Convexity, Skull base | Yes |
| Winther et al. [16] 2017 Retrospective | 113 | SG I: 35, SG II: 48, SG III: 16, SG IV: 14 | (5-yr) SG I: 97.1%, SG II: 91.3%, SG III: 86.7%, SG IV: 54.5% | 123 (median) (6.9 m–210.6 m) | I | Convexity, Skull base, parasagittal | Yes |
| Ehresman et al. [36] 2018 Retrospective | 572 | SG I: 125, SG II: 197, SG III: 92, SG IV: 158 | (4-yr) SG I: 90.7%, SG II: 88.9%, SG III: 83.8%, SG IV: 72.7% | 53.9 m (median) (24 m–83.9 m) | I, II, III | Convexity, Skull base, parasagittal | No. No difference between SG I and II. |
| VoB KM et al. [15] 2017 Retrospective | 826 | SG I: 238, SG II: 343, SG III: 102, SG IV: 79 | SG I: 90.7%, SG II: 88.9%, SG III: 83.8%, SG IV: 72.7% | 50 m (median) (0–277 m) | I, II, III | Convexity, Skull base, parasagittal | No difference in recurrence between I, II and III, increased risk after IV. |
| Przybylowski et al. [11] 2020 Retrospective | 492 | SG I: 97, SG II: 142, SG III: 50, SG IV: 152 | (5-yr) SG I: 94.6%, SG II: 88.3%, SG III: 85.1%, SG IV: 55.6%, SG IV with radiosurgery: 85% | 44.8 (mean) (SD:30.5) | I | Convexity, Skull base, parasagittal | Yes |
| Brokinkel et al. [6] 2020 Retrospective | 939 | SG I: 280, SG II: 446, SG III: 103, SG IV: 106 | SG I: 92%, SG II: 89%, SG III: 82%, SG IV: 81% | 37 m (median) (0–284 m) | I, II, III | Convexity, Skull base, parasagittal | Yes, the predictive value of SG is higher when dichotomizing into Grades I–III compared to I–II. |
| Behling et al. [5] 2021 Retrospective | 1571 | SG I: 376, SG II: 408, SG III: 303, SG IV: 484 | SG I: 83.8%, SG II: 91.7%, SG III: 81.2%, SG IV: 59.1% | 38.4 (mean) (1.2 m–195.6 m) | I, II, III | Convexity, Skull base, Parasagittal, Spinal | No |
| Spille D et al. [14] 2021 Retrospective | 939 | SG I: 280, SG II: 446, SG III: 103, SG IV: 106 | SG I: 92%, SG II: 89%, SG III: 82%, SG IV: 81% | 37 m (median) (NR) | I, II, III | Convexity, Skull base | Yes. Postoperative tumor volume predicts the risk of recurrence more relevantly than the Simpson Grade |
3.4. Simpson Grade IV–V
3.5. Simpson Grade and WHO Grade
3.6. Intraoperative Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Apra, C.; Peyre, M.; Kalamarides, M. Current treatment options for meningioma. Expert Rev. Neurother. 2018, 18, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and etiology of meningioma. J. Neuro-Oncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achey, R.L.; Gittleman, H.; Schroer, J.; Khanna, V.; Kruchko, C.; Barnholtz-Sloan, J. Nonmalignant and malignant meningioma incidence and survival in the elderly, 2005–2015, using the Central Brain Tumor Registry of the United States. Neuro-Oncology 2019, 21, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [Green Version]
- Behling, F.; Fodi, C.; Hoffmann, E.; Renovanz, M.; Skardelly, M.; Tabatabai, G.; Schittenhelm, J.; Honegger, J.; Tatagiba, M. The role of Simpson grading in meningiomas after integration of the updated WHO classification and adjuvant radiotherapy. Neurosurg. Rev. 2021, 44, 2329–2336. [Google Scholar] [CrossRef]
- Brokinkel, B.; Spille, D.C.; Brokinkel, C.; Hess, K.; Paulus, W.; Bormann, E.; Stummer, W. The Simpson grading: Defining the optimal threshold for gross total resection in meningioma surgery. Neurosurg. Rev. 2021, 44, 1713–1720. [Google Scholar] [CrossRef]
- Dedeciusova, M.; Majovsky, M.; Pecen, L.; Benes, V.; Netuka, D. Long-term outcome of Simpson IV meningioma resection: Would it improve with adjuvant SRS? Clin. Neurol. Neurosurg. 2021, 207, 106766. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef] [Green Version]
- Kinjo, T.; Al-Mefty, O.; Kanaan, I. Grade Zero Removal of Supratentorial Convexity Meningiomas. Neurosurgery 1993, 33, 394–399. [Google Scholar] [CrossRef]
- Otero-Rodriguez, A.; Tabernero, M.D.; Munoz-Martin, M.C.; Sousa, P.; Orfao, A.; Pascual-Argente, D.; Gonzalez-Tablas, M.; Ruiz-Martin, L. Re-Evaluating Simpson Grade I, II, and III Resections in Neurosurgical Treatment of World Health Organization Grade I Meningiomas. World Neurosurg. 2016, 96, 483–488. [Google Scholar] [CrossRef]
- Przybylowski, C.J.; Hendricks, B.K.; Frisoli, F.A.; Zhao, X.; Cavallo, C.; Moreira, L.B.; Gandhi, S.; Sanai, N.; Almefty, K.K.; Lawton, M.T.; et al. Prognostic value of the Simpson grading scale in modern meningioma surgery: Barrow Neurological Institute experience. J. Neurosurg. 2021, 135, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, B.I.; McDermott, M.W.; Schwartz, T.H. Letter to the Editor. Time to move beyond the Simpson scale in meningioma surgery. J. Neurosurg. 2021, 135, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, T.H.; McDermott, M.W. The Simpson grade: Abandon the scale but preserve the message. J. Neurosurg. 2021, 135, 488–495. [Google Scholar] [CrossRef]
- Spille, D.C.; Hess, K.; Bormann, E.; Sauerland, C.; Brokinkel, C.; Warneke, N.; Mawrin, C.; Paulus, W.; Stummer, W.; Brokinkel, B. Risk of tumor recurrence in intracranial meningiomas: Comparative analyses of the predictive value of the postoperative tumor volume and the Simpson classification. J. Neurosurg. 2021, 134, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Voß, K.M.; Spille, D.C.; Sauerland, C.; Molina, E.S.; Brokinkel, C.; Paulus, W.; Stummer, W.; Holling, M.; Jeibmann, A.; Brokinkel, B. The Simpson grading in meningioma surgery: Does the tumor location influence the prognostic value? J. Neuro-Oncol. 2017, 133, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Winther, T.L.; Torp, S.H. Significance of the Extent of Resection in Modern Neurosurgical Practice of World Health Organization Grade I Meningiomas. World Neurosurg. 2016, 99, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Sughrue, M.E.; Kane, A.J.; Shangari, G.; Rutkowski, M.J.; McDermott, M.W.; Berger, M.S.; Parsa, A.T. The relevance of Simpson Grade I and II resection in modern neurosurgical treatment of World Health Organization Grade I meningiomas. J. Neurosurg. 2010, 113, 1029–1035. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Mirian, C.; Skyrman, S.; Bartek, J.; Jensen, L.R.; Kihlström, L.; Förander, P.; Orrego, A.; Mathiesen, T. The Ki-67 Proliferation Index as a Marker of Time to Recurrence in Intracranial Meningioma. Neurosurgery 2020, 87, 1289–1298. [Google Scholar] [CrossRef]
- Behling, F.; Hempel, J.-M.; Schittenhelm, J. Brain Invasion in Meningioma—A Prognostic Potential Worth Exploring. Cancers 2021, 13, 3259. [Google Scholar] [CrossRef]
- Nakasu, S.; Nakasu, Y. Prognostic significance of brain invasion in meningiomas: Systematic review and meta-analysis. Brain Tumor Pathol. 2021, 38, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Sahm, F.; Schrimpf, D.; Stichel, D.; Jones, D.T.W.; Hielscher, T.; Schefzyk, S.; Okonechnikov, K.; Koelsche, C.; Reuss, D.E.; Capper, D.; et al. DNA methylation-based classification and grading system for meningioma: A multicentre, retrospective analysis. Lancet Oncol. 2017, 18, 682–694. [Google Scholar] [CrossRef] [Green Version]
- Qi, S.-T.; Liu, Y.; Pan, J.; Chotai, S.; Fang, L.-X. A radiopathological classification of dural tail sign of meningiomas. J. Neurosurg. 2012, 117, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, F.; Yoshioka, H.; Hama, S.; Sugiyama, K.; Arita, K.; Kurisu, K. Recurrence of meningiomas. Cancer 2000, 89, 1102–1110. [Google Scholar] [CrossRef]
- Borovich, B.; Doron, Y. Recurrence of intracranial meningiomas: The role played by regional multicentricity. J. Neurosurg. 1986, 64, 58–63. [Google Scholar] [CrossRef]
- Borovich, B.; Doron, Y.; Braun, J.; Guilburd, J.N.; Zaaroor, M.; Goldsher, D.; Lemberger, A.; Gruszkiewicz, J.; Feinsod, M. Recurrence of intracranial meningiomas: The role played by regional multicentricity. Part 2: Clinical and radiological aspects. J. Neurosurg. 1986, 65, 168–171. [Google Scholar] [CrossRef]
- Morokoff, A.P.; Zauberman, J.; Black, P.M. Surgery for convexity meningiomas. Neurosurgery 2008, 63, 427–433; discussion 433–424. [Google Scholar] [CrossRef] [Green Version]
- Keskil, S.; Bademci, G.; Goksel, M. Tracing the Dural Tail with Image-Guided Surgery. Minim. Invasive Neurosurg. 2006, 49, 357–358. [Google Scholar] [CrossRef]
- Nakau, H.; Miyazawa, T.; Tamai, S.; Tsuchiya, K.; Shima, K.; Shirotani, T.; Chigasaki, H. Pathologic Significance of Meningeal Enhancement (“Flare Sign”) of Meningiomas on MRI. Surg. Neurol. 1997, 48, 584–591. [Google Scholar] [CrossRef]
- Murase, M.; Tamura, R.; Kuranari, Y.; Sato, M.; Ohara, K.; Morimoto, Y.; Yoshida, K.; Toda, M. Novel histopathological classification of meningiomas based on dural invasion. J. Clin. Pathol. 2021, 74, 238–243. [Google Scholar] [CrossRef]
- Nagashima, G.; Fujimoto, T.; Suzuki, R.; Asai, J.-I.; Itokawa, H.; Noda, M. Dural invasion of meningioma: A histological and immunohistochemical study. Brain Tumor Pathol. 2006, 23, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Linsler, S.; Ketter, R.; Oertel, J.; Urbschat, S. Fluorescence imaging of meningioma cells with somatostatin receptor ligands: An in vitro study. Acta Neurochir. 2019, 161, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yang, W.; Deng, J.; Zhang, J.; Ma, F.; Wang, J. Correlation between 99mTc-HYNIC-octreotide SPECT/CT somatostatin receptor scintigraphy and pathological grading of meningioma. J. Neuro-Oncol. 2013, 113, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Jelke, F.; Mirizzi, G.; Borgmann, F.K.; Husch, A.; Slimani, R.; Klamminger, G.G.; Klein, K.; Mombaerts, L.; Gérardy, J.-J.; Mittelbronn, M.; et al. Intraoperative discrimination of native meningioma and dura mater by Raman spectroscopy. Sci. Rep. 2021, 11, 23583. [Google Scholar] [CrossRef] [PubMed]
- Koljenović, S.; Schut, T.B.; Vincent, A.; Kros, J.M.; Puppels, G.J. Detection of Meningioma in Dura Mater by Raman Spectroscopy. Anal. Chem. 2005, 77, 7958–7965. [Google Scholar] [CrossRef]
- Ehresman, J.S.; Garzon-Muvdi, T.; Rogers, D.; Lim, M.; Gallia, G.L.; Weingart, J.; Brem, H.; Bettegowda, C.; Chaichana, K.L. The Relevance of Simpson Grade Resections in Modern Neurosurgical Treatment of World Health Organization Grade I, II, and III Meningiomas. World Neurosurg. 2018, 109, e588–e593. [Google Scholar] [CrossRef]
- Oya, S.; Kawai, K.; Nakatomi, H.; Saito, N. Significance of Simpson grading system in modern meningioma surgery: Integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO Grade I meningiomas. J. Neurosurg. 2012, 117, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, M.J.; Jenkinson, M.D.; Brodbelt, A.R.; Mills, S.J.; Chavredakis, E. WHO grade 1 meningioma recurrence: Are location and Simpson grade still relevant? Clin. Neurol. Neurosurg. 2016, 141, 117–121. [Google Scholar] [CrossRef]
- Heald, J.B.; Carroll, T.A.; Mair, R.J. Simpson grade: An opportunity to reassess the need for complete resection of meningiomas. Acta Neurochir. 2014, 156, 383–388. [Google Scholar] [CrossRef]
- Hasseleid, B.F.; Meling, T.R.; Rønning, P.; Scheie, D.; Helseth, E. Surgery for convexity meningioma: Simpson Grade I resection as the goal: Clinical article. J. Neurosurg. 2012, 117, 999–1006. [Google Scholar] [CrossRef]
- Nanda, A.; Bir, S.C.; Maiti, T.K.; Konar, S.K.; Missios, S.; Guthikonda, B. Relevance of Simpson grading system and recurrence-free survival after surgery for World Health Organization Grade I meningioma. J. Neurosurg. 2017, 126, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Alvernia, J.E.; Dang, N.D.; Sindou, M.P. Convexity meningiomas: Study of recurrence factors with special emphasis on the cleavage plane in a series of 100 consecutive patients. J. Neurosurg. 2011, 115, 491–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gousias, K.; Schramm, J.; Simon, M. The Simpson grading revisited: Aggressive surgery and its place in modern meningioma management. J. Neurosurg. 2016, 125, 551–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, M.; Gallieni, M.; Metwali, H.; Fahlbusch, R.; Samii, M.; Samii, A. Can Intraoperative Magnetic Resonance Imaging Be Helpful in the Surgical Resection of Parasellar Meningiomas? A Case Series. World Neurosurg. 2019, 132, e577–e584. [Google Scholar] [CrossRef]
- Fukushima, Y.; Oya, S.; Nakatomi, H.; Shibahara, J.; Hanakita, S.; Tanaka, S.; Shin, M.; Kawai, K.; Fukayama, M.; Saito, N. Effect of dural detachment on long-term tumor control for meningiomas treated using Simpson Grade IV resection: Clinical article. J. Neurosurg. 2013, 119, 1373–1379. [Google Scholar] [CrossRef]
- Materi, J.; Mampre, D.; Ehresman, J.; Rincon-Torroella, J.; Chaichana, K.L. Predictors of recurrence and high growth rate of residual meningiomas after subtotal resection. J. Neurosurg. 2021, 134, 410–416. [Google Scholar] [CrossRef]
- Terpolilli, N.A.; Rachinger, W.; Kunz, M.; Thon, N.; Flatz, W.H.; Tonn, J.-C.; Schichor, C. Orbit-associated tumors: Navigation and control of resection using intraoperative computed tomography. J. Neurosurg. 2016, 124, 1319–1327. [Google Scholar] [CrossRef] [Green Version]
- Schulder, M.; Jacobs, A.; Carmel, P.W. Intraoperative MRI and adjuvant radiosurgery. Ster. Funct. Neurosurg. 2001, 76, 151–158. [Google Scholar] [CrossRef]
- Charalampaki, P.; Proskynitopoulos, P.J.; Heimann, A.; Nakamura, M. 5-Aminolevulinic Acid Multispectral Imaging for the Fluorescence-Guided Resection of Brain Tumors: A Prospective Observational Study. Front. Oncol. 2020, 10, 1069. [Google Scholar] [CrossRef]
- Multani, K.M.; Balasubramaniam, A.; Rajesh, B.J.; Kumar, M.S.; Manohara, N.; Kumar, A. Utility and pitfalls of high field 3 tesla intraoperative mri in neurosurgery: A single centre experience of 100 cases. Neurol. India 2020, 68, 413–418. [Google Scholar] [CrossRef]
- Adeolu, A.A.; Sutherland, G.R. Intraoperative magnetic resonance imaging and meningioma surgery. West Afr. J. Med. 2006, 25, 174–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuleasca, C.; Aboukais, R.; Vannod-Michel, Q.; Leclerc, X.; Reyns, N.; Lejeune, J.-P. Intraoperative MRI for the microsurgical resection of meningiomas close to eloquent areas or dural sinuses: Patient series. J. Neurosurg. Case Lessons 2021, 1, CASE20149. [Google Scholar] [CrossRef]
- Ashour, R.; Reintjes, S.; Park, M.S.; Sivakanthan, S.; Van Loveren, H.; Agazzi, S. Intraoperative Magnetic Resonance Imaging in Skull Base Surgery: A Review of 71 Consecutive Cases. World Neurosurg. 2016, 93, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Soleman, J.; Fathi, A.-R.; Marbacher, S.; Fandino, J. The role of intraoperative magnetic resonance imaging in complex meningioma surgery. Magn. Reson. Imaging 2013, 31, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, B.M.; Jeltema, H.-R.; Kruijff, S.; Groen, R.J.M. The application of fluorescence techniques in meningioma surgery—A review. Neurosurg. Rev. 2019, 42, 799–809. [Google Scholar] [CrossRef] [Green Version]
- Kajimoto, Y.; Kuroiwa, T.; Miyatake, S.-I.; Ichioka, T.; Miyashita, M.; Tanaka, H.; Tsuji, M. Use of 5-aminolevulinic acid in fluorescence-guided resection of meningioma with high risk of recurrence. Case report. J. Neurosurg. 2007, 106, 1070–1074. [Google Scholar] [CrossRef]
- Morofuji, Y.; Matsuo, T.; Hayashi, Y.; Suyama, K.; Nagata, I. Usefulness of Intraoperative Photodynamic Diagnosis Using 5-Aminolevulinic Acid for Meningiomas with Cranial Invasion: Technical Case Report. Neurosurgery 2008, 62, 102–103; discussion 103–104. [Google Scholar] [CrossRef]
- Youngblood, M.W.; Miyagishima, D.F.; Jin, L.; Gupte, T.; Li, C.; Duran, D.; Montejo, J.D.; Zhao, A.; Sheth, A.; Tyrtova, E.; et al. Associations of meningioma molecular subgroup and tumor recurrence. Neuro-Oncology 2021, 23, 783–794. [Google Scholar] [CrossRef]
- Rogers, C.L.; Won, M.; Vogelbaum, M.A.; Perry, A.; Ashby, L.S.; Modi, J.M.; Alleman, A.M.; Galvin, J.; Fogh, S.E.; Youssef, E.; et al. High-risk Meningioma: Initial Outcomes from NRG Oncology/RTOG 0539. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 790–799. [Google Scholar] [CrossRef]
- Rogers, L.; Barani, I.; Chamberlain, M.; Kaley, T.J.; McDermott, M.; Raizer, J.; Schiff, D.; Weber, D.C.; Wen, P.Y.; Vogelbaum, M.A. Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review. J. Neurosurg. 2015, 122, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Hemmati, S.M.; Ghadjar, P.; Grün, A.; Badakhshi, H.; Zschaeck, S.; Senger, C.; Acker, G.; Misch, M.; Budach, V.; Kaul, D. Adjuvant radiotherapy improves progression-free survival in intracranial atypical meningioma. Radiat. Oncol. 2019, 14, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Broi, M.; Borrelli, P.; Meling, T. Predictors of Survival in Atypical Meningiomas. Cancers 2021, 13, 1970. [Google Scholar] [CrossRef] [PubMed]

| Grade | Definition | Number of Patients Treated | Recurrence as Reported |
|---|---|---|---|
| I | Macroscopic complete tumor resection with removal of affected dura and bone, when tumor arises from wall of dural venous sinus such an operation necessities resection of the sinus | 90 | (9%) |
| II | Macroscopic complete tumor resection and of its visible extension with coagulation of affected dura | 114 | 18 (19%) |
| III | Macroscopic complete tumor removal | 24 | 8 (29%) |
| IV | Partial resection, leaving intradural tumor in situ | 51 | 20 (39%) |
| V | Decompression with/without biopsy | 9 | 8 (88.9%) |
| Author, Year, Study Design | Number of Tumors Treated | Location | iMRI/iCT Scan Utility | Impact of Intraoperative Imaging on Simpson Grade |
|---|---|---|---|---|
| Giordano et al. [44] 2019 Prospective | 19 | Parasellar | iMRI allowed the further safe resection in 56% of cases and offered a better precondition for radiotherapy. Increased EOR for 2/5 tuberculum sellae meningioma, an 5/9 cavernous sinus meningioma. | No change in Simpson Grade |
| Multani et al. [50] 2020 Retrospective | 11 | NA | 5/11 (45.5%) iMRI detected residue and 3/5 additional resection was achieved | No mention of Simpson Grades |
| Ashour R et al. [53] 2016 Retrospective | 10 | Skull base | Additional resection in 4 meningiomas | No mention of Simpson Grades |
| Terpolilli et al. [47] 2016 Retrospective | 19 | Orbital meningioma | Intraoperative CT was used to evaluate the residual osseus part and therefore allowed for sufficient decompression of optic nerve in 52% of cases. | No mention of Simpson Grades |
| Soleman et al. [54] 2012 Retrospective | 27 | Skull base | Only one patient (3.4%) underwent resection of tumor remnant after iMRI, although without improvement of the Simpson resection Grade. | No change in Simpson Grade |
| Schulder et al. [48] 2001 Retrospective | 4 | Skull base | Amount of residual tumor was optimized for SRS | No change in Simpson Grade |
| Tuleasca C et al. [52] 2021 Case series | 6 | Eloquent areas, or dural sinus | Useful to increase EOR and reduce residual volume | GTR achieved after iMRI use in at least 2/6 patients. No change in EOR for 1 patient, other details not reported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chotai, S.; Schwartz, T.H. The Simpson Grading: Is It Still Valid? Cancers 2022, 14, 2007. https://doi.org/10.3390/cancers14082007
Chotai S, Schwartz TH. The Simpson Grading: Is It Still Valid? Cancers. 2022; 14(8):2007. https://doi.org/10.3390/cancers14082007
Chicago/Turabian StyleChotai, Silky, and Theodore H. Schwartz. 2022. "The Simpson Grading: Is It Still Valid?" Cancers 14, no. 8: 2007. https://doi.org/10.3390/cancers14082007
APA StyleChotai, S., & Schwartz, T. H. (2022). The Simpson Grading: Is It Still Valid? Cancers, 14(8), 2007. https://doi.org/10.3390/cancers14082007