
How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
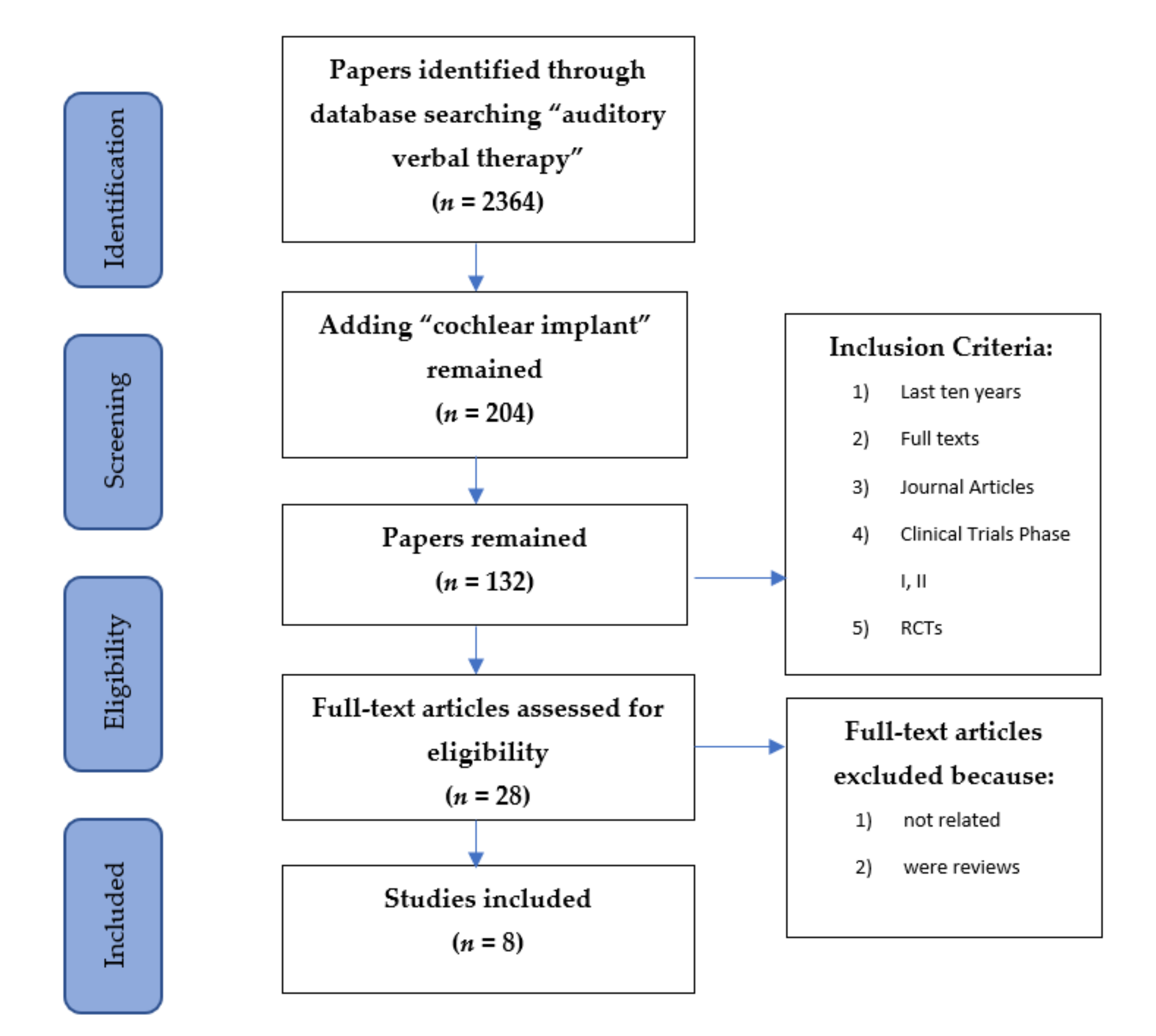
2.1. Identification
2.2. Screening
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
3. Results
3.1. Literature Outcome
3.2. Investigating Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lim, S.Y.C.; Simser, J. Auditory-verbal therapy for children with hearing impairment. Ann. Acad. Med. Singap. 2005, 34, 307–312. [Google Scholar]
- Centers for Disease Control and Prevention. EHDI Hearing Screening & Follow-up Survey. 2014. Available online: https://www.health.state.mn.us/people/newbornscreening/program/ehdireport2014.pdf (accessed on 17 February 2021).
- Moeller, M.P. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000, 106, e43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinaga-Itano, C. Levels of evidence: Universal newborn hearing screening (UNHS) and early hearing detection and intervention systems (EHDI). J. Commun. Disord. 2004, 37, 451–465. [Google Scholar] [CrossRef]
- Fairgray, E.; Purdy, S.C.; Smart, J.L. Effects of auditory-verbal therapy for school-aged children with hearing loss: An exploratory study. Volta Rev. 2010, 110, 407–433. [Google Scholar] [CrossRef]
- Rhoades, E.A.; Maclver-Lux, K.; Estabrooks, W. (Eds.) Auditory Verbal Therapy, for Young Children with Hearing Loss and Their Families, and the Practitioners Who Guide Them; Plural Publishing: San Diego, CA, USA, 2016. [Google Scholar]
- Rhoades, E.A. Research outcomes of auditory-verbal intervention: Is the approach justified? Deaf. Educ. Int. 2006, 8, 125–143. [Google Scholar] [CrossRef]
- AG Bell Academy for Listening and Spoken Language. Principles of Auditory-Verbal Therapy. 2007. Available online: http://www.listeningandspokenlanguage.org/AcademyDocument_id_563.html (accessed on 5 January 2021).
- Estabrooks, W. Auditory-Verbal Therapy and Practice; Alexander Graham Bell Association for the Deaf and the Hard of Hearing Inc.: Washington, DC, USA, 2006. [Google Scholar]
- Davis, A. Epidemiology of permanent childhood hearing impairment. In Pediatric Audiological Medicine, 2nd ed.; Newton, V.E., Ed.; John Wiley & Sons: Chichester, UK, 2009; pp. 1–26. [Google Scholar]
- Niparko, J.K. Spoken language development in children following cochlear implantation. JAMA 2010, 303, 1498–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AG Bell Academy for Listening and Spoken Language Knowledge Center. Early Intervention. Available online: http://www.listeningandspokenlanguage.org/Early_Intervention.html (accessed on 5 January 2021).
- Yoshinaga-Itano, C.; Sedey, A.L.; Coulter, D.K.; Mehl, A.L. Language of early- and later-identified children with hearing loss. Pediatrics 1998, 102, 1161–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Bain, L.; Steinberg, A.G. Parental decision making and the choice of communication modality for the child who is deaf. Arch. Pediatr. Adolesc. Med. 2003, 157, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, E.; Angus, D.; Durieux-Smith, A.; Graham, I.D.; Coyle, D. Parents’ needs following identification of childhood hearing loss. Am. J. Audiol. 2008, 17, 38–49. [Google Scholar] [CrossRef]
- Mitchell, R.E.; Karchmer, M.A. Chasing the mythical ten percent: Parental hearing status of deaf and hard of hearing students in the United States. Sign Lang. Stud. 2004, 4, 138–163. [Google Scholar] [CrossRef]
- Punch, R.; Hyde, M. Social participation of children and adolescents with cochlear implants: A qualitative analysis of parent, teacher, and child interviews. J. Deaf Stud. Deaf Educ. 2011, 16, 474–493. [Google Scholar] [CrossRef] [Green Version]
- Dornan, D.; Hickson, L.; Murdoch, B.; Houston, T. Longitudinal study of speech perception, speech, and language for children with hearing loss in an auditory-verbal therapy program. Volta Rev. 2009, 109, 61–85. [Google Scholar] [CrossRef]
- Jackson, C.W.; Schatschneide, C. Rate of language growth of children with hearing loss in an auditory-verbal early intervention program. Am. Ann. Deaf 2014, 158, 539–554. [Google Scholar] [CrossRef]
- Goldblat, E.; Pinto, O.Y. Academic outcomes of adolescents and young adults with hearing loss who received auditory-verbal therapy. Deaf. Educ. Int. 2017, 19, 126–133. [Google Scholar] [CrossRef]
- Dettman, S.; Wall, E.; Constantinescu, G.; Dowell, R. Communication outcomes for groups of children using cochlear implants enrolled in auditory-verbal, aural-oral, and bilingual-bicultural early intervention programs. Otol. Neurotol. 2013, 34, 451–459. [Google Scholar] [CrossRef]
- Percy-Smith, L.; Tønning, T.L.; Josvassen, J.L.; Mikkelsen, J.H.; Nissen, L.; Dieleman, E.; Hallstrøm, M.; Cayé-Thomasen, P. Auditory verbal habilitation is associated with improved outcome for children with cochlear implant. Cochlear Implant. Int. 2017, 19, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Percy-Smith, L.; Hallstrøm, M.; Josvassen, J.L.; Mikkelsen, J.H.; Nissen, L.; Dieleman, E.; Cayé-Thomasen, P. Differences and similarities in early vocabulary development between children with hearing aids and children with cochlear implant enrolled in 3-year auditory verbal intervention. Int. J. Pediatr. Otorhinolaryngol. 2018, 108, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.S.; Zwolan, T.A. Communication mode and speech and language outcomes of young cochlear implant recipients. Otol. Neurotol. 2019, 40, e975–e983. [Google Scholar] [CrossRef] [PubMed]
- Yanbay, E.; Hickson, L.; Scarinci, N.; Constantinescu, G.; Dettman, S.J. Language outcomes for children with cochlear implants enrolled in different communication programs. Cochlear Implant. Int. 2014, 15, 121–135. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dollaghan, C. The Handbook for the Evidence-Based Practice in Communication Disorders; Paul H. Brooks Publishing Co.: Baltimore, MD, USA, 2007. [Google Scholar]
- Kaipa, R.; Danser, M.L. Efficacy of auditory-verbal therapy in children with hearing impairment: A systematic review from 1993 to 2015. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 124–134. [Google Scholar] [CrossRef]
- American Speech-Language-Hearing Association. Evidence-Based Practice in Communication Disorders: An Introduction; Technical Report; ASHA: Rockville, MD, USA, 2004. [Google Scholar]
- Fulcher, A.; Purcell, A.A.; Baker, E.; Munro, N. Listen up: Children with early identified hearing loss achieve age-appropriate speech/language outcomes by 3years-of-age. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Sahli, A.S. Developments of children with hearing loss according to the age of diagnosis, amplification, and training in the early childhood period. Eur. Arch. Otorhinolaryngol. 2019, 276, 2457–2463. [Google Scholar] [CrossRef] [PubMed]
- Eriks-Brophy, A. Outcomes of auditory-verbal therapy: A review of the evidence and a call for action. Volta Rev. 2004, 104, 21–35. [Google Scholar]
- Rhoades, E.A.; Chisolm, T.H. Global language progress with an auditory-verbal approach for children who are deaf or hard of hearing. Volta Rev. 2000, 102, 5–25. [Google Scholar]
- Hogan, S.; Stokes, J.; White, E.; Tyszkiewicz, E.; Woolgar, A. An evaluation of Auditory Verbal therapy using the rate of early language development as an outcome measure. Deaf. Educ. Int. 2008, 10, 143–167. [Google Scholar] [CrossRef]


{kind=link}
| Study | Language | Design | Aim | Participants | Examined Areas of Language | Tools | Outcome |
|---|---|---|---|---|---|---|---|
| Percy-Smith et al. (2018) [23] | Danish | Longitudinal, comparative (3 years) | Early vocabulary development among children with CI compared with children with HA/Bahs (all enrolled in a 3-year AV program) | 36—CI, 19—HA | Receptive and productive vocabulary, language understanding | PPVT-4, Reynell, Viborg materialet | Children with HI progressed over a 3-year period, but they did not reach the same level as children with NH |
| Jackson and Schatschneider (2014) [19] | English | Longitudinal | The rate of language development of HI children in a private clinical intervention program, receiving weekly AVT | 12 boys, 12 girls | Expressive language, auditory comprehension | PLS-4 | Within-subjects comparisons revealed statistically significant improvements (p < 0.05) in both expressive language and auditory comprehension |
| Thomas and Zwolan (2019) [24] | English | Retrospective, comparative | Effect of communication mode (AV, OC, TC) on spoken language | 39—AV, 107—OC, 57—TC | Receptive and expressive language, speech intelligibility, reading | PPVT, EVT, WJPC, GFT-AAPS | Significantly higher scores for the AV group |
| Percy-Smith et al. (2017) [22] | Danish | Retrospective, comparative | Effect of (re)habilitation strategy on speech language for early cochlear-implanted children | 94—SH, 36—AV | Receptive and productive vocabulary, language understanding | PPVT-4, Reynell, Viborg materialet | Children in AV intervention outperformed children in SH in all tests of speech and language |
| Yanbay et al. (2014) [25] | English | Retrospective cohort | Differences in outcomes among children with cochlear implants enrolled in AO, AVT, and SS programs | 14—AO, 18—AV, 10—SS | Receptive vocabulary, auditory comprehension, expressive communication | PPVT, PLS-4, IRSAD, FPRS | No significant differences in language outcomes across the three groups |
| Dettman et al. (2013) [21] | English | Retrospective | The relative impact of early intervention approach on speech perception and language skills | 8—AV, 23—AO, 8—BB | Receptive vocabulary, speech perception (correct phonemes and correct words) | PPVT, CNC words, BKB sentences | AV group showed the least receptive vocabulary delay and highest mean score in CNC words—AV and AO groups performed equally well in BKB sentences |
| Fulcher et al. (2012) [30] | English | Prospective/retrospective, comparative | Examine the speech/language outcomes of children with HL by comparing them with respect to (i) early versus later-identified HL and (ii) degree of hearing loss | 45 early identified (12 months) and 49 late identified (>12 months) | Speech production, receptive vocabulary, receptive and expressive language | Goldman–Fristoe Test of Articulation-2; Sounds-in-Words (GFTA-2); PPVT-4, a receptive vocabulary measure; PLS-4 | By 3 years of age, 93% of all early-identified participants scored within normal limits for speech, 90% for understanding vocabulary, and 95% for receptive and expressive language |
| Sahli (2019) [31] | Turkish | Retrospective | Effect of hearing loss on early childhood in terms of development, instrumentation/amplification, and the starting age of training | 92 males, 77 females | Hearing, comprehension, and use of language, receptive, and expressive language capabilities | DDST-II | Children diagnosed before 6 months, instrumented between 3 and 6 months, and started with AVT revealed normal skills in their language capabilities |
| Aspects/Studies | Percy-Smith et al. (2018) | Jackson and Schatschneider (2014) | Thomas and Zwolan (2019) | Percy-Smith et al. (2017) | Yanbay et al. (2014) | Dettman et al. (2013) | Fulcher et al. (2012) | Sahli (2019) |
|---|---|---|---|---|---|---|---|---|
| Plausible rationale for the study? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the evidence from an experimental study? | No | No | Yes | Yes | Yes | Yes | Yes | No |
| Was there a control group or condition? | Yes | No | Yes | Yes | Yes | Yes | Yes | No |
| Was randomization used to create contrasting conditions? | No | No | No | No | No | No | No | No |
| Were methods and participants specified prospectively? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were patients recognizable at the beginning and end? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was treatment described clearly and implemented as intended? | No | Yes | No | Yes | Yes | Yes | Yes | No |
| Was the measure valid and reliable? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the outcome evaluated with blinding? | Νο | No | No | Νο | No | No | No | No |
| Nuisance variables | See text | See text | See text | See text | See text | See text | See text | See text |
| Was the finding statistically significant? | No | Yes | Yes | Yes | No | Partly | Yes | Yes |
| If the finding was not statistically significant, was statistical power adequate? | No | N/A | Ν/Α 1 | N/A | Yes | No | N/A | N/A |
| Was the finding important? | No | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Was the finding precise? 2 | No | No | Yes | Yes | Yes | Yes | No | No |
| Was there a substantial cost–benefit advantage? | UR | UR | UR 3 | UR | UR | UR | UR | UR |
| Evidence level | IIb | IIb | IIa | IIa | IIa | IIa | IIa | IIb |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binos, P.; Nirgianaki, E.; Psillas, G. How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review. Life 2021, 11, 239. https://doi.org/10.3390/life11030239
Binos P, Nirgianaki E, Psillas G. How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review. Life. 2021; 11(3):239. https://doi.org/10.3390/life11030239
Chicago/Turabian StyleBinos, Paris, Elina Nirgianaki, and George Psillas. 2021. "How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review" Life 11, no. 3: 239. https://doi.org/10.3390/life11030239
APA StyleBinos, P., Nirgianaki, E., & Psillas, G. (2021). How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review. Life, 11(3), 239. https://doi.org/10.3390/life11030239