
Antidepressant Treatment and Manic Switch in Bipolar I Disorder: A Clinical and Molecular Genetic Study


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Characteristics
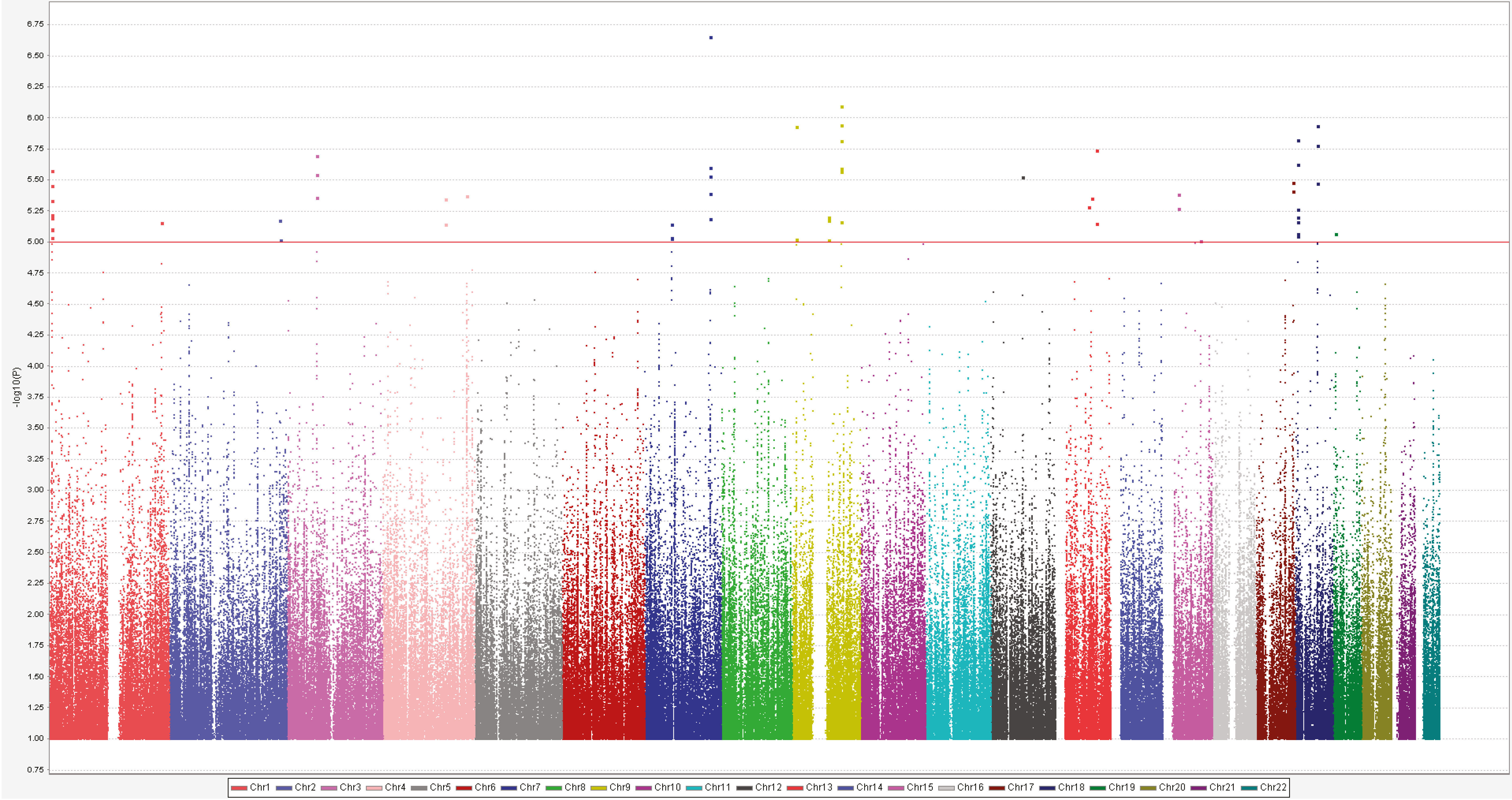
2.2. Genome-Wide Association Study
3. Discussion
4. Materials and Methods
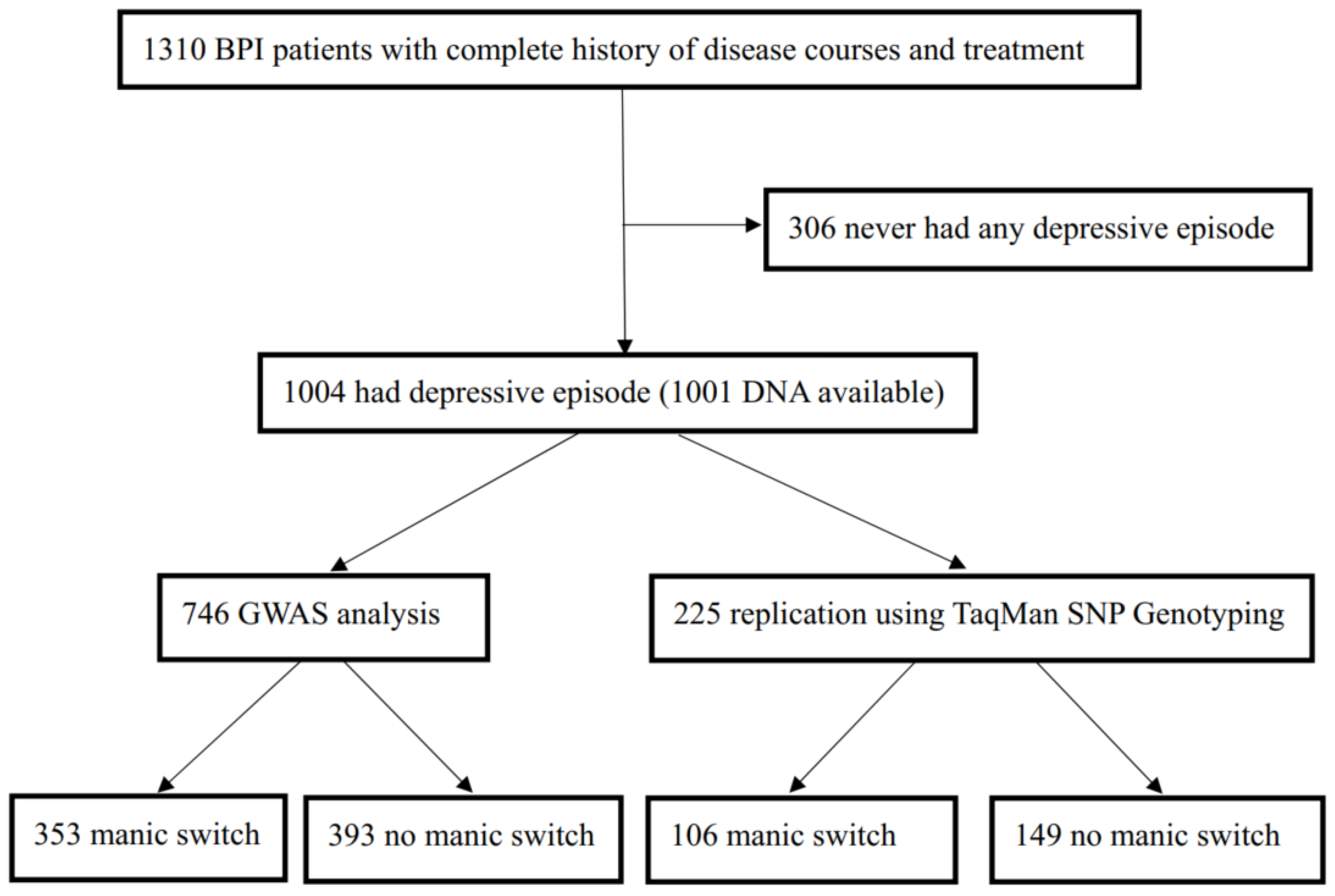
4.1. Study Patients
4.2. Assessments
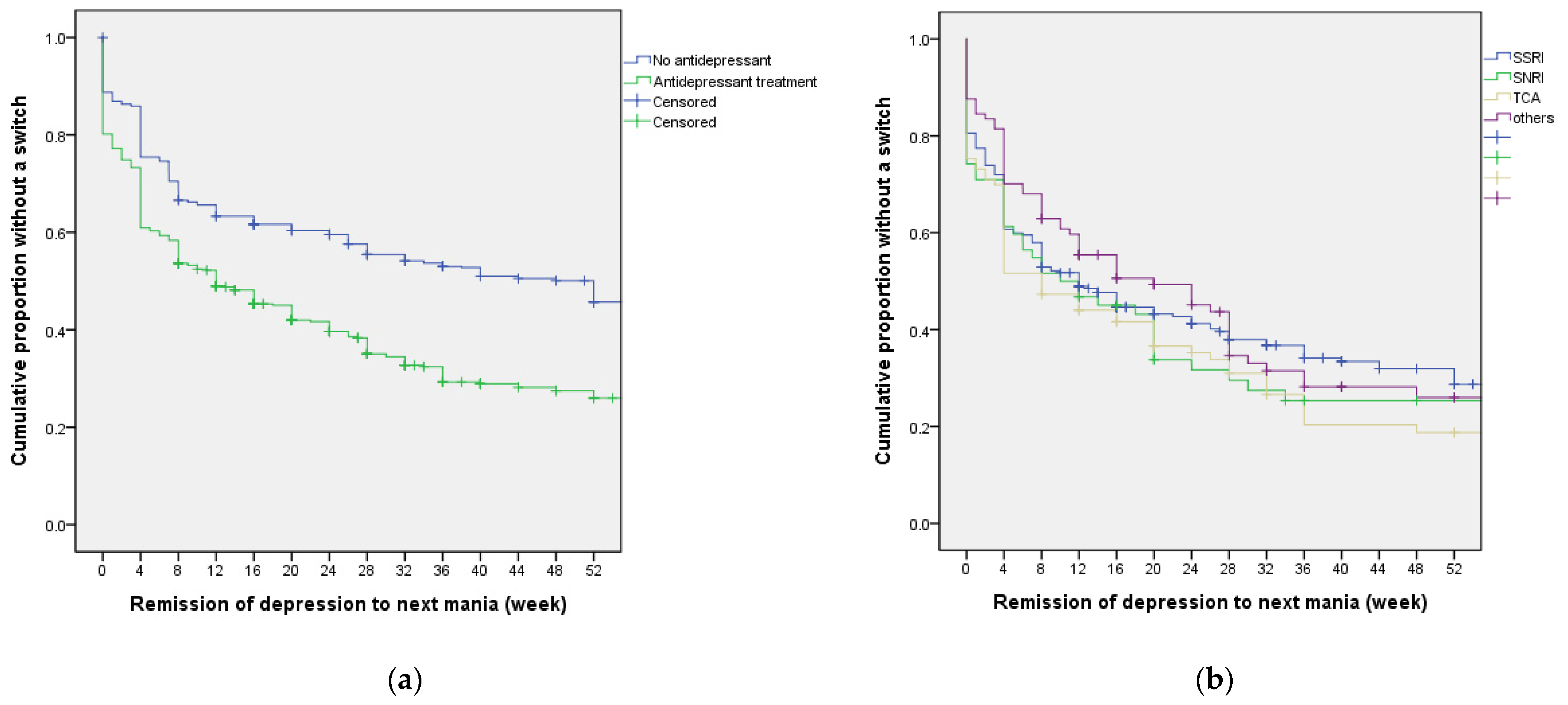
4.3. Antidepressant Treatment and Affective Switch
4.4. Genome-Wide Association Study (GWAS)
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muller-Oerlinghausen, B.; Berghofer, A.; Bauer, M. Bipolar disorder. Lancet 2002, 359, 241–247. [Google Scholar] [CrossRef]
- Miller, S.; Dell’Osso, B.; Ketter, T.A. The prevalence and burden of bipolar depression. J. Affect. Disord. 2014, 169 (Suppl. S1), S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Forte, A.; Baldessarini, R.J.; Tondo, L.; Vazquez, G.H.; Pompili, M.; Girardi, P. Long-term morbidity in bipolar-I, bipolar-II, and unipolar major depressive disorders. J. Affect. Disord. 2015, 178, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Grunze, H.; Vieta, E.; Goodwin, G.M.; Bowden, C.; Licht, R.W.; Möller, H.J.; Kasper, S.; WFSBP Task Force on Treatment Guidelines for Bipolar Disorders. The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Bipolar Disorders: Update 2010 on the treatment of acute bipolar depression. World J. Biol. Psychiatry 2010, 11, 81–109. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J.; Tondo, L.; Vázquez, G.H. Pharmacological treatment of adult bipolar disorder. Mol. Psychiatry 2019, 24, 198–217. [Google Scholar] [CrossRef]
- Baldessarini, R.J.; Leahy, L.; Arcona, S.; Gause, D.; Zhang, W.; Hennen, J. Patterns of psychotropic drug prescription for U.S. patients with diagnoses of bipolar disorders. Psychiatric Serv. 2007, 58, 85–91. [Google Scholar] [CrossRef]
- Viktorin, A.; Lichtenstein, P.; Thase, M.E.; Larsson, H.; Lundholm, C.; Magnusson, P.K.; Landén, M. The risk of switch to mania in patients with bipolar disorder during treatment with an antidepressant alone and in combination with a mood stabilizer. Am. J. Psychiatry 2014, 171, 1067–1073. [Google Scholar] [CrossRef] [Green Version]
- Lyall, L.M.; Penades, N.; Smith, D.J. Changes in prescribing for bipolar disorder between 2009 and 2016: National-level data linkage study in Scotland. Br. J. Psychiatry 2019, 215, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Ghaemi, S.N.; Wingo, A.P.; Filkowski, M.A.; Baldessarini, R.J. Long-term antidepressant treatment in bipolar disorder: Meta-analyses of benefits and risks. Acta. Psychiatr. Scand. 2008, 118, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Sachs, G.S.; Nierenberg, A.A.; Calabrese, J.R.; Marangell, L.B.; Wisniewski, S.R.; Gyulai, L.; Friedman, E.S.; Bowden, C.L.; Fossey, M.D.; Ostacher, M.J.; et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N. Engl. J. Med. 2007, 356, 1711–1722. [Google Scholar] [CrossRef] [Green Version]
- Sidor, M.M.; Macqueen, G.M. Antidepressants for the acute treatment of bipolar depression: A systematic review and meta-analysis. J. Clin. Psychiatry 2011, 72, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Ostacher, M.J.; Goldberg, J.F.; Miklowitz, D.J.; Friedman, E.; Calabrese, J.; Thase, M.E.; Sachs, G.S. Transition to mania during treatment of bipolar depression. Neuropsychopharmacology 2010, 35, 2545–2552. [Google Scholar] [CrossRef] [Green Version]
- McGirr, A.; Vohringer, P.A.; Ghaemi, S.N.; Lam, R.W.; Yatham, L.N. Safety and efficacy of adjunctive second-generation antidepressant therapy with a mood stabiliser or an atypical antipsychotic in acute bipolar depression: A systematic review and meta-analysis of randomised placebo-controlled trials. Lancet Psychiatry 2016, 3, 1138–1146. [Google Scholar] [CrossRef]
- Angst, J. Switch from depression to mania, or from mania to depression: Role of psychotropic drugs. Psychopharmacol. Bull. 1987, 23, 66–67. [Google Scholar] [PubMed]
- Henry, C.; Sorbara, F.; Lacoste, J.; Gindre, C.; Leboyer, M. Antidepressant-induced mania in bipolar patients: Identification of risk factors. J. Clin. Psychiatry 2001, 62, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Post, R.M.; Altshuler, L.L.; Frye, M.A.; Suppes, T.; Rush, A.J.; Keck, P.E., Jr.; McElroy, S.L.; Denicoff, K.D.; Leverich, G.S.; Kupka, R.; et al. Rate of switch in bipolar patients prospectively treated with second-generation antidepressants as augmentation to mood stabilizers. Bipolar Disord. 2001, 3, 259–265. [Google Scholar] [CrossRef]
- Post, R.M.; Leverich, G.S.; Nolen, W.A.; Kupka, R.W.; Altshuler, L.L.; Frye, M.A.; Suppes, T.; McElroy, S.; Keck, P.; Grunze, H.; et al. A re-evaluation of the role of antidepressants in the treatment of bipolar depression: Data from the Stanley Foundation Bipolar Network. Bipolar Disord. 2003, 5, 396–406. [Google Scholar] [CrossRef]
- Leverich, G.S.; Altshuler, L.L.; Frye, M.A.; Suppes, T.; McElroy, S.L.; Keck, P.E., Jr.; Kupka, R.W.; Denicoff, K.D.; Nolen, W.A.; Grunze, H.; et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am. J. Psychiatry 2006, 163, 232–239. [Google Scholar] [CrossRef]
- Bauer, M.; Rasgon, N.; Grof, P.; Glenn, T.; Lapp, M.; Marsh, W.; Munoz, R.; Suwalska, A.; Baethge, C.; Bschor, T.; et al. Do antidepressants influence mood patterns? A naturalistic study in bipolar disorder. Eur. Psychiatry 2006, 21, 262–269. [Google Scholar] [CrossRef]
- Rybakowski, J.K. Genetic influences on response to mood stabilizers in bipolar disorder: Current status of knowledge. CNS Drugs 2013, 27, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Amare, A.T.; Schubert, K.O.; Baune, B.T. Pharmacogenomics in the treatment of mood disorders: Strategies and Opportunities for personalized psychiatry. EPMA J. 2017, 8, 211–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlis, R.H.; Smoller, J.W.; Ferreira, M.A.; McQuillin, A.; Bass, N.; Lawrence, J.; Sachs, G.S.; Nimgaonkar, V.; Scolnick, E.M.; Gurling, H.; et al. A genomewide association study of response to lithium for prevention of recurrence in bipolar disorder. Am. J. Psychiatry 2009, 166, 718–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squassina, A.; Manchia, M.; Borg, J.; Congiu, D.; Costa, M.; Georgitsi, M.; Chillotti, C.; Ardau, R.; Mitropoulos, K.; Severino, G.; et al. Evidence for association of an ACCN1 gene variant with response to lithium treatment in Sardinian patients with bipolar disorder. Pharmacogenomics 2011, 12, 1559–1569. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Lee, C.S.; Lee, M.T.M.; Ouyang, W.C.; Chen, C.C.; Chong, M.Y.; Wu, J.Y.; Tan, H.K.L.; Lee, Y.C.; Chuo, L.J.; et al. Variant GADL1 and response to lithium therapy in bipolar I disorder. N. Eng. J. Med. 2014, 370, 119–128. [Google Scholar] [CrossRef]
- Hou, L.; Heilbronner, U.; Degenhardt, F.; Adli, M.; Akiyama, K.; Akula, N.; Ardau, R.; Arias, B.; Backlund, L.; Banzato, C.E.M.; et al. Genetic variants associated with response to lithium treatment in bipolar disorder: A genome-wide association study. Lancet 2016, 387, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Biernacka, J.M.; McElroy, S.L.; Crow, S.; Sharp, A.; Benitez, J.; Veldic, M.; Kung, S.; Cunningham, J.M.; Post, R.M.; Mrazek, D.; et al. Pharmacogenomics of antidepressant induced mania: A review and meta-analysis of the serotonin transporter gene (5HTTLPR) association. J. Affect. Disord. 2012, 136, e21–e29. [Google Scholar] [CrossRef]
- Truman, C.J.; Goldberg, J.F.; Ghaemi, S.N.; Baldassano, C.F.; Wisniewski, S.R.; Dennehy, E.B.; Thase, M.E.; Sachs, G.S. Self-reported history of manic/hypomanic switch associated with antidepressant use: Data from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). J. Clin. Psychiatry 2007, 68, 1472–1479. [Google Scholar] [CrossRef] [Green Version]
- Koszewska, I.; Rybakowski, J.K. Antidepressant-induced mood conversions in bipolar disorder: A retrospective study of tricyclic versus non-tricyclic antidepressant drugs. Neuropsychobiology 2009, 59, 12–16. [Google Scholar] [CrossRef]
- Fela-Thomas, A.L.; Olotu, O.S.; Esan, O. Risk of manic switch with antidepressants use in patients with bipolar disorder in a Nigerian neuropsychiatric hospital. S. Afr. J. Psychiatry 2018, 24, 1215. [Google Scholar] [CrossRef]
- Goldberg, J.F.; Truman, C.J. Antidepressant-induced mania: An overview of current controversies. Bipolar Disord. 2003, 5, 407–420. [Google Scholar] [CrossRef]
- Mundo, E.; Cattaneo, E.; Russo, M.; Altamura, A.C. Clinical variables related to antidepressant-induced mania in bipolar disorder. J. Affect. Disord. 2006, 92, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Tondo, L.; Vazquez, G.; Baldessarini, R.J. Mania associated with antidepressant treatment: Comprehensive meta-analytic review. Acta Psychiatr. Scand. 2010, 121, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Pacchiarotti, I.; Bond, D.J.; Baldessarini, R.J.; Nolen, W.A.; Grunze, H.; Licht, R.W.; Post, R.M.; Berk, M.; Goodwin, G.M.; Sachs, G.S.; et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am. J. Psychiatry 2013, 170, 1249–1262. [Google Scholar] [CrossRef] [PubMed]
- Serretti, A.; Artioli, P.; Zanardi, R.; Rossini, D. Clinical features of antidepressant associated manic and hypomanic switches in bipolar disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2003, 27, 751–757. [Google Scholar] [CrossRef]
- Cannon, D.M.; Carson, R.E.; Nugent, A.C.; Eckelman, W.C.; Kiesewetter, D.O.; Williams, J.; Rollis, D.; Drevets, M.; Gandhi, S.; Solorio, G.; et al. Reduced muscarinic type 2 receptor binding in subjects with bipolar disorder. Arch. Gen. Psychiatry 2006, 63, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, A.S.; Scarr, E.; McLean, C.; Sundram, S.; Dean, B. Decreased muscarinic receptor binding in the frontal cortex of bipolar disorder and major depressive disorder subjects. J. Affect. Disord. 2009, 116, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Janowsky, D.S.; El-Yousef, M.K.; Davis, J.M.; Sekerke, H.J. A cholinergic-adrenergic hypothesis of mania and depression. Lancet 1972, 2, 632–635. [Google Scholar] [CrossRef]
- Gibbons, A.S.; Jeon, W.J.; Scarr, E.; Dean, B. Changes in muscarinic m2 receptor levels in the cortex of subjects with bipolar disorder and major depressive disorder and in rats after treatment with mood stabilisers and antidepressants. Int. J. Neuropsychopharmacol. 2016, 19, pyv118. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.T.; Chen, C.H.; Lee, C.S.; Chen, C.C.; Chong, M.Y.; Ouyang, W.C.; Chiu, N.Y.; Chuo, L.J.; Chen, C.Y.; Tan, H.K.L.; et al. Genome-wide association study of bipolar I disorder in the Han Chinese population. Mol. Psychiatry 2011, 16, 548–556. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Cheng, A.T.; Tien, A.Y.; Chang, C.J.; Brugha, T.S.; Cooper, J.E.; Lee, C.S.; Compton, W.; Liu, C.Y.; Yu, W.Y.; Chen, H.M. Cross-cultural implementation of a Chinese version of the Schedules for Clinical Assessment in Neuropsychiatry (SCAN) in Taiwan. Br. J. Psychiatry 2001, 178, 567–572. [Google Scholar] [CrossRef]
- Tohen, M.; Frank, E.; Bowden, C.L.; Colom, F.; Ghaemi, S.N.; Yatham, L.N.; Malhi, G.S.; Calabrese, J.R.; Nolen, W.A.; Vieta, E.; et al. The International Society for Bipolar Disorders (ISBD) Task Force report on the nomenclature of course and outcome in bipolar disorders. Bipolar Disord. 2009, 11, 453–473. [Google Scholar] [CrossRef] [PubMed]
- Howie, B.N.; Donnelly, P.; Marchini, J. A flexible and accurate genotype imputation method for the next generation of genome-wide association studies. PLoS Genet. 2009, 5, e1000529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howie, B.; Marchini, J.; Stephens, M. Genotype imputation with thousands of genomes. G3 Genes Genomes Genet. 2011, 1, 457–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchini, J.; Howie, B. Genotype imputation for genome-wide association studies. Nat. Rev. Genet. 2010, 11, 499–511. [Google Scholar] [CrossRef]
- 1000 Genomes Project Consortium. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| (a) Antidepressant Treatment | ||||
| Total | Treatment with antidepressants | |||
| N = 1004 | No (N = 493) | Yes (N = 511) | p Value | |
| Female gender, N (%) | 562 (56.0) | 262 (53.1) | 300 (58.7) | 0.086 |
| Age at first depressive episode, mean (SD) | 30.7 (12.5) | 29.7 (12.0) | 31.6 (12.8) | 0.017 |
| Subsequent manic episode, N (%) | 765 (76.2) | 384 (77.9) | 381 (74.6) | 0.215 |
| Manic switch or recurrence within 1 year, N (%) | 603 (60.1) | 259 (52.5) | 344 (67.3) | <0.001 |
| Manic switch, N (%) | 399 (39.7) | 163 (33.1) | 236 (46.2) | <0.001 |
| (b) Manic Switch | ||||
| Manic switch | ||||
| No (N = 605) | Yes (N = 399) | |||
| Female gender, N (%) | 562 (56.0) | 336 (55.5) | 226 (56.6) | 0.730 |
| Age at first depressive episode, mean (SD) | 30.7 (12.5) | 30.9 (12.2) | 30.4 (12.9) | 0.017 |
| Types of antidepressants | ||||
| SSRI | 258 (25.7) | 138 (22.8) | 120 (30.1) | 0.244 |
| TCA | 93 (9.3) | 44 (7.3) | 49 (12.3) | |
| SNRI | 63 (6.3) | 33 (5.5) | 30 (7.5) | |
| Other antidepressants | 97 (9.7) | 60 (9.9) | 37 (9.3) | |
| Lithium, N (%) | 270 (28.7) | 163 (28.6) | 107 (28.7) | 0.990 |
| Other mood stabilizers, N (%) | 317 (31.6) | 185 (30.6) | 132 (33.1) | 0.403 |
| Antipsychotics, N (%) | 404 (40.2) | 249 (41.2) | 155 (38.8) | 0.465 |
| Switch (+) | Switch (−) | Odds Ratio (95% CI) | p Value | |
|---|---|---|---|---|
| GWAS cohort, N = 746(%) | ||||
| CC | 301 (85.3%) | 275 (70.0%) | 2.5 (1.7–3.6) | 6.6 × 10−7 |
| TT + TC | 52 (14.7%) | 118 (30.0%) | ||
| Replication cohort, N = 255(%) | ||||
| CC | 77 (72.6%) | 100 (67.1%) | 1.3 (0.8–2.2) | 0.36 |
| TT + TC | 29 (27.4%) | 49 (32.9%) | ||
| Combined, N = 1001(%) | ||||
| CC | 378 (82.4%) | 375 (69.2%) | 2.1 (1.5–2.8) | 1.96 × 10−6 |
| TT + TC | 81 (17.6%) | 167(30.8%) | ||
| Antidepressants X rs10262219 * | ||||
| Antidepressants(−) × CT + TT (ref.) | 1 | |||
| Antidepressants(+) × CC | 5.9 (3.7–9.4) | <10−6 | ||
| Antidepressants(+) × CT + TT | 2.3 (1.4–3.7) | 7.0 × 10−4 | ||
| Antidepressants(−) × CC | 3.0 (1.7–5.2) | 1.2 × 10−4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-K.; Wu, L.S.-H.; Huang, M.-C.; Kuo, C.-J.; Cheng, A.T.-A. Antidepressant Treatment and Manic Switch in Bipolar I Disorder: A Clinical and Molecular Genetic Study. J. Pers. Med. 2022, 12, 615. https://doi.org/10.3390/jpm12040615
Chen C-K, Wu LS-H, Huang M-C, Kuo C-J, Cheng AT-A. Antidepressant Treatment and Manic Switch in Bipolar I Disorder: A Clinical and Molecular Genetic Study. Journal of Personalized Medicine. 2022; 12(4):615. https://doi.org/10.3390/jpm12040615
Chicago/Turabian StyleChen, Chih-Ken, Lawrence Shih-Hsin Wu, Ming-Chyi Huang, Chian-Jue Kuo, and Andrew Tai-Ann Cheng. 2022. "Antidepressant Treatment and Manic Switch in Bipolar I Disorder: A Clinical and Molecular Genetic Study" Journal of Personalized Medicine 12, no. 4: 615. https://doi.org/10.3390/jpm12040615
APA StyleChen, C. -K., Wu, L. S. -H., Huang, M. -C., Kuo, C. -J., & Cheng, A. T. -A. (2022). Antidepressant Treatment and Manic Switch in Bipolar I Disorder: A Clinical and Molecular Genetic Study. Journal of Personalized Medicine, 12(4), 615. https://doi.org/10.3390/jpm12040615