Efficacy of the Newly Invented Eyelid Clamper in Ultra-Widefield Fundus Imaging


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
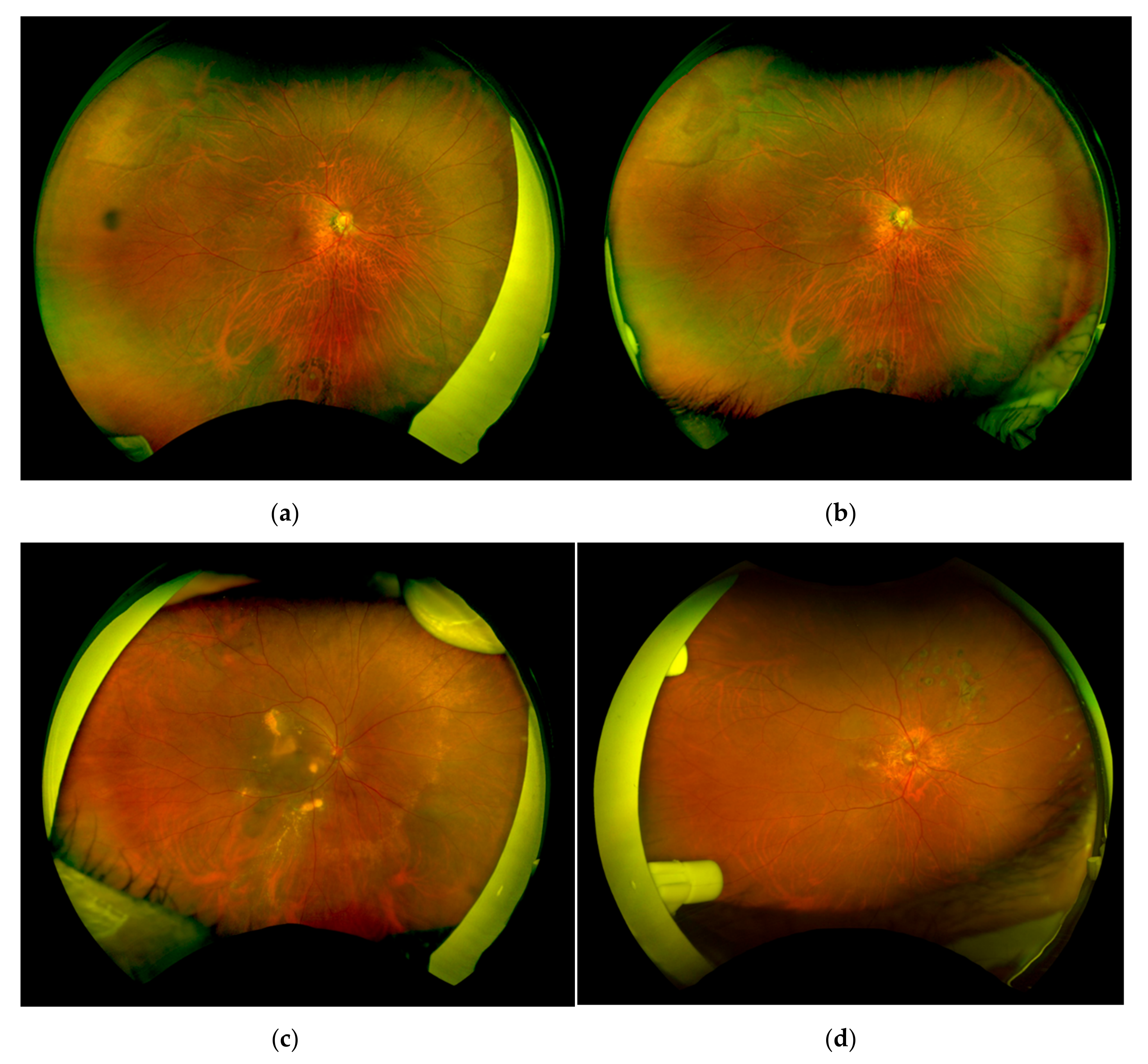
2.1. Patients and Image Acquisition
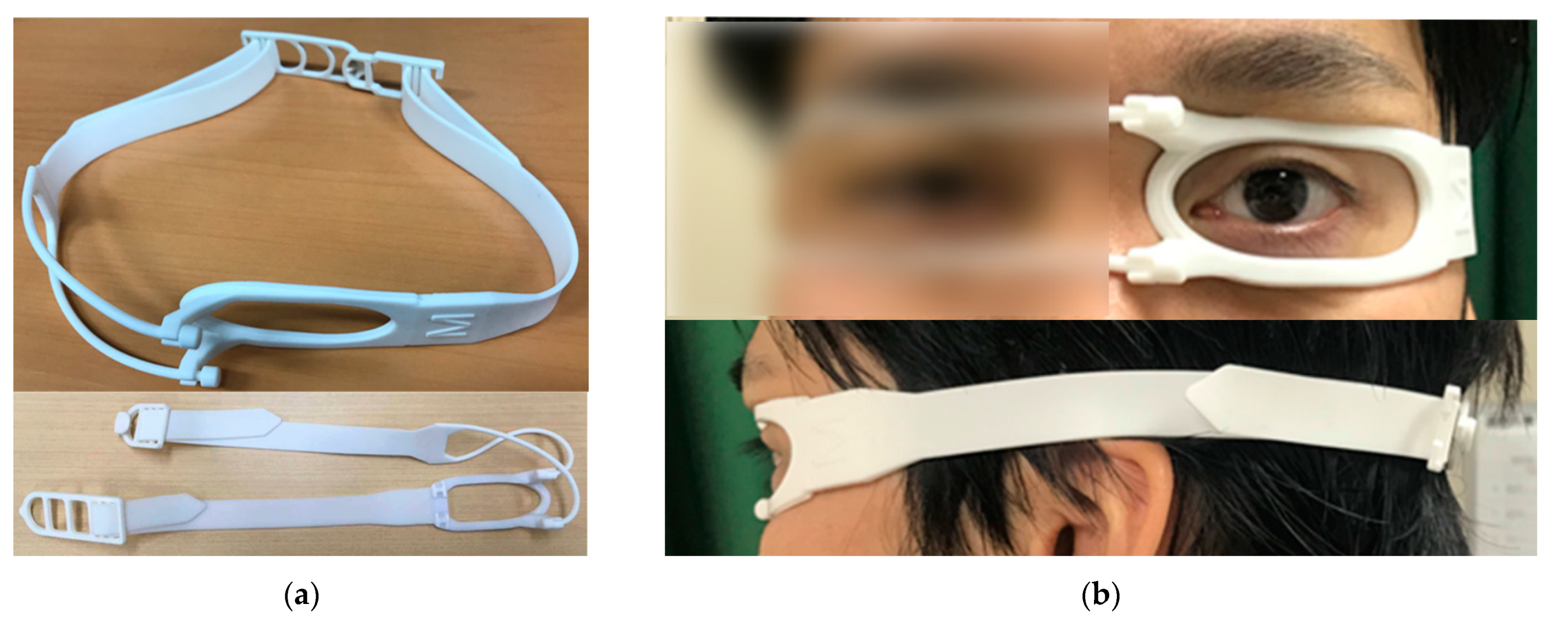
2.2. Eyelid Clamper
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mackenzie, P.J.; Russell, M.; Ma, P.E.; Isbister, C.M.; Maberley, D.A.L. Sensitivity and specificity of the Optos Optomap for detecting peripheral retinal lesions. Retina 2007, 27, 1119–1124. [Google Scholar] [CrossRef]
- Bonnay, G.; Nguyen, F.; Meunier, I.; Ducasse, A.; Hamel, C.; Arndt, C. Screening for retinal detachment using wide-field retinal imaging. J. Fr. Ophtalmol. 2011, 34, 482–485. [Google Scholar] [CrossRef]
- Wessel, M.M.; Aaker, G.D.; Parlitsis, G.; Cho, M.; Amico, D.J.D. Improves the Detection and Classification of Diabetic Retinopathy. Retina 2012, 32, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Nagiel, A.; Lalane, R.A.; Sadda, S.R.; Schwartz, S.D. Ultra-widefield fundus imaging: A review of clinical applications and future trends. Retina 2016, 36, 660–678. [Google Scholar] [CrossRef]
- Spaide, R.F. Erratum: Peripheral areas of nonperfusion in treated central retinal vein occlusion as imaged by wide-field fluorescein angiography. Retina 2011, 31, 829–837. [Google Scholar] [CrossRef]
- Hirano, T.; Imai, A.; Kasamatsu, H.; Kakihara, S.; Toriyama, Y.; Murata, T. Assessment of diabetic retinopathy using two ultra-wide-field fundus imaging systems, the Clarus® and OptosTM systems. BMC Ophthalmol. 2018, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.C.K.; Yap, M.K.H.; Goldschmidt, E.; Swann, P.G.; Ng, L.H.Y.; Lam, C.S.Y. Use of the Optomap with lid retraction and its sensitivity and specificity. Clin. Exp. Optom. 2008, 91, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaka, S.; Yamamoto, M.; Santou, M.; Ookado, S.; Yokoyama, J.; Imai, D.; Kita, M. Evaluation of the Methods to Eliminate Lash effect during Fundus Imaging with Ultra-wide-angle Scanning Laser Ophthalmoscope. Jpn. Orthopt. J. 2015, 44, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Inoue, M.; Yanagawa, A.; Yamane, S.; Arakawa, A.; Kawai, Y.; Kadonosono, K. Wide-field fundus imaging using the optos optomap and a disposable eyelid speculum. JAMA Ophthalmol. 2013, 131, 226–227. [Google Scholar] [CrossRef]
- Witmer, M.T.; Parlitsis, G.; Patel, S.; Kiss, S. Comparison of ultra-widefield fluorescein angiography with the Heidelberg Spectralis® noncontact ultra-widefield module versus the Optos® Optomap®. Clin. Ophthalmol. 2013, 7, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Friberg, T.; Labriola, L. Medical Retina: Focus on Retinal Imaging; Frank, G.H., Richard, F.S., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; Chapter 4; ISBN 3662502089. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Results |
|---|---|
| Face pain scale while wearing the eyelid clamper | 1.13 ± 1.35 |
| Face pain scale after wearing the eyelid clamper | 0.10 ± 0.31 |
| Location of the pain | Both temples in 3 patients |
| The lower eyelid in 2 patients | |
| Around the nose in 1 patient | |
| The examined eye in 4 patients |
| Tape | Eyelid Clamper | Conventional Eyelid Speculum | |
|---|---|---|---|
| Topical anesthesia | - | - | + |
| Pain | Caused by adhesion | Mostly by pressure of the band | Cannot be done without anesthesia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozawa, N.; Mori, K.; Katada, Y.; Tsubota, K.; Kurihara, T. Efficacy of the Newly Invented Eyelid Clamper in Ultra-Widefield Fundus Imaging. Life 2020, 10, 323. https://doi.org/10.3390/life10120323
Ozawa N, Mori K, Katada Y, Tsubota K, Kurihara T. Efficacy of the Newly Invented Eyelid Clamper in Ultra-Widefield Fundus Imaging. Life. 2020; 10(12):323. https://doi.org/10.3390/life10120323
Chicago/Turabian StyleOzawa, Nobuhiro, Kiwako Mori, Yusaku Katada, Kazuo Tsubota, and Toshihide Kurihara. 2020. "Efficacy of the Newly Invented Eyelid Clamper in Ultra-Widefield Fundus Imaging" Life 10, no. 12: 323. https://doi.org/10.3390/life10120323
APA StyleOzawa, N., Mori, K., Katada, Y., Tsubota, K., & Kurihara, T. (2020). Efficacy of the Newly Invented Eyelid Clamper in Ultra-Widefield Fundus Imaging. Life, 10(12), 323. https://doi.org/10.3390/life10120323