
Dental Biofilm and Saliva Microbiome and Its Interplay with Pediatric Allergies

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dental Examination and Sampling Procedures
- Saliva sampling, salivary flow rate, and other dental parameters
- 2.
- Dental biofilm sampling
2.3. Microbiome Analysis of Saliva and Dental Biofilm
- DNA isolation and sequencing
- 16s rRNA gene data collection and sequencing
- Microbiome sequencing analysis
3. Results
3.1. Demographic Information and Dental Parameter
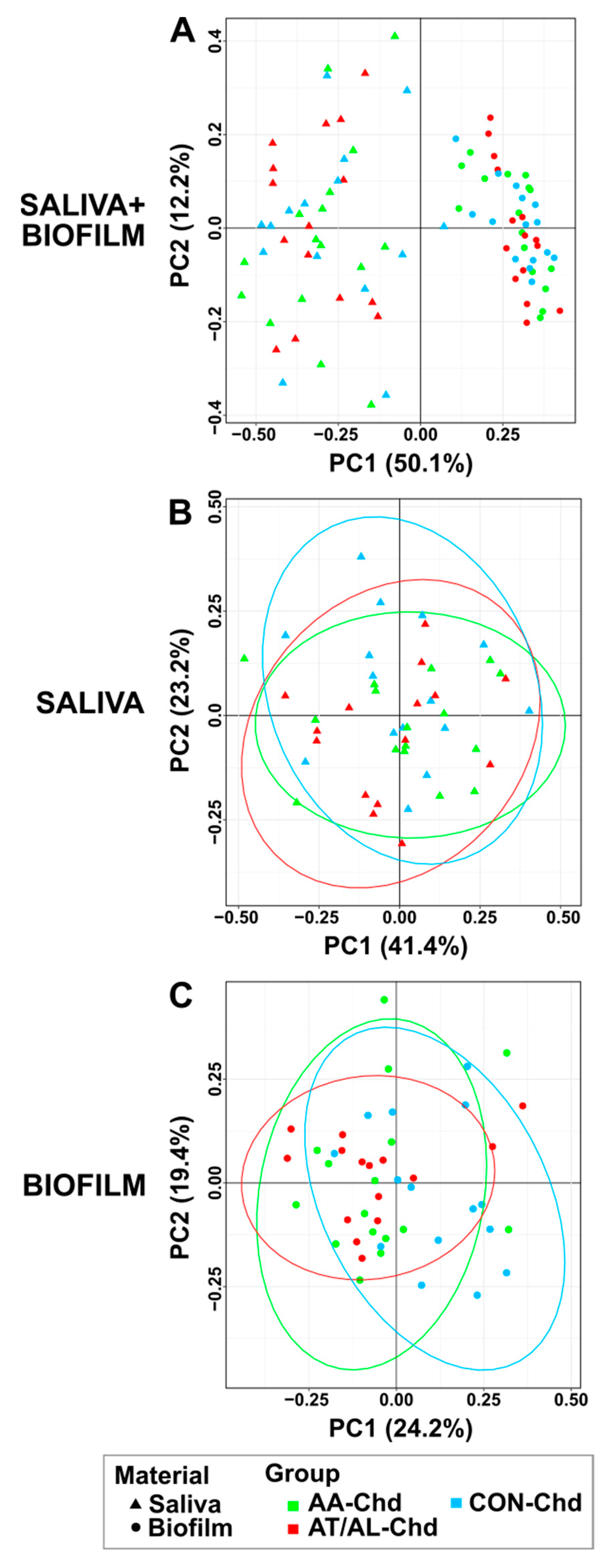
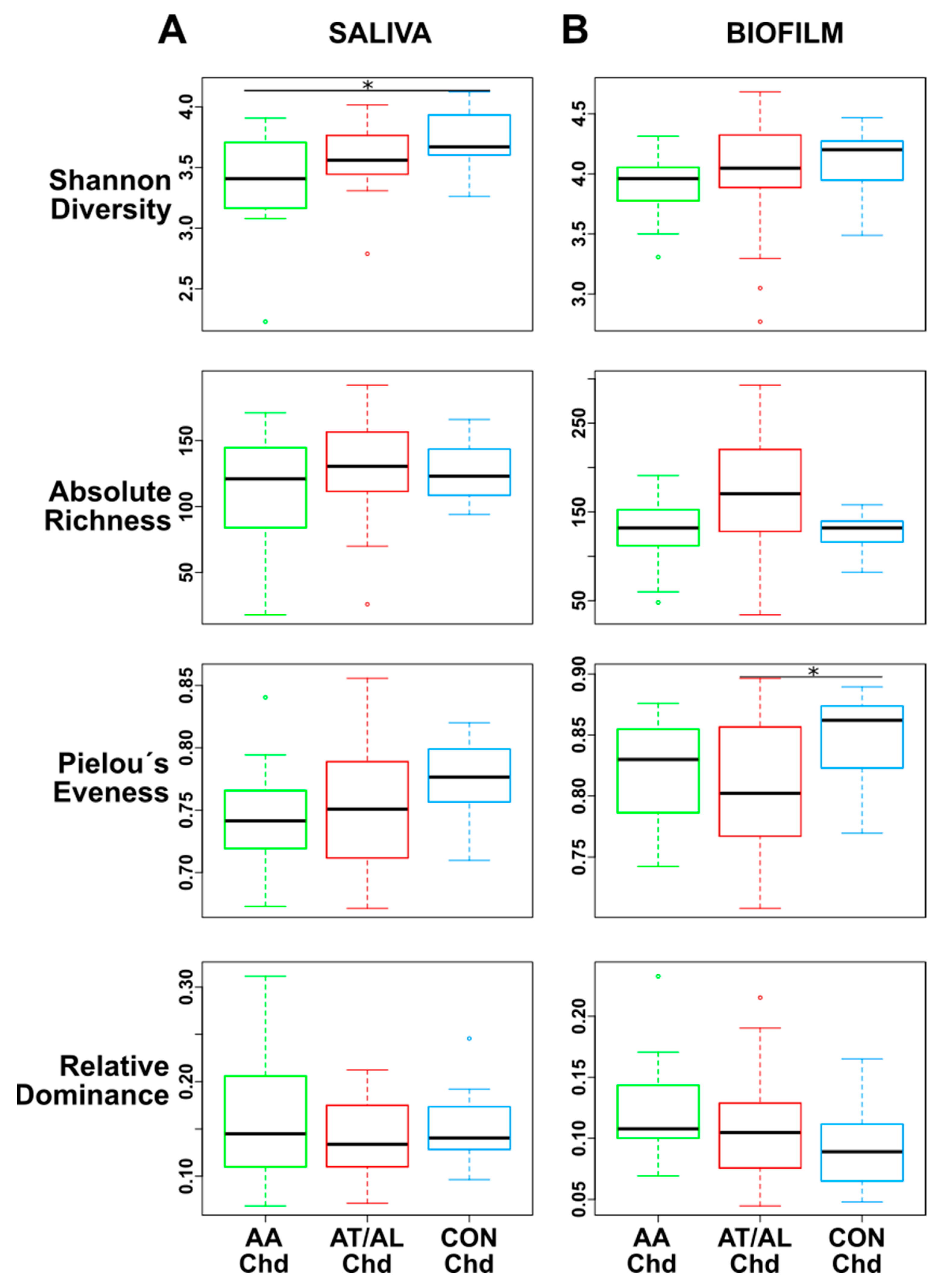
3.2. Comparison of Saliva and Biofilm
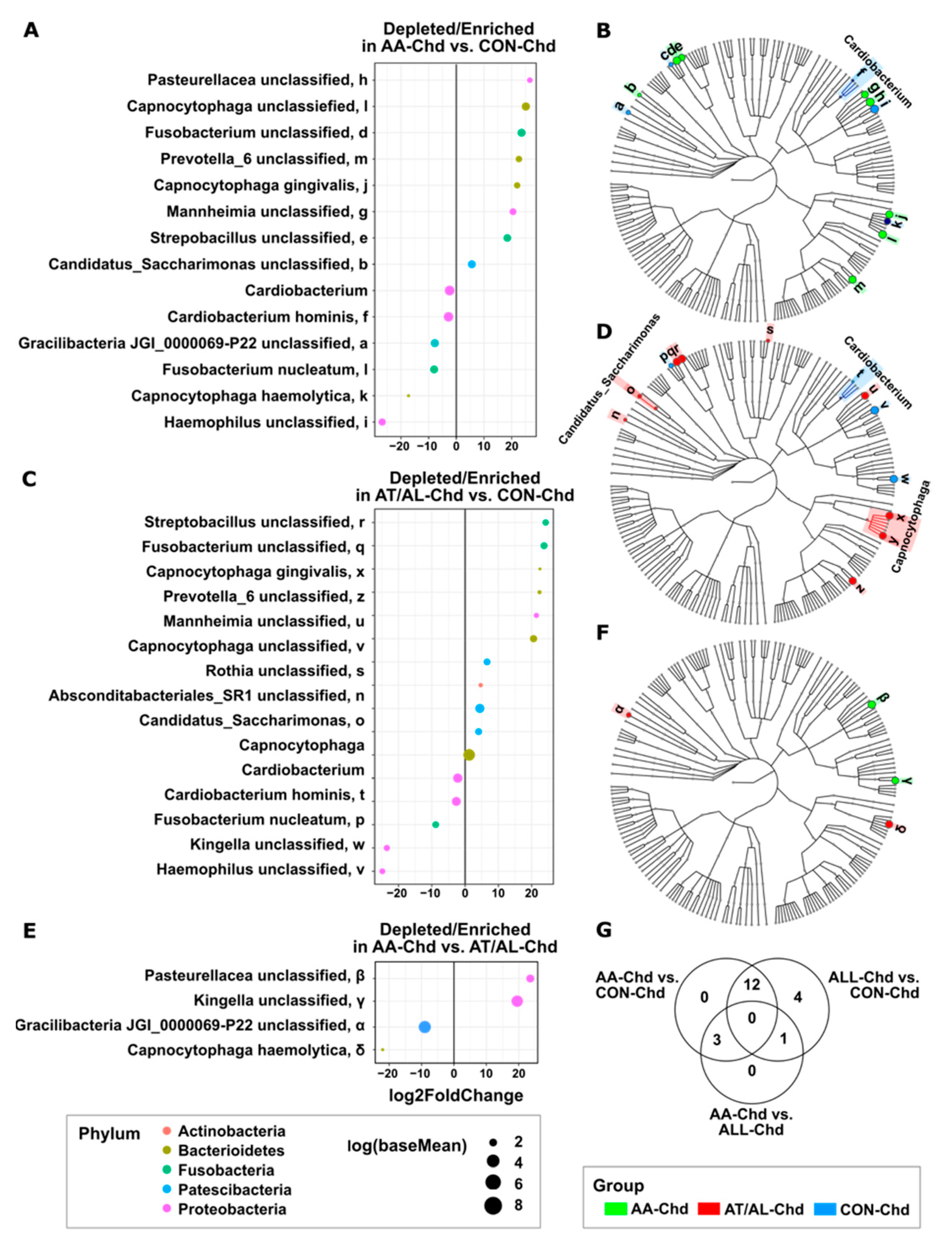
3.3. Enriched or Depleted Taxa of Dental Biofilm
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wade, W.G. Detection and culture of novel oral Bacteria. In Oral Microbial Ecology—Current Research and New Perspectives; Jakubovics, N.S., Palmer, R.J., Jr., Eds.; Caister Academic Press: Norfolk, UK, 2013. [Google Scholar]
- Kumar, P.S.; Mason, M.R.; Yu, J. Biofilms in Periodontal Health and Disease. In Oral Microbial Ecology—Current Research and New Perspectives; Jakubovics, N.S., Palmer, R.J., Jr., Eds.; Caister Academic Press: Norfolk, UK, 2013. [Google Scholar]
- Costerton, J.W.; Lewandowski, Z.; Caldwell, D.E.; Korber, D.R.; Lappin-Scott, H.M. Microbial biofilms. Ann. Rev. Microbiol. 1995, 49, 711–745. [Google Scholar] [CrossRef]
- Marsh, P.D. Microbial succession in relation to enamel demineralisation. Microb. Ecol. Health Dis. 1990. [Google Scholar] [CrossRef]
- Arweiler, N.B.; Netuschil, L. The oral microbiota. Adv. Exp. Med. Biol. 2016, 902, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Morhart, R.; Fitzgerald, R. Composition and ecology of the oral flora. In The Biologic Basis of Dental Caries; Menaker, L., Ed.; Harper & Row: Hagerstown, MD, USA, 1980; pp. 263–277. [Google Scholar]
- Al-Ahmad, A.; Wunder, A.; Auschill, T.M.; Follo, M.; Braun, G.; Hellwig, E.; Arweiler, N.B. The in vivo dynamics of Streptococcus spp., Actinomyces naeslundii, Fusobacterium nucleatum and Veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. J. Med. Microbiol. 2007, 56, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D.; Martin, M.V.; Lewis, M.A.O.; Williams, D.W. Oral Microbiology, 5th ed.; Churchill Livingstone Elsevier: Edinburgh, UK, 2009. [Google Scholar]
- Arweiler, N.B.; Hellwig, E.; Sculean, A.; Hein, N.; Auschill, T.M. Individual vitality pattern of in situ dental biofilms at different locations in the oral cavity. Caries Res. 2004, 38, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Arweiler, N.B.; Lenz, R.; Sculean, A.; Al-Ahmad, A.; Hellwig, E.; Auschill, T.M. Effect of food preservatives on in situ biofilm formation. Clin. Oral Investig. 2008, 12, 203–208. [Google Scholar] [CrossRef]
- Arweiler, N.B.; Netuschil, L.; Beier, D.; Grunert, S.; Heumann, C.; Altenburger, M.J.; Sculean, A.; Nagy, K.; Al-Ahmad, A.; Auschill, T.M. Action of food preservatives on 14-days dental biofilm formation, biofilm vitality and biofilm-derived enamel demineralisation in situ. Clin. Oral Investig. 2014, 18, 829–838. [Google Scholar] [CrossRef]
- Arweiler, N.B.; Auschill, T.M.; Heumann, C.; Hellwig, E.; Al-Ahmad, A. Influence of probiotics on the salivary microflora oral Streptococci and their integration into oral biofilm. Antibiotics 2020, 9, 803. [Google Scholar] [CrossRef]
- Auschill, T.M.; Arweiler, N.B.; Netuschil, L.; Brecx, M.; Reich, E.; Sculean, A. Spatial distribution of vital and dead microorganisms in dental biofilms. Arch. Oral Biol. 2001, 46, 471–4766. [Google Scholar] [CrossRef]
- Auschill, T.M.; Arweiler, N.B.; Brecx, M.; Reich, E.; Sculean, A.; Netuschil, L. The effect of dental restorative materials on dental biofilm. Eur. J. Oral Sci. 2002, 110, 48–53. [Google Scholar] [CrossRef]
- Willis, J.R.; Gabaldón, T. The human oral microbiome in health and disease: From sequences to ecosystems. Microorganisms 2020, 8, 308. [Google Scholar] [CrossRef] [Green Version]
- Khumaedi, A.I.; Purnamasari, D.; Wijaya, I.P.; Soeroso, Y. The relationship of diabetes, periodontitis and cardiovascular disease. Diabetes Metab. Syndr. 2019, 13, 1675–1678. [Google Scholar] [CrossRef]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Graziani, F.; Loos, B.; Pertel, P.; Wimmer, G.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Sapey, E.; Yonel, Z.; Edgar, R.; Parmar, S.; Hobbins, S.; Newby, P.; Crossley, D.; Usher, A.; Johnson, S.; Walton, G.M.; et al. The clinical and inflammatory relationships between periodontitis and chronic obstructive pulmonary disease. J. Clin. Periodontol. 2020, 47, 1040–1052. [Google Scholar] [CrossRef]
- Minty, M.; Canceil, T.; Serino, M.; Burcelin, R.; Tercé, F.; Blasco-Baque, V. Oral microbiota-induced periodontitis: A new risk factor of metabolic diseases. Rev. Endocr. Metab. Disord. 2019, 20, 449–459. [Google Scholar] [CrossRef]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontology 2000, 83, 125–153. [Google Scholar] [CrossRef] [PubMed]
- McDerra, E.J.; Pollard, M.A.; Curzon, M.E. The dental status of asthmatic British school children. Pediatr. Dent. 1998, 20, 281–287. [Google Scholar]
- Milano, M.; Lee, J.Y.; Donovan, K.; Chen, J.-W. A cross-sectional study of medication-related factors and caries experience in asthmatic children. Pediatric Dent. 2006, 28, 415–419. [Google Scholar]
- Stensson, M.; Wendt, L.-K.; Koch, G.; Oldaeus, G.; Birkhed, D. Oral health in preschool children with asthma. Int. J. Paediatr. Dent. 2008, 18, 243–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, J.D.; Taylor, S.E.; Nunn, M.E. The association between asthma and dental caries in children and adolescents: A population-based case-control study. Caries Res. 2001, 35, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, N.; Kocher, T.; Wallaschofski, H.; Schwahn, C.; Lüdemann, J.; Kerner, W.; Völzke, H. Inverse association between periodontitis and respiratory allergies in patients with type 1 diabetes mellitus. J. Clin. Periodontol. 2008, 35, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Arbes, S.J., Jr.; Matsui, E.C. Can oral pathogens influence allergic disease? J. Allergy Clin. Immunol. 2011, 127, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Hesselmar, B.; Sjöberg, F.; Saalman, R.; Aberg, N.; Adlerberth, I.; Wold, A.E. Pacifier cleaning practices and risk of allergy development. Pediatrics 2013, 131, e1829–e1837. [Google Scholar] [CrossRef] [Green Version]
- Reddy, B.V.; Chava, V.K.; Nagarakanti, S.; Gunupati, S.; Samudrala, P. Hygiene hypothesis and periodontitis—A possible association. Med. Hypotheses 2014, 82, 60–63. [Google Scholar] [CrossRef]
- Caporaso, J.G.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Huntley, J.; Fierer, N.; Owens, S.M.; Betley, J.; Fraser, L.; Bauer, M.; et al. Ultra-high-throughput microbial community analysis on the Illumina HiSeq and MiSeq platforms. ISME J. 2012, 6, 621–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoilew, K.; Ueffing, H.; Dalpke, A.; Wolff, B.; Frese, C.; Wolff, D.; Boutin, S. Bacterial biofilm composition in healthy subjects with and without caries experience. J. Oral Microbiol. 2019, 11, 1633194. [Google Scholar] [CrossRef] [Green Version]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The human respiratory system and its microbiome at a glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef]
- Johnson, C.C.; Ownby, D.R.; Alford, S.H.; Havstad, S.L.; Williams, L.K.; Zoratti, E.M.; Peterson, E.L.; Joseph, C.L. Antibiotic exposure in early infancy and risk for childhood atopy. J. Allergy Clin. Immunol. 2005, 115, 1218–1224. [Google Scholar] [CrossRef]
- Jakobsson, H.E.; Abrahamsson, T.R.; Jenmalm, M.C.; Harris, K.; Quince, C.; Jernberg, C.; Björkstén, B.; Engstrand, L.; Andersson, A.F. Decreased gut microbiota diversity, delayed Bacteroidetes colonisation and reduced Th1 responses in infants delivered by caesarean section. Gut 2014, 63, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Guaraldi, F.; Salvatori, G. Effect of breast and formula feeding on gut microbiota shaping in newborns. Front. Cell Infect. Microbiol. 2012, 2, 94. [Google Scholar] [CrossRef] [Green Version]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Jenmalm, M.C. The mother-offspring dyad: Microbial transmission, immune interactions and allergy development. J. Intern. Med. 2017, 282, 484–495. [Google Scholar] [CrossRef] [Green Version]
- West, C.E.; Dzidic, M.; Prescott, S.L.; Jenmalm, M.C. Bugging allergy; role of pre-, pro- and synbiotics in allergy prevention. Allergol. Int. 2017, 66, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Kemter, A.M.; Nagler, C.R. Influences on allergic mechanisms through gut, lung, and skin microbiome exposures. J. Clin. Investig. 2019, 129, 1483–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzidic, M.; Abrahamsson, T.R.; Artacho, A.; Collado, M.C.; Mira, A.; Jenmalm, M.C. Oral microbiota maturation during the first 7 years of life in relation to allergy development. Allergy. 2018, 73, 2000–2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, H.E.; Chun, Y.; Jeong, S.; Jumreornvong, O.; Sicherer, S.H.; Bunyavanich, S. Multidimensional study of the oral microbiome, metabolite, and immunologic environment in peanut allergy. J. Allergy Clin. Immunol. 2021. [Google Scholar] [CrossRef]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.D.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral microbiota and immune system crosstalk: A translational research. Biology 2020, 9, 131. [Google Scholar] [CrossRef]
- Busscher, H.J.; van der Mei, H.C. Physico-chemical interactions in initial microbial adhesion and relevance for biofilm formation. Adv. Dent. Res. 1997, 11, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Cook, G.; Lamont, R. The community architecture of biofilms: Dynamic structures and mechanisms. In Dental Plaque Revisited; Newman, H.N., Wilson, M., Eds.; BioLine, Antony Rowe Ltd.: Chippenham, UK, 1999; pp. 5–14. [Google Scholar]
- Zaura, E.; Keijser, B.J.; Huse, S.M.; Crielaard, W. Defining the healthy “core microbiome” of oral microbial communities. BMC Microbiol. 2009, 9, 259. [Google Scholar] [CrossRef] [Green Version]
- Watnick, P.; Kolter, R. Biofilm, city of microbes. J. Bacteriol. 2000, 182, 2675–2679. [Google Scholar] [CrossRef] [Green Version]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Anwar, H.; Strap, J.L.; Costerton, J.W. Establishment of aging biofilms: Possible mechanism of bacterial resistance to antimicrobial therapy. Antimicrob. Agents Chemother. 1992, 36, 1347–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renz, H.; Skevaki, C. Early life microbial exposures and allergy risks: Opportunities for prevention. Nat. Rev. Immunol. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | AA-Chd | AT/AL-Chd | CON-Chd |
|---|---|---|---|
| Group size | n = 15 | n = 16 | n = 15 |
| Age (years) | 10.73 ± 2.89 | 11.31 ± 2.82 | 9.93 ± 2.22 |
| Sex (male:female) | 8:7 | 8:8 | 9:6 |
| BMI (kg/m2 mean) | 18.79 ± 2.44 | 19.49 ± 5.63 | 17.66 ± 4.07 |
| SFR (mL/min) | 0.33 ± 0.18 | 0.53 ± 0.25 | 0.28 ± 0.16 |
| Dmft/DMFT | 0.47 ± 1.30 | 1.00 ± 2.00 | 1.27 ± 1.91 |
| PSI | 0.73 ± 0.45 | 0.41 ± 0.39 a | 1.07 ± 0.38 a |
| GBI (%) | 16.00 ± 13.00 a,b | 8.00 ± 9.00 a,b | 36.00 ± 12.00 a |
| PCR (%) | 68.00 ± 27.00 | 65.00 ± 27.00 | 51.00 ± 11.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arweiler, N.B.; Rahmel, V.; Alhamwe, B.A.; Alhamdan, F.; Zemlin, M.; Boutin, S.; Dalpke, A.; Renz, H. Dental Biofilm and Saliva Microbiome and Its Interplay with Pediatric Allergies. Microorganisms 2021, 9, 1330. https://doi.org/10.3390/microorganisms9061330
Arweiler NB, Rahmel V, Alhamwe BA, Alhamdan F, Zemlin M, Boutin S, Dalpke A, Renz H. Dental Biofilm and Saliva Microbiome and Its Interplay with Pediatric Allergies. Microorganisms. 2021; 9(6):1330. https://doi.org/10.3390/microorganisms9061330
Chicago/Turabian StyleArweiler, Nicole B., Vivien Rahmel, Bilal Alashkar Alhamwe, Fahd Alhamdan, Michael Zemlin, Sébastien Boutin, Alexander Dalpke, and Harald Renz. 2021. "Dental Biofilm and Saliva Microbiome and Its Interplay with Pediatric Allergies" Microorganisms 9, no. 6: 1330. https://doi.org/10.3390/microorganisms9061330
APA StyleArweiler, N. B., Rahmel, V., Alhamwe, B. A., Alhamdan, F., Zemlin, M., Boutin, S., Dalpke, A., & Renz, H. (2021). Dental Biofilm and Saliva Microbiome and Its Interplay with Pediatric Allergies. Microorganisms, 9(6), 1330. https://doi.org/10.3390/microorganisms9061330