Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma?

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Characteristic of Patients
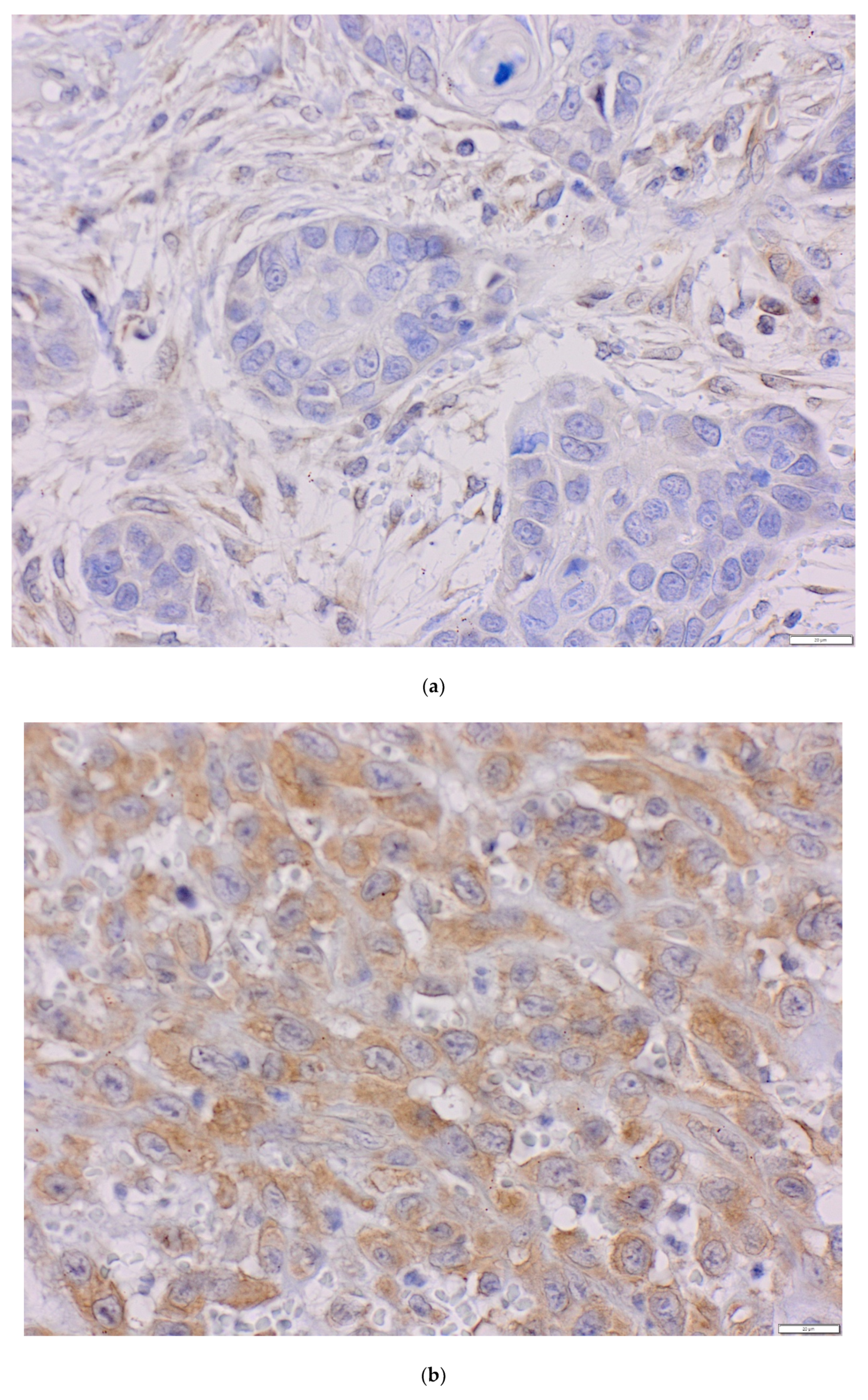
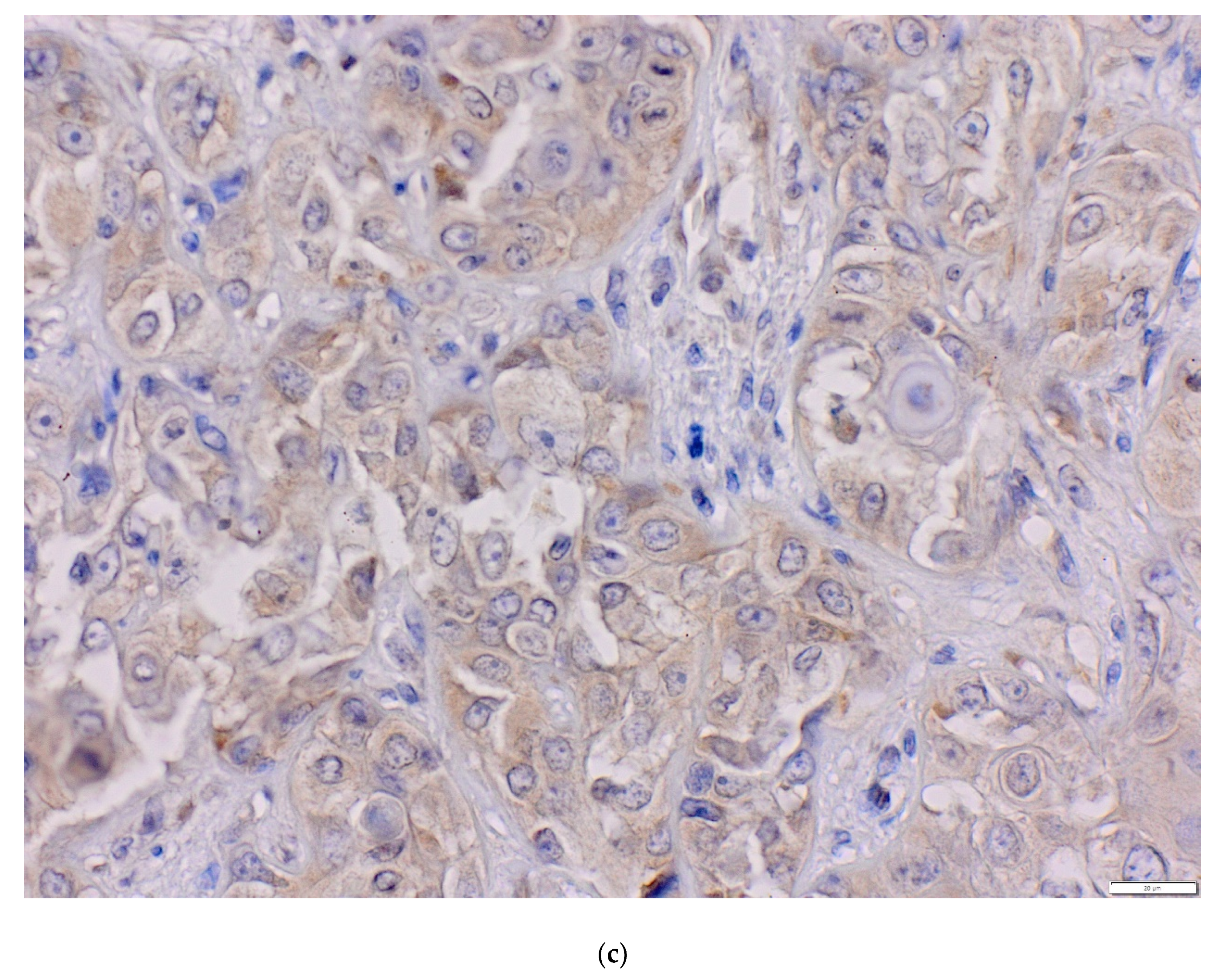
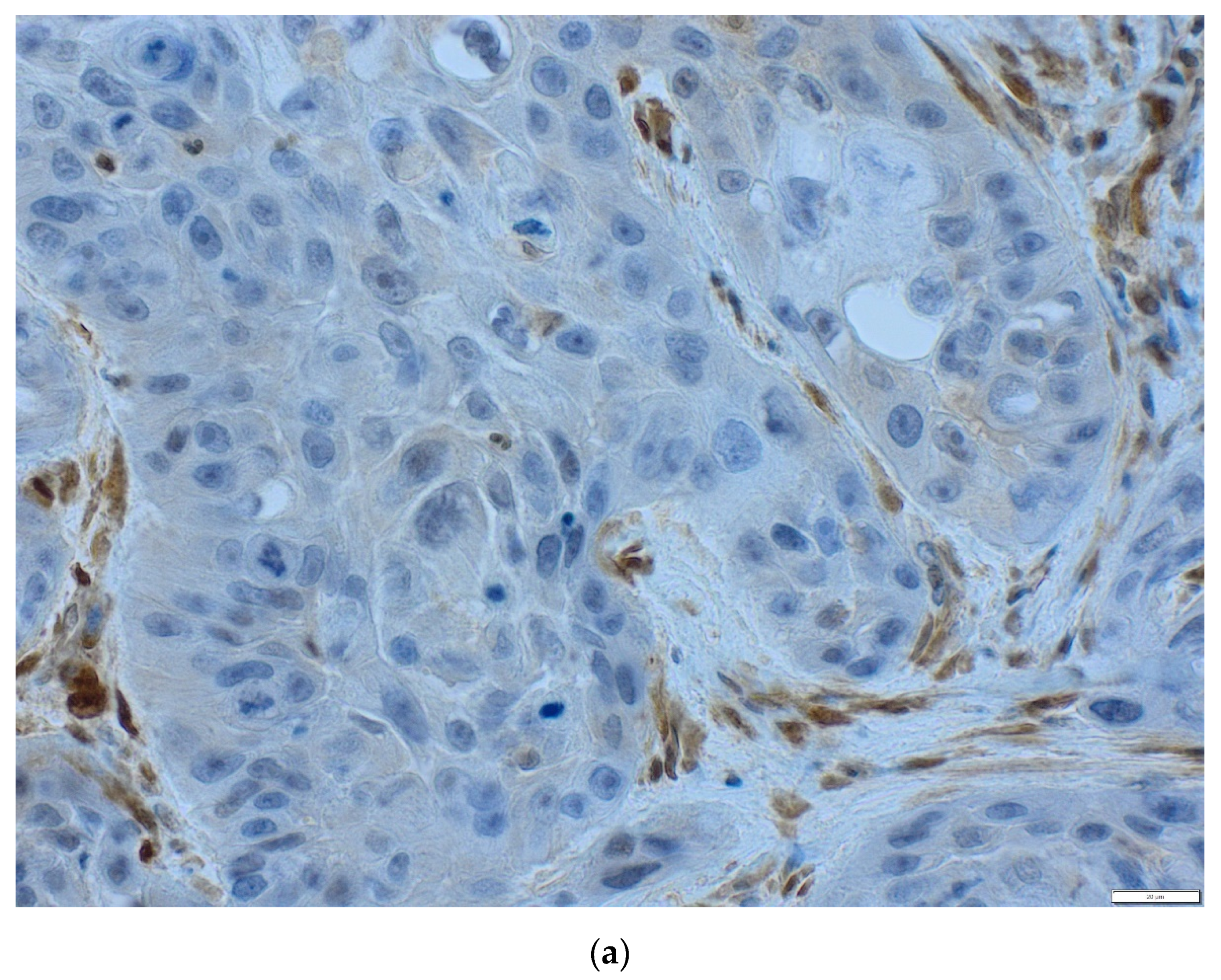
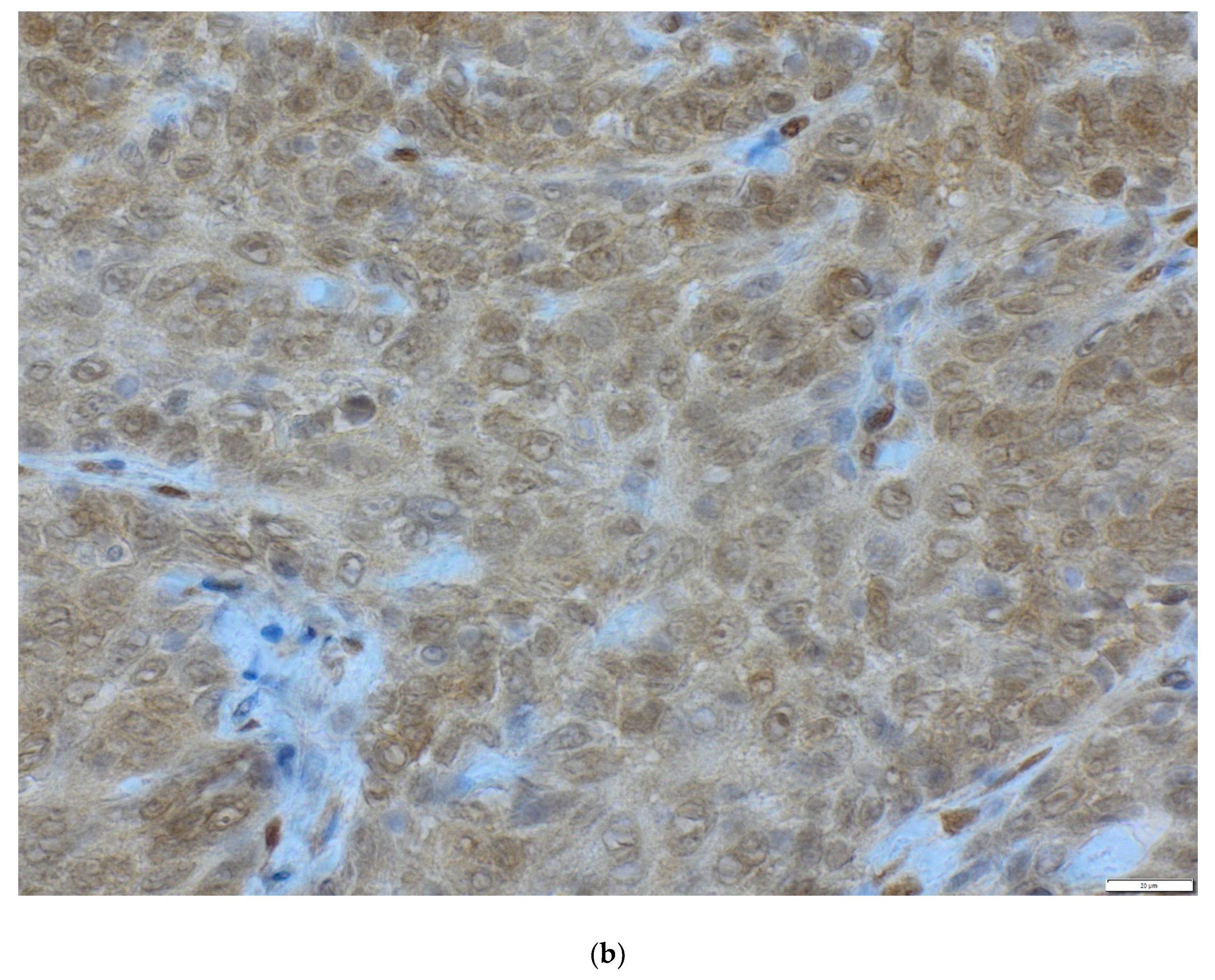
2.2. Immunohistochemistry Assessment of PIK3CA and PTEN Protein
2.2.1. PIK3CA Protein
2.2.2. PTEN Protein
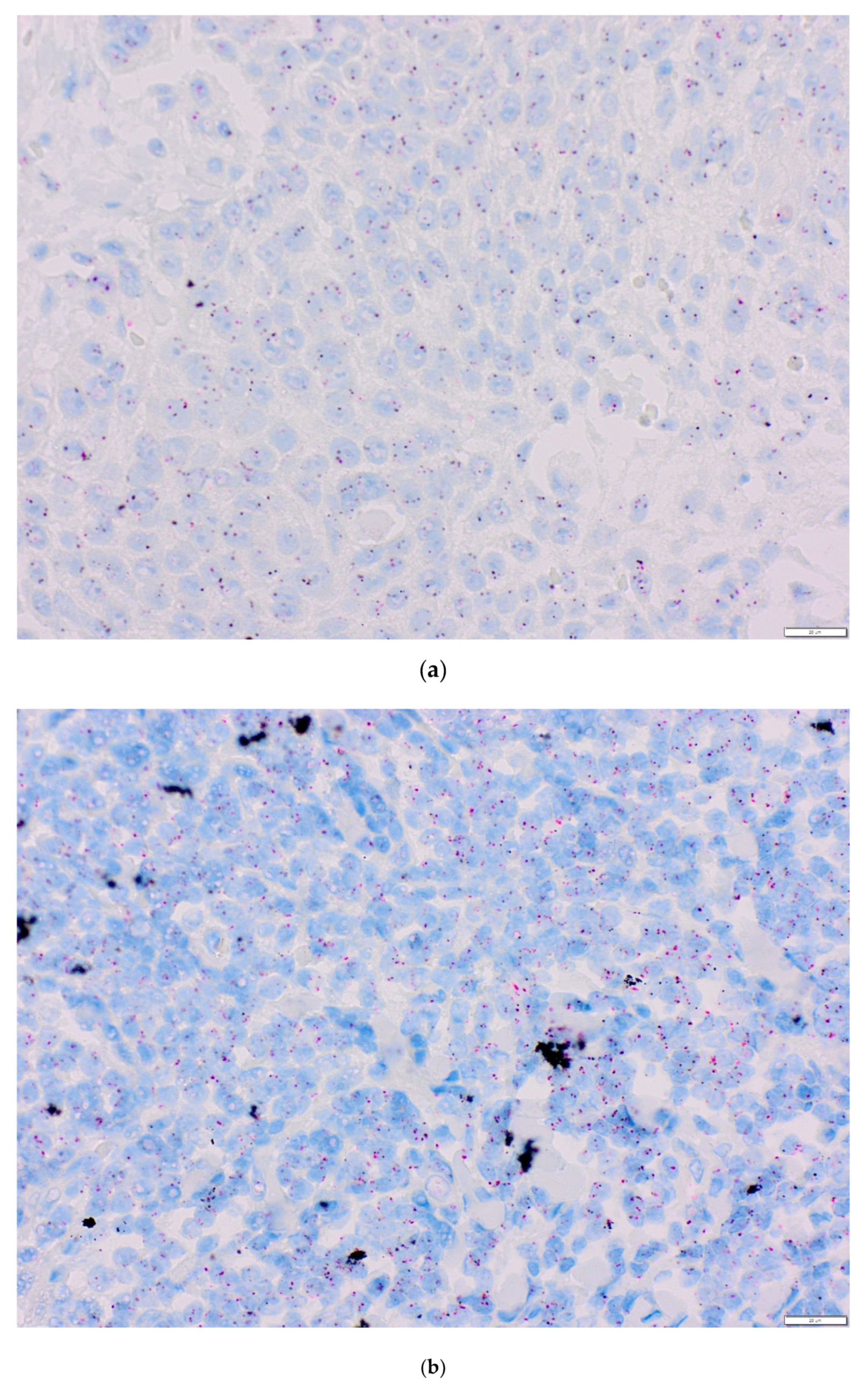
2.3. Analysis of the PIK3CA Gene Copy Number Using Chromogenic and Silver In Situ Hybridization (CISH/SISH)
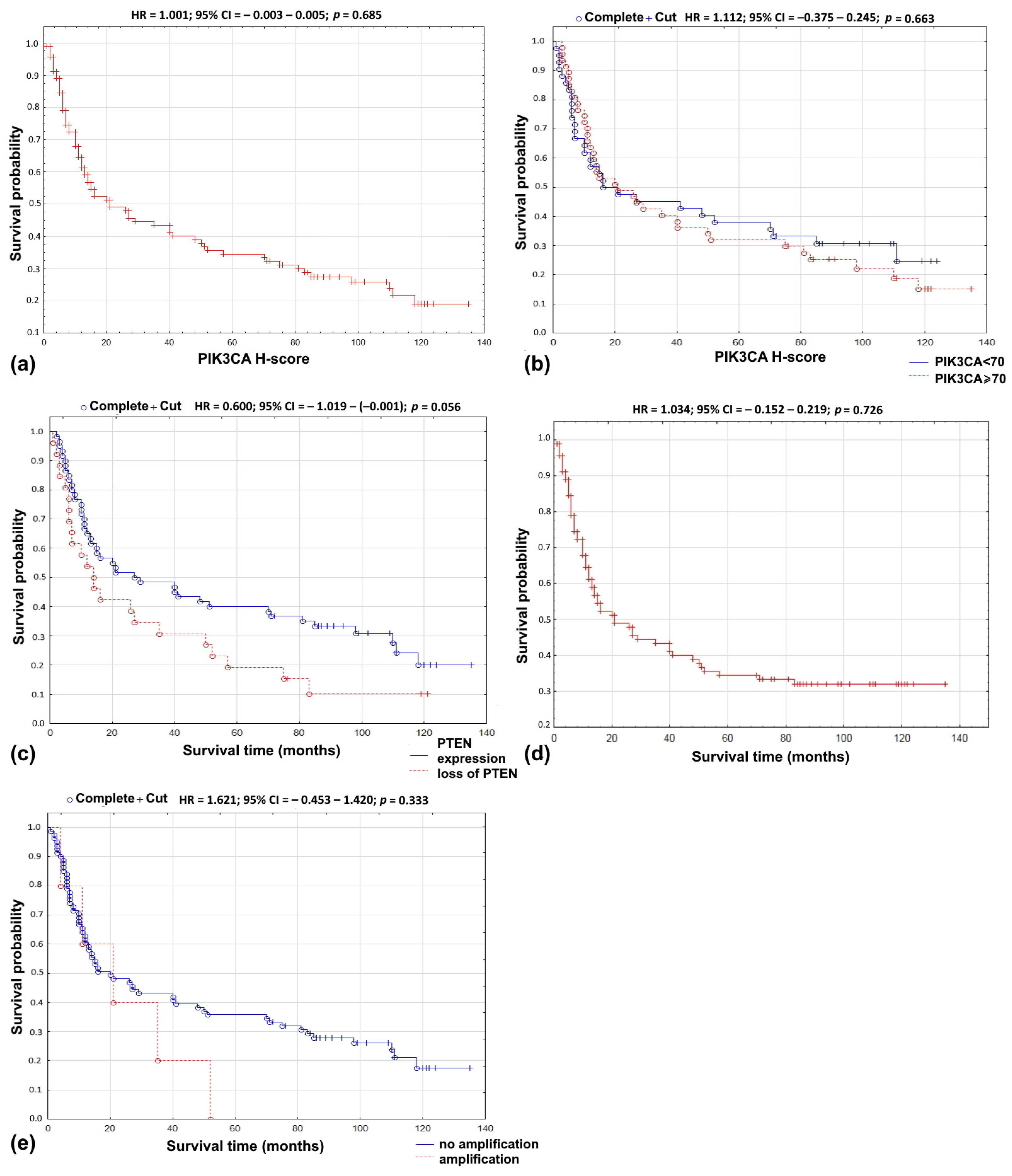
2.4. Combined PIK3CA Protein Level and PIK3CA Gene Copy Number Analysis
2.5. Combined PIK3CA and PTEN Protein Expression Evaluation
2.6. Combined Loss of PTEN Protein and PIK3CA Gene Copy Number Evaluation
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Tissue Microarray
4.3. Immunohistochemistry
4.4. Chromogenic and Silver In Situ Hybridization
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| aCGH | array comparative genomic hybridization |
| AKT | serine-threonine kinase |
| CISH | chromogenic in situ hybridization |
| cMET | tyrosine-protein kinase Met |
| EGFR | epidermal growth factor receptor |
| FISH | fluorescent in situ hybridization |
| H-score | hybrid scoring system method |
| HNSCC | head and neck squamous cell carcinoma |
| HR | hazard ratio |
| IHC | immunohistochemistry |
| MLPA | multiplex ligation-dependent probe amplification |
| OSCC | oral squamous cell carcinoma |
| p | p value |
| PCR | polymerase chain reaction |
| PDK1 | 3-phosphoinositide-dependent kinase-1 |
| PH | pleckstrin homology |
| PI3K | intracellular phosphatidylinositol 3-kinase signaling pathway |
| PIK3CA or p110 | phosphatidylinositol-4,5-bisphosphate 3-kinase |
| PIP2 | phosphatidylinositol 4,5-bisphosphate |
| PIP3 | phosphatidylinositol 3,4,5-trisphosphate |
| PTEN | phosphatase and tensin homolog encoded on chromosome 10 |
| RT-PCR | reverse transcription polymerase chain reaction |
| RKT | receptor tyrosine kinases |
| SISH | silver in situ hybridization |
| TGFβ/SMAD pathway | transforming growth factor beta/SMAD |
| TMA | tissue microarray |
References
- Sritippho, T.; Chotjumlong, P.; Iamaroon, A. Roles of human papillomaviruses and p16 in oral cancer. Asian Pac. J. Cancer Prev. 2015, 16, 6193–6200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasahira, T.; Kirita, T.; Kuniyasu, H. Update of molecular pathobiology in oral cancer: A review. Int. J. Clin. Oncol. 2014, 19, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2018. Available online: https://gco.iarc.fr/today (accessed on 7 January 2019).
- Llewellyn, C.D.; Johnson, N.W.; Warnakulasuriya, K.A. Risk factors for squamous cell carcinoma of the oral cavity in young people—A comprehensive literature review. Oral Oncol. 2001, 37, 401–418. [Google Scholar] [CrossRef]
- IARC. Tobacco Smoke and Involuntary Smoking, Volume 83. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2004. [Google Scholar]
- Fioretti, F.; Bosetti, C.; Tavani, A.; Franceschi, S.; La Vecchia, C. Risk factors for oral and pharyngealcancer in never smokers. Oral Oncol. 1999, 35, 375–378. [Google Scholar] [CrossRef]
- Neville, B.W.; Day, T.A. Oral cancer and precancerous lesions. CA Cancer J. Clin. 2002, 52, 195–215. [Google Scholar] [CrossRef]
- Taberna, M.; Inglehart, R.C.; Pickard, R.K.; Fakhry, C.; Agrawal, A.; Katz, M.L.; Gillison, M.L. Significant changes in sexual behavior after a diagnosis of human papillomavirus-positive and human papillomavirus-negative oral cancer. Cancer 2017, 123, 1156–1165. [Google Scholar] [CrossRef] [Green Version]
- Llewellyn, C.D.; Johnson, N.W.; Warnakulasuriya, K.A. Risk factors for oral cancer in newly diagnosed patients aged 45 years and younger: A case-control study in Southern England. J. Oral Pathol. Med. 2004, 33, 525–532. [Google Scholar] [CrossRef]
- Monteiro, L.S.; Delgado, M.L.; Ricardo, S.; Garcez, F.; do Amaral, B.; Warnakulasuriya, S.; Lopes, C. Phosphorylated mammalian target of rapamycin is associated with an adverse outcome in oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 638–645. [Google Scholar] [CrossRef]
- Johnson, N.W.; Jayasekara, P.; Amarasinghe, A.A. Squamous cell carcinoma and precursor lesions of the oral cavity: Epidemiology and aetiology. Periodontology 2000 2011, 57, 19–37. [Google Scholar] [CrossRef] [Green Version]
- Pentenero, M.; Gandolfo, S.; Carrozzo, M. Importance of tumor thickness and depth of invasion in nodal involvement and prognosis of oral squamous cell carcinoma: A review of the literature. Head Neck 2005, 27, 1080–1991. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, L.; Ricardo, S.; Delgado, M.; Garcez, F.; do Amaral, B.; Lopes, C. Phosphorylated EGFR at tyrosine 1173 correlates with poor prognosis in oral squamous cell carcinomas. Oral Dis. 2014, 20, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.M.; Shiah, S.G.; Huang, C.C.; Hsiao, J.R.; Chang, J.Y. Up-regulation of miR-455-5p by the TGF-β-SMAD signalling axis promotes the proliferation of oral squamous cancer cells by targeting UBE2B. J. Pathol. 2016, 240, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Murugan, A.K.; Munirajtan, A.K.; Tsuchida, N. Ras oncogenes in oral cancer: The past 20 years. Oral Oncol. 2012, 48, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Izumchenko, E.; Sun, K.; Jones, S.; Brait, M.; Agrawal, N.; Koch, W.; McCord, C.L.; Riley, D.R.; Angiuoli, S.V.; Velculescu, V.E.; et al. Notch1 mutations are drivers of oral tumorigenesis. Cancer Prev. Res. 2015, 8, 277–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemans, C.R.; Braakhuis, B.J.; Brakenhoff, R.H. The molecular biology of head and neck cancer. Nat. Rev. Cancer 2011, 11, 9–22. [Google Scholar] [CrossRef]
- Samuels, Y.; Waldman, T. Oncogenic mutations of PIK3CA in human cancers. Curr. Top. Microbiol. Immunol. 2010, 347, 21–41. [Google Scholar] [CrossRef]
- Brana, I.; Siu, L.L. Clinical development of phosphatidylinositol 3-kinase inhibitors for cancer treatment. BMC Med. 2012, 10, 161. [Google Scholar] [CrossRef] [Green Version]
- Price, K.A.; Cohen, E.E. Mechanisms of and therapeutic approaches for overcoming resistance to epidermal growth factor receptor (EGFR)-targeted therapy in squamous cell carcinoma of the head and neck (SCCHN). Oral Oncol. 2015, 51, 399–408. [Google Scholar] [CrossRef]
- Cantley, L.C. The phosphoinositide 3-kinase pathway. Science 2002, 296, 1655–1657. [Google Scholar] [CrossRef]
- Engelman, J.A.; Luo, J.; Cantley, L.C. The evolution of phosphatidylinositol 3-kinases as regulators of growth and metabolism. Nat. Rev. Genet. 2006, 7, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Samuels, Y.; Ericson, K. Oncogenic PI3K and its role in cancer. Curr. Opin. Oncol. 2006, 18, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.R.; Mell, L.K.; Cohen, E.E. Targeting the PI3K/AKT/mTOR pathway in squamous cell carcinoma of the head and neck. Oral Oncol. 2015, 51, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Carnero, A.; Blanco-Aparicio, C.; Renner, O.; Link, W.; Leal, J.F.M. The PTEN/PI3K/AKT signalling pathway in cancer, therapeutic implications. Curr. Cancer Drug. Targets 2008, 8, 187–198. [Google Scholar] [CrossRef]
- Sal, V.; Demirkiran, F.; Erenel, H.; Tokgozoglu, N.; Kahramanoglu, I.; Bese, T.; Turan, H.; Sofiyeva, N.; Calay, Z.; Arvas, M.; et al. Expression of PTEN and β-Catenin and Their Relationship With Clinicopathological and Prognostic Factors in Endometrioid Type Endometrial Cancer. Int. J. Gynecol. Cancer 2016, 26, 512–520. [Google Scholar] [CrossRef]
- Ermoian, R.P.; Furniss, C.S.; Lamborn, K.R.; Basila, D.; Berger, M.S.; Gottschalk, A.R.; Nicholas, M.K.; Stokoe, D.; Haas-Kogan, D.A. Dysregulation of PTEN and protein kinase B is associated with glioma histology and patient survival. Clin. Cancer Res. 2002, 8, 1100–1106. [Google Scholar]
- Krohn, A.; Diedler, T.; Burkhardt, L.; Mayer, P.S.; De Silva, C.; Meyer-Kornblum, M.; Kötschau, D.; Tennstedt, P.; Huang, J.; Gerhäuser, C.; et al. Genomic deletion of PTEN is associated with tumor progression and early PSA recurrence in ERG fusion-positive and fusion-negative prostate cancer. Am. J. Pathol. 2012, 181, 401–412. [Google Scholar] [CrossRef]
- Qiu, W.; Schönleben, F.; Li, X.; Ho, D.J.; Close, L.G.; Manolidis, S.; Bennet, B.P.; Su, G.H. PIK3CA mutations in head and neck squamous cell carcinoma. Clin. Cancer Res. 2006, 12, 1441–1446. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.F.; Yu, B.H.; Li, D.L.; Ke, H.L.; Guo, X.Z.; Xiao, X.Y. PI3K expression and PIK3CA mutations are related to colorectal cancer metastases. World J. Gastroenterol. 2012, 18, 3745–3751. [Google Scholar] [CrossRef]
- Li, X.; Li, M.; Chen, D.; Shi, G.; Zhao, H. PAQR3 inhibits proliferation via suppressing PI3K/AKT signaling pathway in non-small cell lung cancer. Arch. Med. Sci. 2017, 14, 1289–1297. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.W. Initiating breast cancer by PIK3CA mutation. Breast Cancer Res. 2012, 14, 301. [Google Scholar] [CrossRef] [PubMed]
- Janku, F.; Wheler, J.J.; Westin, S.N.; Moulder, S.L.; Naing, A.; Tsimberidou, A.M.; Fu, S.; Falchook, G.S.; Hong, D.S.; Garrido-Laguna, I.; et al. PI3K/AKT/mTOR inhibitors in patients with breast and gynecologic malignancies harboring PIK3CA mutations. J. Clin. Oncol. 2012, 30, 777–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, F.L.; Jorissen, R.N.; Lipton, L.; Mouradov, D.; Sakthianandeswaren, A.; Christie, M.; Li, S.; Tsui, C.; Tie, J.; Desai, J.; et al. PIK3CA and PTEN gene and exon mutation-specific clinicopathologic and molecular associations in colorectal cancer. Clin. Cancer Res. 2013, 19, 3285–3296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, S.; Inoue, H.; Yasuda, K.; Suzuki, K.; Higashi, H.; Era, S.; Mori, M. Reduced expression of PTEN protein and its prognostic implications in invasive ductal carcinoma of the breast. Oncology 2005, 68, 398–404. [Google Scholar] [CrossRef]
- Xiao, J.; Hu, C.P.; He, B.X.; Chen, X.; Lu, X.X.; Xie, M.X.; Li, W.; He, S.Y.; You, S.J.; Chen, Q. PTEN expression is a prognostic marker for patients with non-small cell lung cancer: A systematic review and meta-analysis of the literature. Oncotarget 2016, 7, 57832–57840. [Google Scholar] [CrossRef] [Green Version]
- Taghavi, N.; Yazdi, I. Prognostic factors of survival rate in oral squamous cell carcinoma: Clinical, histologic, genetic and molecular concepts. Arch. Iran. Med. 2015, 18, 314–319. [Google Scholar]
- Starzyńska, A.; Sejda, A.; Adamska, P.; Marvaso, G.; Sakowicz-Burkiewicz, M.; Adamski, Ł.; Jereczek-Fossa, B.A. Prognostic value of the PIK3CA, AKT, and PTEN mutations in oral squamous cell carcinoma: Literature review. Arch. Med. Sci. 2020. [Google Scholar] [CrossRef]
- Amornphimoltham, T.; Roth, S.J.; Ideker, T.; Gutkind, J.S. Targeting the mTOR signaling circuitry in head and neck cancer. In Squamous Cell Carcinoma. Molecular Therapeutic Targets; Warnakulasuriya, S., Khan, Z., Eds.; Springer: Berlin, Germany, 2017. [Google Scholar]
- Vander Broek, R.; Mohan, S.; Eytan, D.F.; Chen, Z.; Van Waes, C. The PI3K/Akt/mTOR axis in head and neck cancer: Functions, aberrations, cross-talk, and therapies. Oral Dis. 2015, 21, 815–825. [Google Scholar] [CrossRef]
- Massacesi, C.; Di Tomaso, E.; Urban, P.; Germa, C.; Quadt, C.; Trandafir, L.; Aimone, P.; Fretault, N.; Dharan, B.; Tavorath, R.; et al. PI3K inhibitors as new cancer therapeutics: Implications for clinical trial design. Onco Targets Ther. 2016, 9, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Soulières, D.; Faivre, S.; Mesía, R.; Remenár, É.; Li, S.H.; Karpenko, A.; Dechaphunkul, A.; Ochsenreither, S.; Kiss, L.A.; Lin, J.C.; et al. Buparlisib and paclitaxel in patients with platinum-pretreated recurrent or metastatic squamous cell carcinoma of the head and neck (BERIL-1): A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Oncol. 2017, 18, 323–335. [Google Scholar] [CrossRef]
- Fury, M.G.; Lee, N.Y.; Sherman, E.; Ho, A.L.; Rao, S.; Heguy, A.; Shen, R.; Korte, S.; Lisa, D.; Ganly, I.; et al. A Phase 1 Study of Everolimus + Weekly Cisplatin + Intensity Modulated Radiation Therapy in Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Fury, M.G.; Sherman, E.; Ho, A.L.; Tsai, F.; Xiao, H.; Nwankwo, O.; Sima, C.; Heguy, A.; Katabi, N.; Haque, S.; et al. A phase 1 study of everolimus plus docetaxel plus cisplatin as induction chemotherapy for patients with locally and/or regionally advanced head and neck cancer. Cancer 2013, 119, 1823–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymond, E.; Tourneau, C.L.; Gatineau, M.; Delord, J.P.; Fayette, J.; Tijeras-Raballand, C.D.A.; Albert, S.; Granier, M.; Chibaudel, B.; Hadengue, A.; et al. CAPRA: Safety, efficacy, and translational biomarkers of weekly everolimus, carboplatin, and paclitaxel as induction therapy for locally advanced head and neck squamoous cell carcinoma (HNSCC). J. Clin. Oncol. 2013, 31, 6036. [Google Scholar] [CrossRef]
- Liu, C.J.; Lin, S.C.; Chen, Y.J.; Chang, K.M.; Chang, K.W. Array-comparative genomic hybridization to detect genomewide changes in microdissected primary and metastatic oral squamous cell carcinomas. Mol. Carcinog. 2006, 45, 721–731. [Google Scholar] [CrossRef]
- Won, H.S.; Jung, C.K.; Chun, S.H.; Kang, J.H.; Kim, Y.S.; Sun, D.I.; Kim, M.S. Difference in expression of EGFR, pAkt, and PTEN between oropharyngeal and oral cavity squamous cell carcinoma. Oral Oncol. 2012, 48, 985–990. [Google Scholar] [CrossRef]
- Garg, R.; Kapoor, V.; Mittal, M.; Singh, M.K.; Shukla, N.K.; Das, S.N. Abnormal expression of PI3K isoforms in patients with tobacco-related oral squamous cell carcinoma. Clin. Chim. Acta 2013, 416, 100–106. [Google Scholar] [CrossRef]
- Xiong, H.; Yang, Y.; Yang, K.; Zhao, D.; Tang, H.; Ran, X. Loss of the clock gene PER2 is associated with cancer development and altered expression of important tumor-related genes in oral cancer. Int. J. Oncol. 2018, 52, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Krump, M.; Ehrmann, J. Differences in CD44s expression in HNSCC tumours of different areas within the oral cavity. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech. Repub. 2013, 157, 280–283. [Google Scholar] [CrossRef] [Green Version]
- Mandapathil, M.; Boduc, M.; Netzer, C.; Güldner, C.; Roessler, M.; Wallicek-Dworschak, U.; Jahns, E.; Stuck, B. CD73 expression in lymph node metastases in patients with head and neck cancer. Acta Otolaryngol. 2018, 138, 180–184. [Google Scholar] [CrossRef]
- Dave, J.H.; Vora, H.H.; Ghosh, N.R.; Trivedi, T.I. Mediator of DNA damage checkpoint protein 1 (MDC1) as a prognostic marker for patients with oral squamous cell carcinoma. J. Oral Pathol. Med. 2017, 46, 253–258. [Google Scholar] [CrossRef]
- Wang, L.; Hu, H.; Pan, Y.; Wang, R.; Li, Y.; Shen, L.; Yu, Y.; Li, H.; Cai, D.; Sun, Y.; et al. PIK3CA mutations frequently coexist with EGFR/KRAS mutations in non-small cell lung cancer and suggest poor prognosis in EGFR/KRAS wildtype subgroup. PLoS ONE 2014, 9, e88291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.F.; Zhou, X.K.; Chen, J.H.; Yi, G.; Chen, H.G.; Ba, M.C.; Lin, S.Q.; Qi, Y.F. Up-regulation of PIK3CA promotes metastasis in gastric carcinoma. World J. Gastroenterol. 2010, 16, 4986–4991. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; Dziadziuszko, R.; Thatcher, N.; Mann, H.; Watkins, C.; Parums, D.V.; Speake, G.; Holloway, B.; Bunn, P.A., Jr.; Franklin, W.A. Epidermal growth factor receptor immunohistochemistry: Comparison of antibodies and cut off points to predict benefit from gefitinib in a phase 3 placebo-controlled study in advanced non small-cell lung cancer. Cancer 2008, 112, 1114–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, M.S.; Sakurada, A.; Cutz, J.C.; Zhu, C.Q.; Kamel-Reid, S.; Squire, J.; Lorimer, L.; Zhang, T.; Liu, N.; Daneshmand, M.; et al. Erlotinib in lung cancer—Molecular and clinical predictors of outcome. N. Engl. J. Med. 2005, 353, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Woenckhaus, J.; Steger, K.; Werner, E.; Fenic, I.; Gamerdinger, U.; Dreyer, T.; Stahl, U. Genomic gain of PIK3CA and increased expression of p110alpha are associated with progression of dysplasia into invasive squamous cell carcinoma. J. Pathol. 2002, 198, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Böhle, A.S.; Dohrmann, P.; Leuschner, I.; Schulz, A.; Kremer, B.; Fändrich, F. Overexpression of phosphatidylinositol 3-kinase in human lung cancer. Langenbecks Arch. Surg. 2001, 386, 293–301. [Google Scholar] [CrossRef]
- Akagi, I.; Miyashita, M.; Makino, H.; Nomura, T.; Hagiwara, N.; Takahashi, K.; Cho, K.; Mishima, T.; Ishibashi, O.; Ushijima, T.; et al. Overexpression of PIK3CA is associated with lymph node metastasis in esophageal squamous cell carcinoma. Int. J. Oncol. 2009, 34, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Abe, A.; Minaguchi, T.; Ochi, H.; Onuki, M.; Okada, S.; Matsumoto, K.; Satoh, T.; Oki, A.; Yoshikawa, H. PIK3CA overexpression is a possible prognostic factor for favorable survival in ovarian clear cell carcinoma. Hum. Pathol. 2013, 44, 199–207. [Google Scholar] [CrossRef]
- Jehan, Z.; Bavi, P.; Sultana, M.; Abubaker, J.; Bu, R.; Hussain, A.; Alsbeih, G.; Al-Sanea, N.; Abduljabbar, A.; Ashari, L.H.; et al. Frequent PIK3CA gene amplification and its clinical significance in colorectal cancer. J. Pathol. 2009, 219, 337–346. [Google Scholar] [CrossRef]
- Firoozinia, M.; Moghadamtousi, S.Z.; Nikzad, S.; Abdul, K.H. PIK3CA gene amplification and PI3K p110α protein expression in breast carcinoma. Int. J. Med. Sci. 2014, 11, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Afkhami, M.; Schmolze, D.; Yost, S.E.; Frankel, P.H.; Dagis, A.; Amanam, I.U.; Telatar, M.; Nguyen, K.; Yu, K.W.; Luu, T.; et al. Mutation and immune profiling of metaplastic breast cancer: Correlation with survival. PLoS ONE 2019, 14, e0224726. [Google Scholar] [CrossRef]
- García-Carracedo, D.; Villaronga, M.Á.; Álvarez-Teijeiro, S.; Hermida-Prado, F.; Santamaría, I.; Allonca, E.; Suárez-Fernández, L.; Gonzalez, M.V.; Balbín, M.; Astudillo, A.; et al. Impact of PI3K/AKT/mTOR pathway activation on the prognosis of patients with head and neck squamous cell carcinomas. Oncotarget 2016, 7, 29780–29793. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.I.; Soria, J.C.; Hassan, K.A.; El-Naggar, A.K.; Tang, X.; Liu, D.D.; Hong, W.K.; Mao, L. Loss of PTEN expression as a prognostic marker for tongue cancer. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 1441–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squarize, C.H.; Castilho, R.M.; Santos Pinto, D. Immunohistochemical evidence of PTEN in oral squamous cell carcinoma and its correlation with the histological malignancy grading system. J. Oral Pathol. Med. 2002, 31, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Angadi, P.V.; Krishnapillai, R. Evaluation of PTEN immunoexpression in oral submucous fibrosis: Role in pathogenesis and malignant transformation. Head Neck Pathol. 2012, 6, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmani, A.; Alzohairy, M.; Babiker, A.Y.; Rizvi, M.A.; Elkarimahmad, H.G. Clinicopathological significance of PTEN and bcl2 expressions in oral squamous cell carcinoma. Int. J. Clin. Exp. Pathol. 2012, 5, 965–971. [Google Scholar]
- Monteiro, L.S.; Amaral, J.B.; Vizcaíno, J.R.; Lopes, C.A.; Torres, F.O. A clinical-pathological and survival study of oral squamous cell carcinomas from a population of the North of Portugal. Med. Oral Patol. Oral Cir. Bucal. 2014, 19, e120–e126. [Google Scholar] [CrossRef] [Green Version]
- Miyahara, L.A.N.; Pontes, F.S.C.; Burbano, R.M.R.; Conte Neto, N.; Guimarães, D.M.; Fonseca, F.P.; Pontes, H.A.R. PTEN allelic loss is an important mechanism in the late stage of development of oral leucoplakia into oral squamous cell carcinoma. Histopathology 2018, 72, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Pickhard, A.; Gröber, S.; Haug, A.K.; Piontek, G.; Wirth, M.; Straßen, U.; Redelius, M.; Reiter, R. Survivin and pAkt as potential prognostic markers in squamous cell carcinoma of the head and neck. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 733–742. [Google Scholar] [CrossRef]
- Mastronikolis, N.S.; Tsiambas, E.; Papadas, T.A.; Karameris, A.; Ragos, V.; Peschos, D.; Mastronikolis, S.N.; Papadas, A.T.; Liatsos, C.; Armata, I.E.; et al. Deregulation of PTEN expression in laryngeal squamous cell carcinoma based on tissue microarray digital analysis. Anticancer Res. 2017, 37, 5521–5524. [Google Scholar] [CrossRef]
- Wang, J.; Chen, H.; Liao, Y.; Chen, N.; Liu, T.; Zhang, H.; Zhang, H. Expression and clinical evidence of miR-494 and PTEN in non-small cell lung cancer. Tumour. Biol. 2015, 36, 6965–6972. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Tian, Y.; Zhu, C.; Yang, X.; Sun, Q. High miR-718 Suppresses phosphatase and tensin homolog (PTEN) expression and correlates to unfavorable prognosis in gastric cancer. Med. Sci. Monit. 2018, 24, 5840–5850. [Google Scholar] [CrossRef] [PubMed]
- Kechagioglou, P.; Papi, R.M.; Provatopoulou, X.; Kalogera, E.; Papadimitriou, E.; Grigoropoulos, P.; Nonni, A.; Zografos, G.; Kyriakidis, D.A.; Gounaris, A.; et al. Tumor suppressor PTEN in breast cancer: Heterozygosity, mutations and protein expression. Anticancer Res. 2014, 34, 1387–1400. [Google Scholar] [PubMed]
- Naguib, A.; Cooke, J.C.; Happerfield, L.; Kerr, L.; Gay, L.J.; Luben, R.N.; Ball, R.Y.; Mitrou, P.N.; McTaggart, A.; Arends, M.J. Alterations in PTEN and PIK3CA in colorectal cancers in the EPIC Norfolk study: Associations with clinicopathological and dietary factors. BMC Cancer 2011, 11, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Huang, H.; Sun, L.; Yang, M.; Pan, C.; Chen, W.; Wu, D.; Lin, Z.; Zeng, C.; Yao, Y.; et al. MiR-21 indicates poor prognosis in tongue squamous cell carcinomas as an apoptosis inhibitor. Clin. Cancer Res. 2009, 15, 3998–4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozaki, K.; Imoto, I.; Pimkhaokham, A.; Hasegawa, S.; Tsuda, H.; Omura, K.; Inaawa, J. PIK3CA mutation is an oncogenic aberration at advanced stages of oral squamous cell carcinoma. Cancer Sci. 2006, 97, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Fenic, I.; Steger, K.; Gruber, C.; Arens, C.; Woenckhaus, J. Analysis of PIK3CA and Akt/protein kinase B in head and neck squamous cell carcinoma. Oncol. Rep. 2007, 18, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Tu, H.F.; Chang, K.W.; Chiang, W.F.; Liu, C.J.; Yu, E.H.; Liu, S.T.; Lin, S.C. The frequent co-expression of the oncogenes PIK3CA and PAK1 in oral carcinomas. Oral Oncol. 2011, 47, 211–216. [Google Scholar] [CrossRef]
- Suda, T.; Hama, T.; Kondo, S.; Yuza, Y.; Yoshikawa, M.; Urashima, M.; Kato, T.; Moriyama, H. Copy number amplification of the PIK3CA gene is associated with poor prognosis in non-lymph node metastatic head and neck squamous cell carcinoma. BMC Cancer 2012, 12, 416. [Google Scholar] [CrossRef] [Green Version]
- Cha, J.D.; Kim, H.J.; Cha, I.H. Genetic alterations in oral squamous cell carcinoma progression detected by combining array-based comparative genomic hybridization and multiplex ligation-dependent probe amplification. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 594–607. [Google Scholar] [CrossRef]
- Sticht, C.; Hofele, C.; Flechtenmacher, C.; Bosch, F.X.; Freier, K.; Joos, S. Amplification of Cyclin L1 is associated with lymph node metastases in head and neck squamous cell carcinoma (HNSCC). Br. J. Cancer 2005, 92, 770–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikawa, Y.; Morita, K.I.; Kayamori, K.; Tanimoto, K.; Sakamoto, K.; Katoh, H.; Ishikawa, S.; Inazawam, J.; Harada, H. Receptor tyrosine kinase amplification is predictive of distant metastasis in patients with oral squamous cell carcinoma. Cancer Sci. 2017, 108, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Badzio, A.; Wynes, M.W.; Dziadziuszko, R.; Merrick, D.T.; Pardo, M.; Rzyman, W.; Kowalczyk, A.; Singh, S.; Ranger-Moore, J.; Manriquez, G.; et al. Increased insulin-like growth factor 1 receptor protein expression and gene copy number in small cell lung cancer. J. Thorac. Oncol. 2010, 5, 1905–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, H.; Herold, T.; Ting, S.; Worm, K.; Huber, U.; Christoph, D.C.; Eberhardt, W.E.; Kostbade, K.; Kasper, S.; Stamatis, G.; et al. HER2 expression and markers of phosphoinositide-3-kinase pathway activation define a favorable subgroup of metastatic pulmonary adenocarcinomas. Lung. Cancer 2015, 88, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, H.; Xiu, J.; Reddy, S.K.; DeBernardo, R. Alteration in PI3K/mTOR, MAPK pathways and Her2 expression/amplification is more frequent in uterine serous carcinoma than ovarian serous carcinoma. J. Surg. Oncol. 2015, 112, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.R.; Park, H.S.; Ahn, Y.Z.; Nam, S.; Jung, H.R.; Park, S.; Lee, S.J.; Balch, C.; Powis, G.; Ku, J.L.; et al. Improving gastric cancer preclinical studies using diverse in vitro and in vivo model systems. BMC Cancer 2016, 16, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Yamashita, T.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor-Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef]
- Bartels, S.; van Luttikhuizen, J.L.; Christgen, M.; Mägel, L.; Luft, A.; Hänzelmann, S.; Lehmann, U.; Schlegelberger, B.; Leo, F.; Steinemann, D.; et al. CDKN2A loss and PIK3CA mutation in myoepithelial-like metaplastic breast cancer. J. Pathol. 2018, 245, 373–383. [Google Scholar] [CrossRef]
- Xing, Y.; Lin, N.U.; Maurer, M.A.; Chen, H.; Mahvash, A.; Sahin, A.; Akcakanat, A.; Li, Y.; Abramson, V.; Litton, J.; et al. Phase II trial of AKT inhibitor MK-2206 in patients with advanced breast cancer who have tumors with PIK3CA or AKT mutations, and/or PTEN loss/PTEN mutation. Breast Cancer Res. 2019, 21, 78. [Google Scholar] [CrossRef] [Green Version]
- Dziadziuszko, R.; Wynes, M.W.; Singh, S.; Asuncion, B.R.; Ranger-Moore, J.; Konopa, K.; Rzyman, W.; Szostakiewicz, B.; Jassem, J.; Hirsch, F.R. Correlation between MET gene copy number by silver in situ hybridization and protein expression by immunohistochemistry in non-small cell lung cancer. J. Thorac. Oncol. 2012, 7, 340–347. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All | PIK3CA Protein Expression | PTEN Protein Expression | Amplification | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Low Level of PIK3CA | High Level of PIK3CA | p Value | Loss of PTEN | Expression of PTEN | p Value | No Amplification of the PIK3CA Gene | Amplification of the PIK3CA Gene | p Value | ||
| N (%) | 92 (100) | 44 (48.35) | 47 (51.65) | - | 28 (31.46) | 61 (68.54) | - | 84 (94.38) | 5 (5.62) | - |
| Age, n (%) | ||||||||||
| <60 | 62 (67.39) | 19 (43.18) | 19 (39.58) | 0.726 | 14 (50.00) | 23 (37.70) | 0.279 | 36 (42.86) | 2 (40.00) | 0.725 |
| ≥60 | 30 (32.61) | 25 (56.82) | 29 (60.42) | 14 (50.00) | 38 (62.30) | 48 (57.14) | 3 (60.00) | |||
| Gender, n (%) | ||||||||||
| Male | 62 (67.39) | 33 (75.00) | 29 (60.42) | 0.136 | 22 (78.57) | 39 (63.93) | 0.171 | 57 (67.86) | 3 (60.00) | 0.909 |
| Female | 30 (32.61) | 11 (25.00) | 19 (39.58) | 6 (21.43) | 22 (36.07) | 27 (31.14) | 2 (40.00) | |||
| Localization, n (%) | ||||||||||
| Tongue | 23 (25.00) | 12 (27.28) | 11 (22.92) | 0.924 | 7 (25.00) | 15 (24.59) | 0.753 | 22 (26.19) | 1 (20.00) | 0.040 |
| Buccal mucosa | 15 (16.30) | 7 (15.90) | 8 (16.66) | 4 (14.28) | 11 (18.04) | 15 (17.85) | 0 (0) | |||
| Floor of mouth | 29 (31.52) | 13 (29,55) | 16 (33.34) | 11 (39.28) | 17 (27.87) | 26 (30.95) | 0 (0) | |||
| Upper gingiva | 9 (9.79) | 1 (2.72) | 8 (16.66) | 3 (10.71) | 5 (8.20) | 9 (10.71) | 0 (0) | |||
| Lower gingiva | 14 (15.22) | 9 (20.45) | 5 (10.42) | 2 (7.14) | 12 (19.67) | 10 (11.90) | 4 (80.00) | |||
| Hard palate | 2 (2.17) | 1 (2.72) | 1 (2.08) | 1 (3.57) | 1 (1.64) | 2 (1.02) | 0 (0) | |||
| Smoking, n (%) | ||||||||||
| Smoking patients | 49 (53.26) | 24 (54.55) | 25 (52.08) | 0.423 | 12 (42.86) | 36 (59.02) | 0.055 | 44 (52.38) | 3 (60.00) | 0.957 |
| No smoking patients | 18 (19.57) | 7 (15.91) | 11 (22.92) | 9 (32.14) | 9 (14.75) | 16 (19.05) | 1 (20.00) | |||
| No data | 25 (27.17) | 13 (29.55) | 12 (25.00) | 7 (25.00) | 16 (22.23) | 24 (28.57) | 1 (20.00) | |||
| Alcohol abuse, n (%) | ||||||||||
| Alcoholics | 14 (15.22) | 8 (18.18) | 6 (12.50) | 0.329 | 4 (14.29) | 10 (16.39) | 0.745 | 13 (15.48) | 0 (0) | 0.382 |
| No alcoholics | 52 (56.52) | 24 (54.55) | 28 (58.33) | 17 (60.71) | 34 (55.74) | 47 (55.95) | 3 (60.00) | |||
| No data | 26 (28.26) | 12 (27.27) | 14 (29.17) | 7 (25.00) | 17 (27.87) | 24 (28.57) | 2 (40.00) | |||
| Grading according to WHO, n (%) | ||||||||||
| G1 | 38 (41.30) | 18 (40.91) | 20 (41.67) | 0.561 | 12 (42.86) | 25 (40.98) | 0.671 | 34 (40.48) | 1 (20.00) | 0.351 |
| G2 | 43 (46.74) | 23 (52.27) | 20 (41.67) | 14 (50.00) | 28 (45.90) | 40 (47.62) | 3 (60.00) | |||
| G3 | 11 (11.95) | 3 (6.82) | 8 (16.67) | 2 (7.14) | 8 (13.11) | 10 (11.90) | 1 (20.00) | |||
| TNM staging system | ||||||||||
| T—primary tumor, n (%) | ||||||||||
| T1 | 16 (17.39) | 9 (20.45) | 10 (20.45) | 0.191 | 3 (10.71) | 13 (21.31) | 0.045 | 20 (23.81) | 1 (20.00) | 1.000 |
| T2a and T2b | 24 (26.09) | 13 (29.55) | 14 (29.55) | 7 (25.00) | 16 (26.23) | 3 (3.57) | 0 (0) | |||
| T3 | 12 (13.04) | 4 (9.09) | 4 (9.09) | 5 (17.86) | 7 (11.48) | 7 (8.33) | 1 (20.00) | |||
| T4a, T4b | 19 (20.65) | 8 (18.18) | 9 (18.18) | 9 (32.14) | 9 (14.75) | 6 (7.14) | 0 (0) | |||
| No data | 21 (22.83) | 10 (22.73) | 11 (22.73) | 4 (14.29) | 16 (26.23) | 48 (57.14) | 3 (60.00) | |||
| N—regional lymph nodes, n (%) | ||||||||||
| N0 | 37 (40.22) | 18 (40.91) | 19 (39.58) | 0.116 | 10 (35.71) | 26 (42.62) | 0.263 | 33 (39.29) | 1 (20.00) | 0.921 |
| N1 | 6 (6.52) | 4 (9.09) | 2 (4.17) | 1 (3.57) | 5 (8.20) | 6 (7.14) | 0 (0) | |||
| N2a, N2b, N2c | 14 (15.22) | 9 (20.45) | 5 (10.42) | 9 (32.14) | 5 (8.20) | 13 (15.48) | 1 (20.00) | |||
| N3a and T3b | 13 (14.13) | 1 (2.27) | 12 (25.00) | 4 (14.29) | 9 (14.75) | 13 (15.48) | 0 (0) | |||
| No data | 22 (23.91) | 12 (27.27) | 10 (20.83) | 4 (14.29) | 16 (26.23) | 19 (22.62) | 3 (60.00) | |||
| M—distant metastases, n (%) | ||||||||||
| M0 | 6 (6.52) | 5 (11.36) | 1 (2.08) | 0.061 | 3 (10.71) | 3 (4.92) | 0.474 | 6 (7.14) | 0 (0) | 0.682 |
| M1 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Mx | 64 (69.57) | 27 (61.36) | 37 (77.08) | 22 (78.57) | 41 (67.21) | 59 (70.24) | 2 (40.00) | |||
| No data | 22 (23.91) | 12 (27.27) | 10 (20.83) | 3 (10.71) | 17 (27.87) | 19 (22.62) | 3 (60.00) | |||
| Staging by WHO, n (%) | ||||||||||
| I | 16 (17.39) | 9 (20.45) | 7 (14.58) | 0.838 | 3 (10.71) | 13 (21.31) | 0.250 | 15 (17.86) | 0 (0) | 0.793 |
| II | 15 (16.30) | 7 (15.91) | 8 (16.67) | 6 (21.43) | 8 (13.11) | 12 (14.29) | 1 (20.00) | |||
| III | 13 (14.13) | 3 (6.81) | 10 (20.83) | 4 (14.29) | 9 (14.75) | 13 (15.48) | 0 (0) | |||
| IV | 28 (30.43) | 15 (34.09) | 13 (27.08) | 11 (39.29) | 16 (26.23) | 27 (32.14) | 1 (20.00) | |||
| No data | 20 (21.74) | 10 (22.73) | 10 (20.83) | 4 (14.29) | 15 (24.59) | 17 (20.24) | 3 (60.00) | |||
| Treatment, n (%) | ||||||||||
| Surgery | 32 (34.78) | 16 (36.36) | 16 (33.33) | 0.776 | 11 (39.29) | 32,79 | 0.615 | 29 (34.52) | 0 (0) | 0.977 |
| Radiotherapy | 10 (10.87) | 7 (15.91) | 3 (6.25) | 7 (25.00) | 4,92 | 10 (11.90) | 0 (0) | |||
| Chemotherapy | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Surgery and radiotherapy | 21 (22.83) | 8 (18.18) | 13 (27.08) | 6 (21.43) | 14 (22.95) | 19 (22.62) | 2 (40.00) | |||
| Surgery and chemotherapy | 1 (1.09) | 0 (0) | 1 (2.08) | 0 (0) | 1 (1.64) | 1 (1.19) | 0 (0) | |||
| Radiotherapy and chemotherapy | 5 (5.43) | 2 (4.55) | 3 (6.25) | 2 (7.14) | 2 (3.28) | 5 (5.95) | 0 (0) | |||
| Surgery, radiotherapy and chemotherapy | 3 (3.26) | 1 (2.27) | 2 (4.17) | 0 (0) | 3 (4.92) | 3 (3.57) | 0 (0) | |||
| Treatment was not started | 6 (6.52) | 1 (2.27) | 5 (10.42) | 0 (0) | 6 (9.84) | 5 (5.95) | 1 (20.00) | |||
| No data | 14 (15.22) | 9 (20.45) | 5 (10.42) | 2 (7.14) | 12 (19.67) | 12 (14.29) | 2 (40.00) | |||
| Five-year survival, n (%) | ||||||||||
| Five-year survival | 29 (31.52) | 15 (34.09) | 14 (29.17) | 0.557 | 4 (14.29) | 23 (37.70) | 0.030 | 27 (32.14) | 0 (0) | 0.127 |
| Patients did not survive 5 years | 61 (66.30) | 27 (61.36) | 34 (70.83) | 23 (82.14) | 37 (60.66) | 55 (65.48) | 5 (100.00) | |||
| No data | 2 (2.17) | 2 (4.55) | 0 (0) | 1 (3.57) | 1 (1.64) | 2 (2.38) | 0 (0) | |||
| Clinical and Pathological Data | PIK3CA Protein Expression | PTEN Expression | PIK3CA Gene Copy Number | PIK3CA/CEP3 Ratio | ||||
|---|---|---|---|---|---|---|---|---|
| p-Value | r | p-Value | r | p-Value | r | p-Value | r | |
| Age [years] | 0.766 | 0.032 | 0.447 | 0.082 | 0.489 | −0.074 | 0.175 | −0.145 |
| Gender | 0.264 | −0.118 | 0.171 | −0.146 | 0.522 | 0.069 | 0.586 | 0.058 |
| Localization * | 0.761 | −0.032 | 0.752 | 0.034 | 0.297 | 0.112 | 0.078 | 0.188 |
| Smoking | 0.304 | −0.128 | 0.053 | −0.239 | 0.758 | 0.039 | 0.357 | 0.117 |
| Alcohol abuse | 0.307 | −0.128 | 0.741 | 0.042 | 0.769 | 0.038 | 0.275 | 0.140 |
| Grading | 0.293 | 0.111 | 0.670 | 0.046 | 0.050 | 0.208 | 0.070 | 0.193 |
| T | 0.466 | 0.089 | 0.043 | −0.243 | 0.403 | −0.103 | 0.089 | −0.209 |
| N | 0.147 | 0.177 | 0.263 | −0.136 | 0.960 | 0.006 | 0.132 | −0.186 |
| M | 0.052 | −0.235 | 0.470 | −0.088 | 0.542 | −0.076 | 0.420 | −0.100 |
| Staging | 0.747 | −0.039 | 0.250 | −0.139 | 0.406 | −0.102 | 0.052 | −0.235 |
| Treatment ** | 0.715 | 0.042 | 0.615 | −0.059 | 0.196 | 0.151 | 0.151 | 0.167 |
| 5-year survival | 0.462 | −0.079 | 0.028 | 0.235 | 0.616 | 0.054 | 0.416 | 0.088 |
| Clinical and Pathological Data | PIK3CA Protein—Continuous Variable | PIK3CA Protein—H-score 70 as Cut-off Point | Loss of PTEN | PIK3CA Gene Copy Number | PIK3CA/CEP3 Ratio | PIK3CA Gene Amplification | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Age [years] | 1.017 | −0.009–0.042 | 0.205 | 2.709 | −0.172–2.165 | 0.077 | 1.013 | −0.013–0.039 | 0.330 | 1.027 | −0.162–0.215 | 0.783 | 1.195 | −0.249–0.605 | 0.424 | 1.570 | −0.500–1.402 | 0.381 |
| Gender | 1.001 | −0.003–0.005 | 0.623 | 1.160 | −0.347–0.645 | 0.556 | 0.600 | −1.026–0.003 | 0.058 | 1.034 | −0.156–0.223 | 0.727 | 1.202 | −0.239–0.607 | 0.405 | 1.660 | −0.440–1.454 | 0.326 |
| Grading | 1.001 | −0.003–0.005 | 0.750 | 1.070 | −0.428–0.564 | 0.788 | 0.565 | −1.099–(−0.041) | 0.040 | 1.003 | −0.189–0.195 | 0.976 | 1.120 | −0.315–0.542 | 0.610 | 1.563 | −0.499–1.393 | 0.382 |
| Staging | 1.001 | −0.004–0.006 | 0.633 | 1.171 | −0.408–0.723 | 0.584 | 0.556 | −1.174–0 | 0.054 | 0.985 | −0.276–0.247 | 0.912 | 1.165 | −0.530–0.836 | 0.659 | 1.071 | −1.397–1.534 | 0.928 |
| Localisation * | 1.001 | −0.004–0.006 | 0.759 | 1.108 | −0.474–0.679 | 0.727 | 0.680 | −1.026–0.257 | 0.249 | 1.092 | −0.162–0.340 | 0.487 | 1.407 | −0.228–0.910 | 0.244 | 5.783 | 0.054–3.456 | 0.037 |
| Smoking | 1.003 | −0.001–0.002 | 0.155 | 1.491 | −0.182–0.981 | 0.175 | 0.436 | −0.148–(−0.177) | 0.016 | 0.960 | −0.277–0.195 | 0.733 | 1.088 | −0.469–0.637 | 0.768 | 1.595 | −0.597–1.531 | 0.418 |
| Alcohol abuse | 1.002 | −0.002–0.007 | 0.449 | 1.282 | −0.346–0.843 | 0.410 | 0.526 | −1.243–(−0.040) | 0.042 | 0.938 | −0.315–0.187 | 0.614 | 1.030 | −0.562–0.621 | 0.923 | 1.429 | −0.864–1.577 | 0.585 |
| T | 1.001 | −0.002–0.006 | 0.766 | 1.067 | −0.529–0.658 | 0.831 | 0.616 | −1.096–0.128 | 0.125 | 0.976 | −0.252–0.203 | 0.836 | 1.032 | −0.529–0.592 | 0.913 | 0.483 | −2.314–0.859 | 0.337 |
| N | 1.001 | −0.003–0.006 | 0.557 | 1.351 | −0.299–0.900 | 0.325 | 0.532 | −1.267–0.002 | 0.054 | 0.952 | −0.310–0.211 | 0.711 | 1.018 | −0.668–0.704 | 0.958 | 0.676 | −1.940–1.157 | 0.604 |
| M | 1.001 | −0.003–0.006 | 0.582 | 1.145 | −0.434–0.704 | 0.640 | 0.527 | −1.215–(−0.066) | 0.033 | 1.000 | −0.241–0.2413 | 0.999 | 1.139 | −0.503–0.762 | 0.686 | 1.300 | −1.195–1.719 | 0.734 |
| Surgery | 1.000 | −0.004–0.004 | 0.905 | 1.135 | −0.403–0.656 | 0.639 | 0.539 | −1.158–(−0.078) | 0.029 | 1.071 | −0.104–0.242 | 0.445 | 1.215 | −0.179–0.568 | 0.324 | 1.151 | −1.060–1.342 | 0.822 |
| Radiotherapy | 1.002 | −0.003–0.006 | 0.470 | 1.170 | −0.397–0.771 | 0.577 | 0.491 | −1.296–(−0.128) | 0.020 | 0.972 | −0.257–0.291 | 0.809 | 1.061 | −0.470–0.589 | 0.827 | 1.331 | −0.912–1.484 | 0.653 |
| Chemotherapy | 1.002 | −0.003–0.006 | 0.424 | 1.211 | −0.364–0.748 | 0.498 | 0.523 | −1.127–(−0.079) | 0.029 | 0.946 | −0.241–0.181 | 0.643 | 1.0 | −0.520–0.571 | 0.928 | 1.296 | −0.948–1.467 | 0.685 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Starzyńska, A.; Adamska, P.; Sejda, A.; Sakowicz-Burkiewicz, M.; Adamski, Ł.J.; Marvaso, G.; Wychowański, P.; Jereczek-Fossa, B.A. Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma? Life 2020, 10, 325. https://doi.org/10.3390/life10120325
Starzyńska A, Adamska P, Sejda A, Sakowicz-Burkiewicz M, Adamski ŁJ, Marvaso G, Wychowański P, Jereczek-Fossa BA. Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma? Life. 2020; 10(12):325. https://doi.org/10.3390/life10120325
Chicago/Turabian StyleStarzyńska, Anna, Paulina Adamska, Aleksandra Sejda, Monika Sakowicz-Burkiewicz, Łukasz Jan Adamski, Giulia Marvaso, Piotr Wychowański, and Barbara Alicja Jereczek-Fossa. 2020. "Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma?" Life 10, no. 12: 325. https://doi.org/10.3390/life10120325
APA StyleStarzyńska, A., Adamska, P., Sejda, A., Sakowicz-Burkiewicz, M., Adamski, Ł. J., Marvaso, G., Wychowański, P., & Jereczek-Fossa, B. A. (2020). Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma? Life, 10(12), 325. https://doi.org/10.3390/life10120325