
The Impact of a Lockdown for the COVID-19 Pandemic on Seasonal HbA1c Variation in Patients with Type 2 Diabetes

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
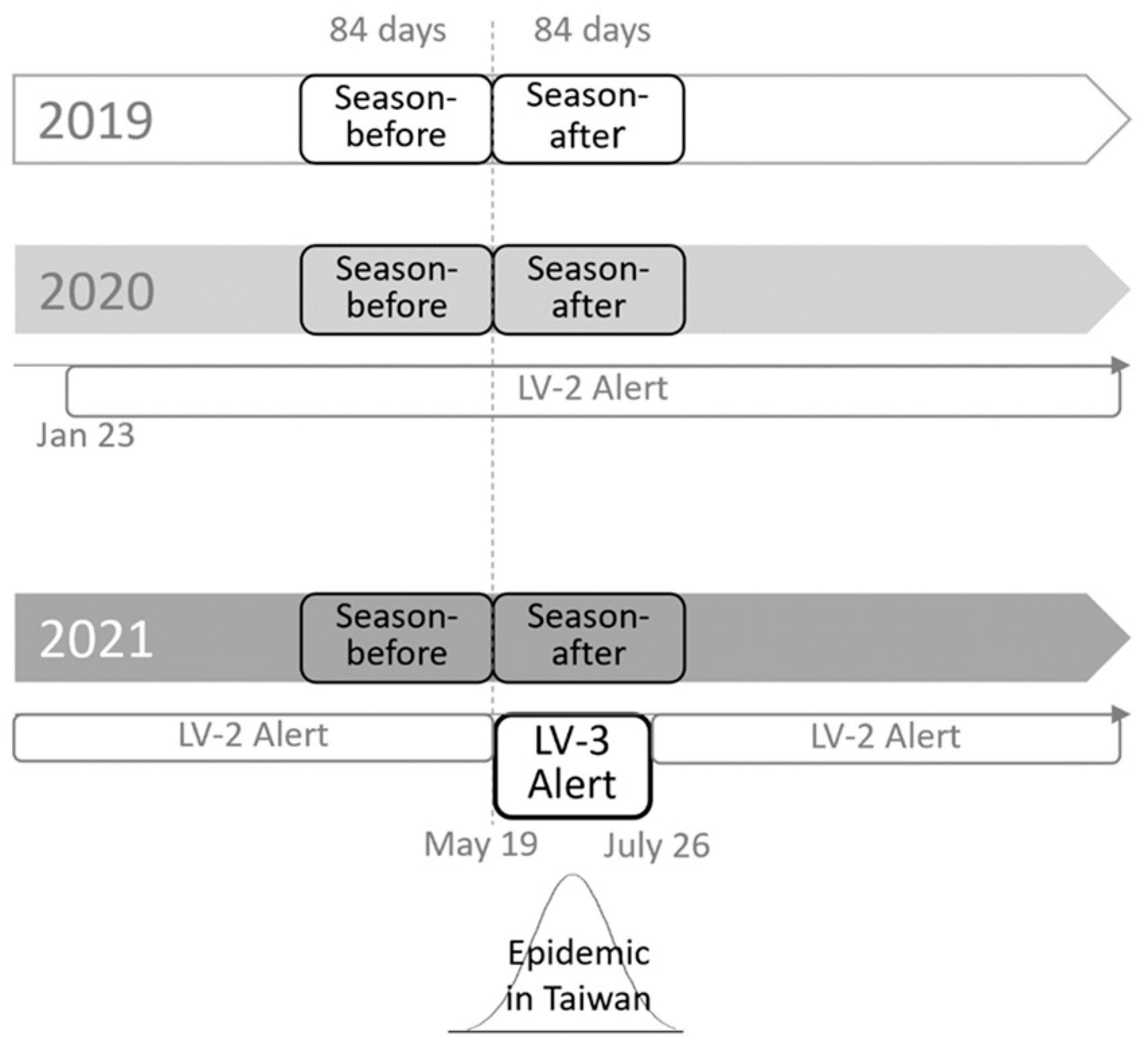
2.1. Study Design and Patients
2.2. Measurements
2.3. Statistical Analysis
2.4. Subgroup Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- Scott, E.S.; Jenkins, A.J.; Fulcher, G.R. Challenges of diabetes management during the COVID-19 pandemic. Med. J. Aust. 2020, 213, 56–57. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: Pandemic is having “severe” impact on non-communicable disease care, WHO survey finds. BMJ 2020, 369, m2210. [Google Scholar] [CrossRef]
- Ruiz-Roso, M.B.; Knott-Torcal, C.; Matilla-Escalante, D.C.; Garcimartín, A.; Sampedro-Nuñez, M.A.; Dávalos, A.; Marazuela, M. COVID-19 Lockdown and Changes of the Dietary Pattern and Physical Activity Habits in a Cohort of Patients with Type 2 Diabetes Mellitus. Nutrients 2020, 12, 2327. [Google Scholar] [CrossRef]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. 2020, 14, 917–920. [Google Scholar] [CrossRef]
- Takahara, M.; Watanabe, H.; Shiraiwa, T.; Maeno, Y.; Yamamoto, K.; Shiraiwa, Y.; Yoshida, Y.; Nishioka, N.; Katakami, N.; Shimomura, I. Lifestyle changes and their impact on glycemic control and weight control in patients with diabetes during the coronavirus disease 2019 pandemic in Japan. J. Diabetes Investig. 2022, 13, 375–385. [Google Scholar] [CrossRef]
- Tanaka, N.; Hamamoto, Y.; Kurotobi, Y.; Yamasaki, Y.; Nakatani, S.; Matsubara, M.; Haraguchi, T.; Yamaguchi, Y.; Izumi, K.; Fujita, Y.; et al. Lifestyle changes as a result of COVID-19 containment measures: Bodyweight and glycemic control in patients with diabetes in the Japanese declaration of a state of emergency. J. Diabetes Investig. 2021, 12, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Maruo, Y.; Irie, Y.; Obata, Y.; Takayama, K.; Yamaguchi, H.; Kosugi, M.; Hazama, Y.; Yasuda, T. Medium-term Influence of the Coronavirus Disease 2019 Pandemic on Patients with Diabetes: A Single-center Cross-sectional Study. Intern. Med. 2022, 61, 303–311. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Garofolo, M.; Aragona, M.; Rodia, C.; Falcetta, P.; Bertolotto, A.; Campi, F.; Del Prato, S.; Penno, G. Glycaemic control during the lockdown for COVID-19 in adults with type 1 diabetes: A meta-analysis of observational studies. Diabetes Res. Clin. Pract. 2021, 180, 109066. [Google Scholar] [CrossRef] [PubMed]
- Silverii, G.A.; Delli Poggi, C.; Dicembrini, I.; Monami, M.; Mannucci, E. Glucose control in diabetes during home confinement for the first pandemic wave of COVID-19: A meta-analysis of observational studies. Acta Diabetol. 2021, 58, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.; Stichling, S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetol. Metab. Syndr. 2021, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Wang, X.H.; Ojo, O.O.; Orjih, E.; Pavithran, N.; Adegboye, A.R.A.; Feng, Q.Q.; McCrone, P. The Effects of COVID-19 Lockdown on Glycaemic Control and Lipid Profile in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1095. [Google Scholar] [CrossRef] [PubMed]
- Wafa, I.A.; Pratama, N.R.; Sofia, N.F.; Anastasia, E.S.; Konstantin, T.; Wijaya, M.A.; Wiyono, M.R.; Djuari, L.; Novida, H. Impact of COVID-19 Lockdown on the Metabolic Control Parameters in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Metab. J. 2022, 46, 260–272. [Google Scholar] [CrossRef]
- O’Mahoney, L.L.; Highton, P.J.; Kudlek, L.; Morgan, J.; Lynch, R.; Schofield, E.; Sreejith, N.; Kapur, A.; Otunla, A.; Kerneis, S.; et al. The impact of the COVID-19 pandemic on glycaemic control in people with diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2022, 24, 1850–1860. [Google Scholar] [CrossRef]
- Tien, K.J.; Yang, C.Y.; Weng, S.F.; Liu, S.Y.; Hsieh, M.C.; Chou, C.W. The impact of ambient temperature on HbA1c in Taiwanese type 2 diabetic patients: The most vulnerable subgroup. J. Formos. Med. Assoc. 2016, 115, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Higgins, T.; Saw, S.; Sikaris, K.; Wiley, C.L.; Cembrowski, G.C.; Lyon, A.W.; Khajuria, A.; Tran, D. Seasonal variation in hemoglobin A1c: Is it the same in both hemispheres? J. Diabetes Sci. Technol. 2009, 3, 668–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakamoto, M.; Matsutani, D.; Minato, S.; Tsujimoto, Y.; Kayama, Y.; Takeda, N.; Ichikawa, S.; Horiuchi, R.; Utsunomiya, K.; Nishikawa, M. Seasonal Variations in the Achievement of Guideline Targets for HbA1c, Blood Pressure, and Cholesterol Among Patients with Type 2 Diabetes: A Nationwide Population-Based Study (ABC Study: JDDM49). Diabetes Care 2019, 2, 816–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.L.; Chang, H.H.; Chen, H.F.; Ku, L.E.; Chang, Y.H.; Shen, H.N.; Li, C.Y. Inverse relationship between ambient temperature and admissions for diabetic ketoacidosis and hyperglycemic hyperosmolar state: A 14-year time-series analysis. Environ. Int. 2016, 94, 642–648. [Google Scholar] [CrossRef]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers for Disease Control. COVID-19 Level 3 Alert in Effect around Taiwan through May 28. Available online: https://www.cna.com.tw/news/firstnews/202105155017.aspx (accessed on 14 August 2022).
- Gender Equality Committee of the Executive Yuan. Important Gender Statistics Database—Actual Coverage Rate of National Health Insurance. Available online: https://www.gender.ey.gov.tw/gecdb/Stat_Statistics_Query.aspx?sn=OU8Vo8ydhvbx1qKbUarVHw%3d%3d&statsn=u4cey DJ9iGzBYUGlJC0z7w%3d%3d&d=&n=163385 (accessed on 14 August 2022).
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Diabetes Association of the Republic of China Taiwan. Executive summary of the DAROC clinical practice guidelines for diabetes care—2018. J. Formos. Med. Assoc. 2020, 119, 577–586. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S144–S174. [Google Scholar] [CrossRef] [PubMed]
- Pivarnik, J.M.; Reeves, M.J.; Rafferty, A.P. Seasonal variation in adult leisure-time physical activity. Med. Sci. Sports Exerc. 2003, 35, 1004–1008. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, K.; Chan, C.; Da Costa, D.; Pilote, L.; De Civita, M.; Ross, N.; Strachan, I.; Sigal, R.; Joseph, L. Walking behaviour and glycemic control in type 2 diabetes: Seasonal and gender differences—Study design and methods. Cardiovasc. Diabetol. 2007, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Shahar, D.R.; Yerushalmi, N.; Lubin, F.; Froom, P.; Shahar, A.; Kristal-Boneh, E. Seasonal variations in dietary intake affect the consistency of dietary assessment. Eur. J. Epidemiol. 2001, 17, 129–133. [Google Scholar] [CrossRef]
- Chen, H.S.; Jap, T.S.; Chen, R.L.; Lin, H.D. A prospective study of glycemic control during holiday time in type 2 diabetic patients. Diabetes Care 2004, 27, 326–330. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, D.E.; Little, R.R.; Lorenz, R.A.; Malone, J.I.; Nathan, D.; Peterson, C.M.; Sacks, D.B. Tests of glycemia in diabetes. Diabetes Care 2004, 27, 1761–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takebayashi, K.; Yamauchi, M.; Hara, K.; Tsuchiya, T.; Hashimoto, K. Seasonal variations and the influence of COVID-19 pandemic on hemoglobin A1c, glycoalbumin, and low-density lipoprotein cholesterol. Diabetol. Int. 2022, 13, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Khare, J.; Jindal, S. Observational study on Effect of Lock Down due to COVID 19 on glycemic control in patients with Diabetes: Experience from Central India. Diabetes Metab. Syndr. 2020, 14, 1571–1574. [Google Scholar] [CrossRef]
- Xue, T.; Li, Q.; Zhang, Q.; Lin, W.; Wen, J.; Li, L.; Chen, G. Blood glucose levels in elderly subjects with type 2 diabetes during COVID-19 outbreak: A retrospective study in a single center. medRxiv 2020. [Google Scholar] [CrossRef]
- Park, S.D.; Kim, S.W.; Moon, J.S.; Lee, Y.Y.; Cho, N.H.; Lee, J.H.; Jeon, J.H.; Choi, Y.K.; Kim, M.K.; Park, K.G. Impact of Social Distancing Due to Coronavirus Disease 2019 on the Changes in Glycosylated Hemoglobin Level in People with Type 2 Diabetes Mellitus. Diabetes Metab. J. 2021, 45, 109–114. [Google Scholar] [CrossRef]
- Psoma, O.; Papachristoforou, E.; Kountouri, A.; Balampanis, K.; Stergiou, A.; Lambadiari, V.; Liatis, S.; Tsimihodimos, V. Effect of COVID-19-associated lockdown on the metabolic control of patients with type 2 diabetes. J. Diabetes Complicat. 2020, 34, 107756. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Hiteshi, P.; Bhansali, A. Improved glycemic control amongst people with long-standing diabetes during COVID-19 lockdown: A prospective, observational, nested cohort study. Int. J. Diabetes Dev. Ctries. 2020, 40, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Bonora, B.M.; Morieri, M.L.; Avogaro, A.; Fadini, G.P. The Toll of Lockdown Against COVID-19 on Diabetes Outpatient Care: Analysis from an Outbreak Area in Northeast Italy. Diabetes Care 2021, 44, e18–e21. [Google Scholar] [CrossRef]
- Önmez, A.; Gamsızkan, Z.; Özdemir, Ş.; Kesikbaş, E.; Gökosmanoğlu, F.; Torun, S.; Cinemre, H. The effect of COVID-19 lockdown on glycemic control in patients with type 2 diabetes mellitus in Turkey. Diabetes Metab. Syndr. 2020, 14, 1963–1966. [Google Scholar] [CrossRef]
- Ruissen, M.M.; Regeer, H.; Landstra, C.P.; Schroijen, M.; Jazet, I.; Nijhoff, M.F.; Pijl, H.; Ballieux, B.E.P.B.; Dekkers, O.; Huisman, S.D.; et al. Increased stress, weight gain and less exercise in relation to glycemic control in people with type 1 and type 2 diabetes during the COVID-19 pandemic. BMJ Open Diabetes Res. Care 2021, 9, e002035. [Google Scholar] [CrossRef]
- Wang, C.Y.; Tu, S.T.; Sheu, W.H.; Chen, I.C.; Chuang, L.M.; Wu, M.S.; Yu, C.J. National survey of ABC (A1C, blood pressure, cholesterol) of Diabetes Health Promotion Institutes in Taiwan: 2002-2018. J. Formos. Med. Assoc. 2018, 117, 952–954. [Google Scholar] [CrossRef]
- Yu, N.C.; Su, H.Y.; Chiou, S.T.; Yeh, M.C.; Yeh, S.W.; Tzeng, M.S.; Sheu, W.H. Trends of ABC control 2006–2011: A National Survey of Diabetes Health Promotion Institutes in Taiwan. Diabetes Res. Clin. Pract. 2013, 99, 112–119. [Google Scholar] [CrossRef]
- Yu, N.C.; Su, H.Y.; Tsai, S.T.; Lin, B.J.; Shiu, R.S.; Hsieh, Y.C.; Sheu, W.H. ABC control of diabetes: Survey data from National Diabetes Health Promotion Centers in Taiwan. Diabetes Res. Clin. Pract. 2009, 84, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Tai, T.Y. Long-term glycemic control by a diabetes case-management program and the challenges of diabetes care in Taiwan. Diabetes Res Clin. Pract. 2014, 106, S328–S332. [Google Scholar] [CrossRef]
- Ke, H.T.; Hsieh, C.L.; Cheng, W.J. Physical Activity, Dietary Behavior, and Body Weight Changes during the COVID-19 Nationwide Level 3 Alert in Taiwan: Results of a Taiwanese Online Survey. Nutrients 2022, 14, 4941. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.C.; Yang, H.C.; Chang, H.Y.; Yeh, C.J.; Chen, H.H.; Huang, K.C.; Pan, W.H. Morbid obesity in Taiwan: Prevalence, trends, associated social demographics, and lifestyle factors. PLoS ONE 2017, 12, e0169577. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics | Cohort-2019 | Cohort-2020 | Cohort-2021 | p † |
|---|---|---|---|---|
| (n = 9111) | (n = 9078) | (n = 8663) | ||
| Age (years) | 65.3 ± 12.6 | 65.0 ± 12.4 | 64.9 ± 12.2 | 0.154 |
| Female, n (%) | 4109 (45.1) | 4044 (44.5) * | 3734 (43.1) | 0.022 |
| Height (cm) | 162.0 ± 6.4 | 161.9 ± 7.4 * | 162.2 ± 7.2 | 0.012 |
| Weight (kg) | 68.2 ± 10.2 * | 69.0 ± 12.0 | 69.3 ± 11.5 | <0.001 |
| BMI (kg/m2) | 26.0 ± 3.2 * | 26.3 ± 3.8 | 26.3 ± 3.6 | <0.001 |
| SBP (mmHg) | 131.8 ± 14.1 * | 133.8 ± 16.9 | 134.0 ± 15.4 | <0.001 |
| DBP (mmHg) | 71.9 ± 9.5 * | 73.4 ± 11.2 | 73.3 ± 9.7 | <0.001 |
| HR (beat/min) | 81.9 ± 10.1 * | 82.9 ± 11.9 * | 84.0 ± 10.8 | <0.001 |
| eGFR (mL/min/1.73 m2) | 71.08 ± 25.76 * | 71.03 ± 25.32 * | 65.81 ± 22.88 | <0.001 |
| LDL cholesterol (mg/dL) | 87.0 ± 22.3 * | 85.8 ± 21.5 | 85.1 ± 22.1 | <0.001 |
| TG (mg/dL) | 151.2 ± 101.2 * | 154.9 ± 112.5 * | 147.1 ± 106.9 | <0.001 |
| GPT (U/L) | 26.8 ± 18.5 | 27.2 ± 18.6 * | 26.3 ± 16.4 | <0.001 |
| Hypertension, n (%) | 6555 (71.9) * | 6458 (71.1) * | 5609 (64.7) | 0.003 |
| Anti-hypertensive drug use, n (%) | 5724 (62.8) | 5696 (62.7) | 5423 (62.6) | 0.952 |
| Insulin use, n (%) | 1875 (20.6) | 1843 (20.3) | 1721 (19.9) | 0.492 |
| OHA use, n (%) | 7957 (87.3) | 7942 (87.5) | 7599 (87.7) | 0.739 |
| GLP-1 RA use, n (%) | 445 (4.9) * | 449 (4.9) * | 502 (5.8) | 0.010 |
| Variables | Cohort-2019 | Cohort-2020 | Cohort-2021 | p † |
|---|---|---|---|---|
| (n = 9111) | (n = 9078) | (n = 8663) | ||
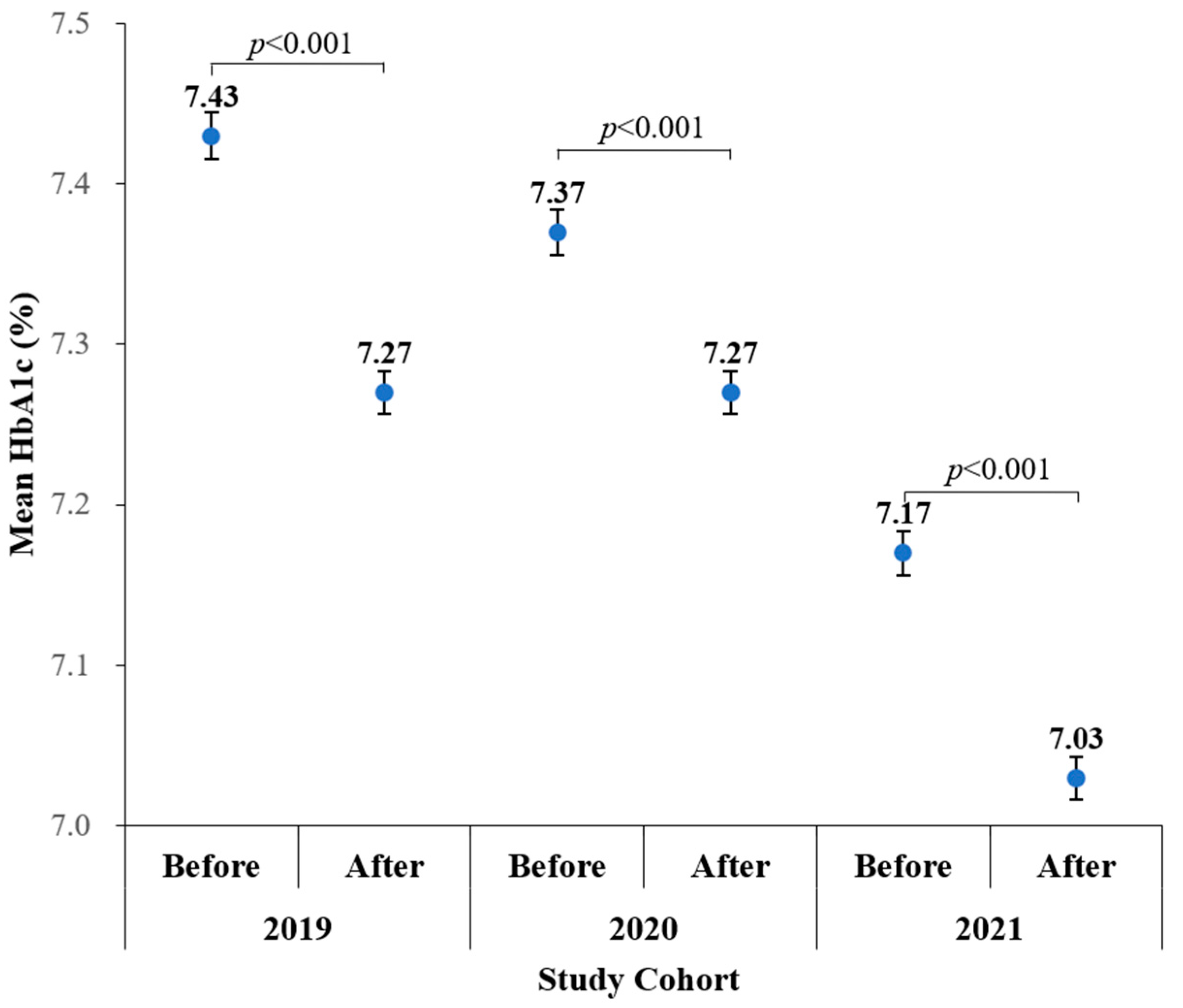
| HbA1c-before (%) | 7.43 ± 1.38 * | 7.37 ± 1.34 * | 7.17 ± 1.29 | <0.001 † |
| HbA1c-after (%) | 7.27 ± 1.27 * | 7.27 ± 1.28 * | 7.03 ± 1.22 | <0.001 † |
| ΔHbA1c (%) | −0.16 ± 0.83 | −0.10 ± 0.83 * | −0.14 ± 0.76 | 0.001 |
| Parameters | Unit of β | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|---|
| β | 95% CI | p | β | 95% CI | p | ||
| Year | Cohort-2019 vs. 2021 | −0.024 | −0.048, −0.001 | 0.040 | −0.047 | −0.073, −0.021 | <0.001 |
| Cohort-2020 vs. 2021 | 0.035 | 0.011, 0.058 | 0.004 | 0.009 | −0.017, 0.035 | 0.500 | |
| Age | per 10 years increase | 0.008 | −0.003, 0.018 | 0.138 | |||
| Sex | Male vs. Female | −0.041 | −0.061, −0.02 | <0.001 | |||
| BMI | ≥24 vs. <24 (kg/m2) | 0.014 | −0.011, 0.039 | 0.264 | |||
| LDL cholesterol | ≥100 vs. <100 (mg/dL) | −0.020 | −0.052, 0.012 | 0.224 | |||
| TG | ≥150 vs. <150 (mg/dL) | 0.050 | 0.028, 0.072 | <0.001 | |||
| SBP | ≥140 vs. <140 (mmHg) | 0.036 | 0.013, 0.060 | 0.003 | |||
| eGFR | <60 vs ≥60 (mL/min/1.73 m2) | 0.029 | 0.003, 0.055 | 0.027 | |||
| GPT | per 10 U/L increase | 0.017 | 0.010, 0.023 | <0.001 | |||
| HR | per 10 beat/min increase | −0.001 | −0.010, 0.008 | 0.851 | |||
| Antihypertensive drug | Use vs. no | 0.043 | 0.021, 0.065 | <0.001 | |||
| Insulin | Use vs. no | −0.120 | −0.154, −0.087 | <0.001 | |||
| OHA | Use vs. no | −0.083 | −0.110, −0.055 | <0.001 | |||
| GLP-1 RA | Use vs. no | 0.023 | −0.037, 0.083 | 0.456 | |||
| Basic Characteristics | Total (n = 3720) |
|---|---|
| Age (years) | 63.9 ± 11.8 |
| Female, n (%) | 1687 (45.4) |
| Height (cm) | 162.0 ± 9.0 |
| Weight (kg) | 69.9 ± 14.6 |
| BMI (kg/m2) | 26.5 ± 4.59 |
| SBP (mmHg) | 136.1 ± 19.4 |
| DBP (mmHg) | 73.8 ± 12.0 |
| HR (beat/min) | 84.5 ± 13.2 |
| eGFR (mL/min/1.73 m2) | 70.92 ± 24.71 |
| LDL cholesterol (mg/dL) | 84.06 ± 26.63 |
| TG (mg/dL) | 133.5 ± 109.2 |
| GPT (U/L) | 24.9 ± 16.4 |
| Hypertension, n (%) | 2547 (68.5) |
| Anti-hypertensive drug use, n (%) | 2407 (64.7) |
| Insulin use, n (%) | 804 (21.6) |
| OHA use, n (%) | 3504 (94.2) |
| GLP-1 RA use, n (%) | 325 (8.7) |
| Variables | Year (n = 3720) | |||
|---|---|---|---|---|
| 2019 | 2020 | 2021 | p-For-Trend † | |
| HbA1c-before (%) | 7.41 ± 1.24 * | 7.37 ± 1.20 * | 7.18 ± 1.17 | <0.001 |
| HbA1c-after (%) | 7.27 ± 1.16 * | 7.28 ± 1.14 * | 7.07 ± 1.13 | <0.001 |
| ΔHbA1c (%) | −0.15 ± 0.73 * | −0.09 ± 0.68 | −0.11 ± 0.66 | 0.034 |
| ΔHbA1c (%) | Univariable Analysis | ||
|---|---|---|---|
| β | 95% CI | p | |
| Cohort-2019 vs. 2021 | −0.037 | −0.068, −0.006 | 0.019 |
| Cohort-2020 vs. 2021 | 0.022 | −0.008, 0.051 | 0.156 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Y.-C.; Li, Y.-H.; Liu, H.-C.; Hsu, C.-Y.; Chang, W.-J.; Lee, I.-T.; Lu, C.-L. The Impact of a Lockdown for the COVID-19 Pandemic on Seasonal HbA1c Variation in Patients with Type 2 Diabetes. Life 2023, 13, 763. https://doi.org/10.3390/life13030763
Cheng Y-C, Li Y-H, Liu H-C, Hsu C-Y, Chang W-J, Lee I-T, Lu C-L. The Impact of a Lockdown for the COVID-19 Pandemic on Seasonal HbA1c Variation in Patients with Type 2 Diabetes. Life. 2023; 13(3):763. https://doi.org/10.3390/life13030763
Chicago/Turabian StyleCheng, Yu-Cheng, Yu-Hsuan Li, Hsiu-Chen Liu, Chiann-Yi Hsu, Wan-Jen Chang, I-Te Lee, and Chin-Li Lu. 2023. "The Impact of a Lockdown for the COVID-19 Pandemic on Seasonal HbA1c Variation in Patients with Type 2 Diabetes" Life 13, no. 3: 763. https://doi.org/10.3390/life13030763
APA StyleCheng, Y. -C., Li, Y. -H., Liu, H. -C., Hsu, C. -Y., Chang, W. -J., Lee, I. -T., & Lu, C. -L. (2023). The Impact of a Lockdown for the COVID-19 Pandemic on Seasonal HbA1c Variation in Patients with Type 2 Diabetes. Life, 13(3), 763. https://doi.org/10.3390/life13030763