
Mild Coronavirus Disease 2019 (COVID-19) Is Marked by Systemic Oxidative Stress: A Pilot Study

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Measurement of Free Thiols
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
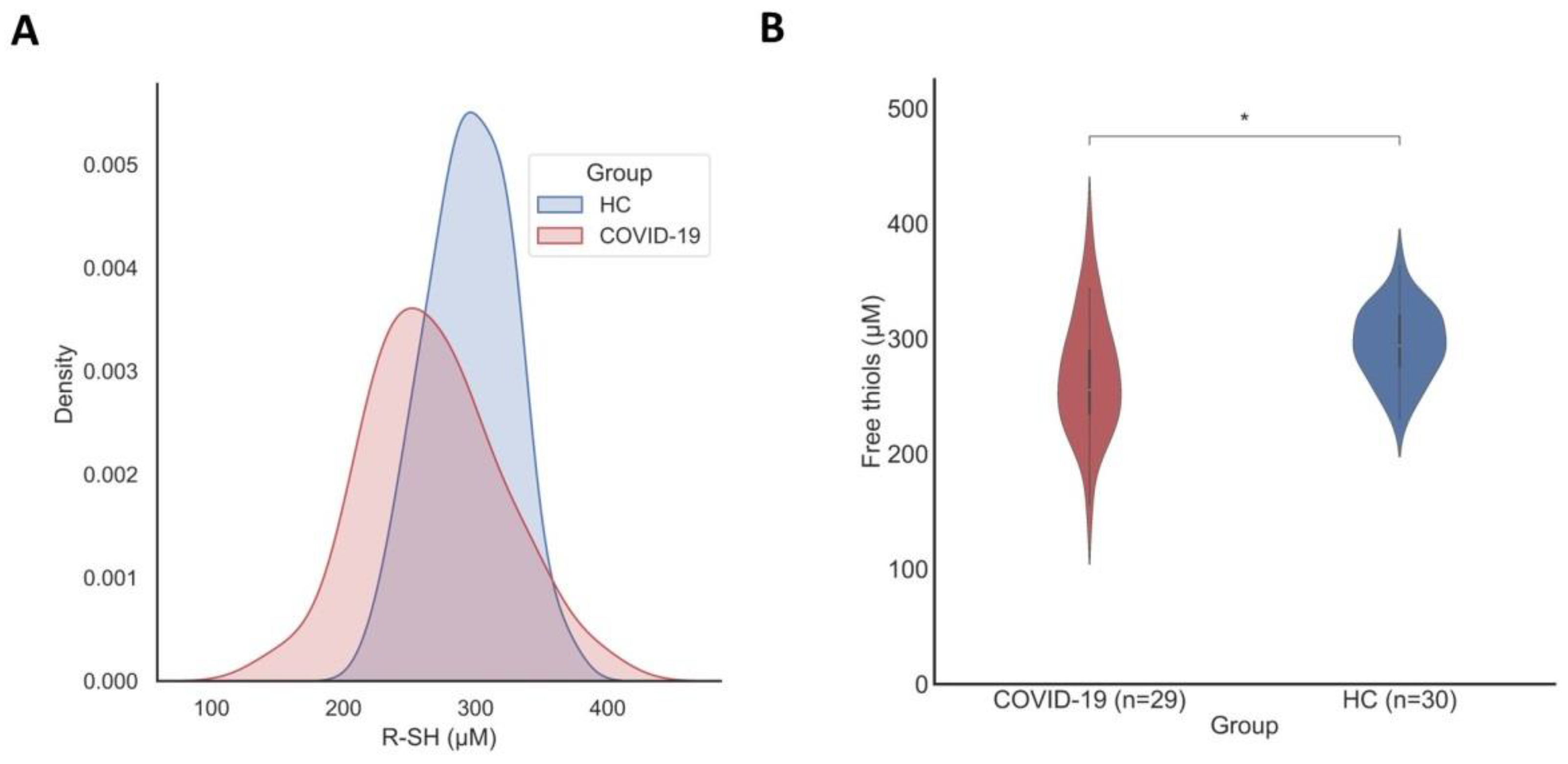
3.2. Serum Free Thiol Concentrations Are Significantly Reduced in Patients with COVID-19
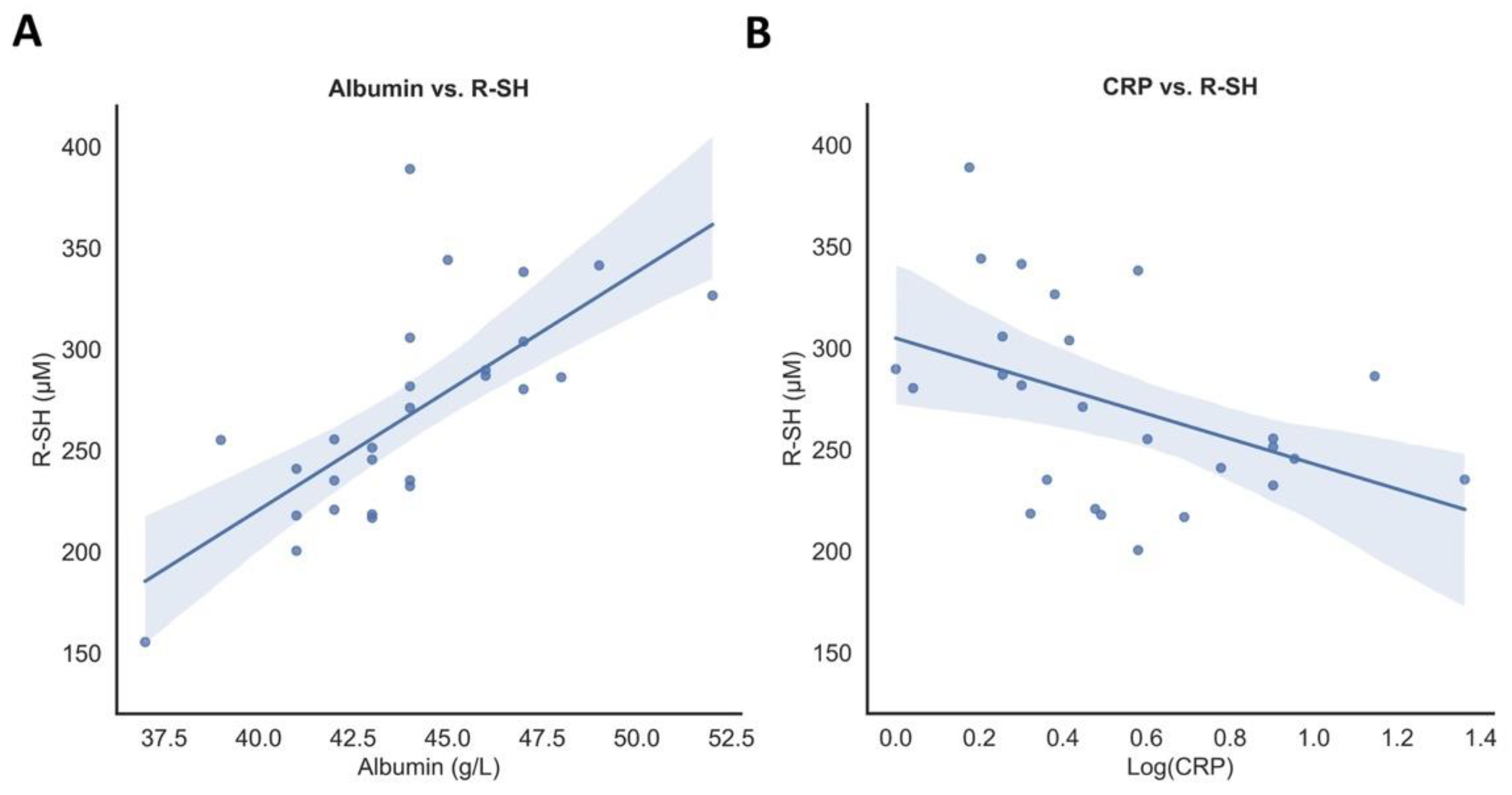
3.3. Associations of Serum Free Thiol Concentrations with Disease Parameters
3.4. Serum Free Thiol Concentrations Associate with COVID-19 Disease Severity
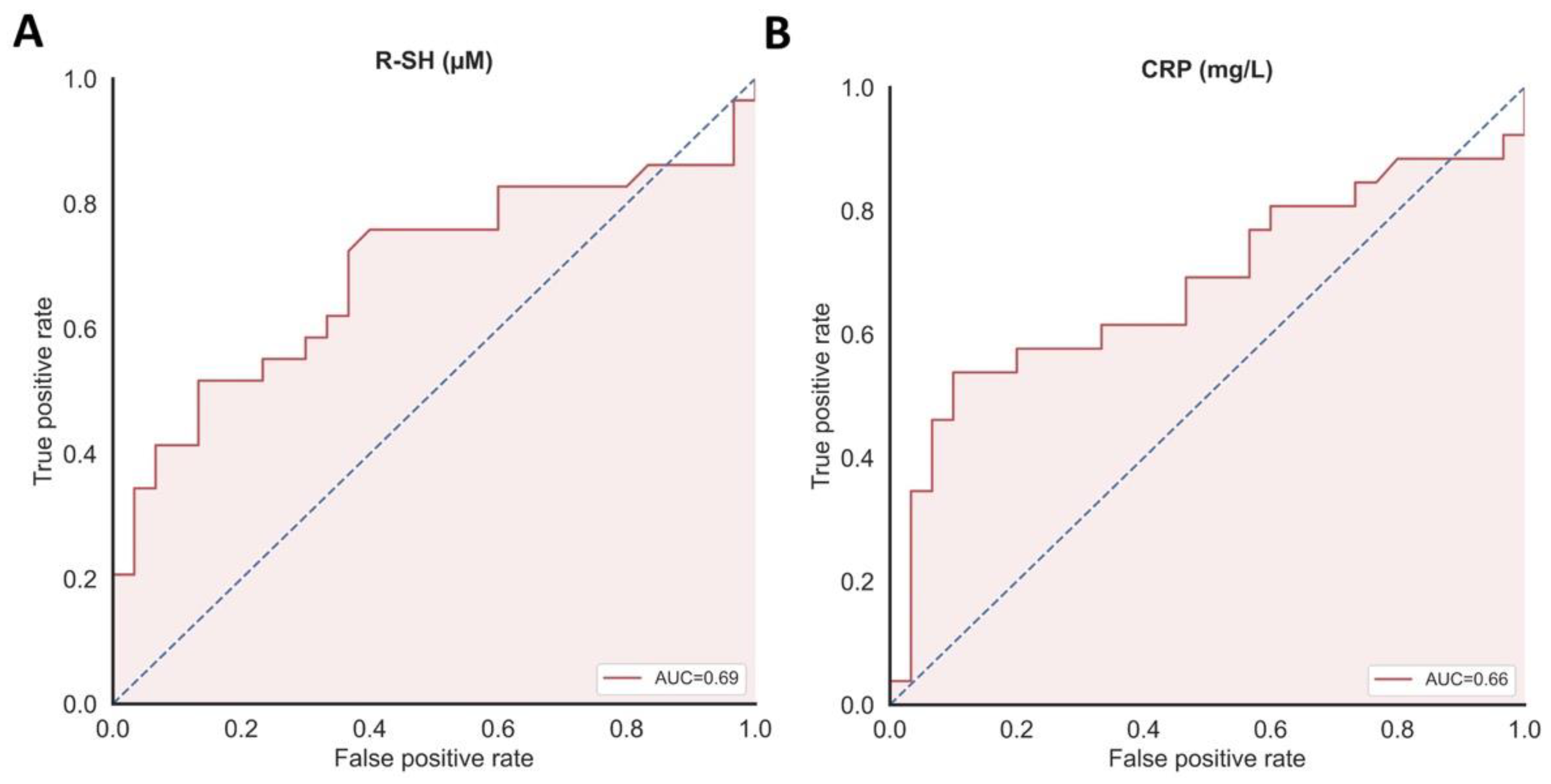
3.5. Discriminative Capacity of Serum Free Thiols as Biomarker for COVID-19 Disease Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Eijk, L.E.; Binkhorst, M.; Bourgonje, A.R.; Offringa, A.K.; Mulder, D.J.; Bos, E.M.; Kolundzic, N.; Abdulle, A.E.; van der Voort, P.H.; Rikkert, M.G.O.; et al. COVID-19: Immunopathology, pathophysiological mechanisms, and treatment options. J. Pathol. 2021, 254, 307–331. [Google Scholar] [CrossRef]
- Bourgonje, A.R.; Abdulle, A.E.; Timens, W.; Hillebrands, J.L.; Navis, G.J.; Gordijn, S.J.; Bolling, M.C.; Dijkstra, G.; Voors, A.A.; Osterhaus, A.D.; et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J. Pathol. 2020, 251, 228–248. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Sies, H.; Jones, D.P. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef] [PubMed]
- Cumpstey, A.F.; Clark, A.D.; Santolini, J.; Jackson, A.A.; Feelisch, M. COVID-19: A Redox Disease-What a Stress Pandemic Can Teach Us About Resilience and What We May Learn from the Reactive Species Interactome About Its Treatment. Antioxid. Redox Signal. 2021, 35, 1226–1268. [Google Scholar] [CrossRef]
- Bourgonje, A.R.; Offringa, A.K.; van Eijk, L.E.; Abdulle, A.E.; Hillebrands, J.L.; van der Voort, P.H.J.; van Goor, H.; van Hezik, E.J. N-Acetylcysteine and Hydrogen Sulfide in Coronavirus Disease 2019. Antioxid. Redox Signal. 2021, 35, 1207–1225. [Google Scholar] [CrossRef] [PubMed]
- Dagcioglu, B.F.; Keskin, A.; Guner, R.; Kaya Kalem, A.; Eser, F.; Erel, O.; Neselioglu, S.; Bayrakdar, F.; Ozkara, A. Thiol levels in mild or moderate COVID-19 patients: A comparison of variant and classic COVID-19 cases. Int. J. Clin. Pract. 2021, 75, e14753. [Google Scholar] [CrossRef]
- Kalem, A.K.; Kayaaslan, B.; Neselioglu, S.; Eser, F.; Hasanoglu, İ.; Aypak, A.; Akinci, E.; Akca, H.N.; Erel, O.; Guner, R. A useful and sensitive marker in the prediction of COVID-19 and disease severity: Thiol. Free Radic. Biol. Med. 2021, 166, 11–17. [Google Scholar] [CrossRef]
- Abdulle, A.E.; Bourgonje, A.R.; Kieneker, L.M.; Koning, A.M.; la Bastide-van Gemert, S.; Bulthuis, M.L.C.; Dijkstra, G.; Faber, K.N.; Dullaart, R.P.F.; Bakker, S.J.L.; et al. Serum free thiols predict cardiovascular events and all-cause mortality in the general population: A prospective cohort study. BMC Med. 2020, 18, 130. [Google Scholar] [CrossRef]
- Frenay, A.S.; de Borst, M.H.; Bachtler, M.; Tschopp, N.; Keyzer, C.A.; van den Berg, E.; Bakker, S.J.; Feelisch, M.; Pasch, A.; van Goor, H. Serum free sulfhydryl status is associated with patient and graft survival in renal transplant recipients. Free Radic. Biol. Med. 2016, 99, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Bourgonje, A.R.; Abdulle, A.E.; Al-Rawas, A.M.; Al-Maqbali, M.; Al-Saleh, M.; Enriquez, M.B.; Al-Siyabi, S.; Al-Hashmi, K.; Al-Lawati, I.; Bulthuis, M.L.C.; et al. Systemic Oxidative Stress Is Increased in Postmenopausal Women and Independently Associates with Homocysteine Levels. Int. J. Mol. Sci. 2020, 21, 314. [Google Scholar] [CrossRef] [Green Version]
- Cortese-Krott, M.M.; Koning, A.; Kuhnle, G.G.C.; Nagy, P.; Bianco, C.L.; Pasch, A.; Wink, D.A.; Fukuto, J.M.; Jackson, A.A.; Van Goor, H.; et al. The Reactive Species Interactome: Evolutionary Emergence, Biological Significance, and Opportunities for Redox Metabolomics and Personalized Medicine. Antioxid. Redox Signal. 2017, 27, 684–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banne, A.F.; Amiri, A.; Pero, R.W. Reduced level of serum thiols in patients with a diagnosis of active disease. J. Anti Aging Med. 2003, 6, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Koning, A.M.; Meijers, W.C.; Pasch, A.; Leuvenink, H.G.D.; Frenay, A.S.; Dekker, M.M.; Feelisch, M.; de Boer, R.A.; van Goor, H. Serum free thiols in chronic heart failure. Pharmacol. Res. 2016, 111, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef]
- Tami, A.; van der Gun, B.T.F.; Wold, K.; Vincenti-Gonzalez, M.F.; Knoester, M.; Dijkstra, A.; Veloo, A.C.M.; van den Boogaard, J.; Huckriede, A.; Niesters, H.G.M.; et al. The COVID-HOME Study: Prospective Cohort Study Of Non-hospitalised COVID-19 Patients. In Proceedings of the Part II: Patient Clinical Development at Home, Proceedings of the ESCMID Conference on Coronavirus Disease, Online Conference, 23–25 September 2020; p. 00283. [Google Scholar]
- Hu, M.L.; Louie, S.; Cross, C.E.; Motchnik, P.; Halliwell, B. Antioxidant protection against hypochlorous acid in human plasma. J. Lab. Clin. Med. 1993, 121, 257–262. [Google Scholar] [PubMed]
- Ellman, G.L. Tissue sulfhydryl groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Giustarini, D.; Dalle-Donne, I.; Lorenzini, S.; Milzani, A.; Rossi, R. Age-related influence on thiol, disulfide, and protein-mixed disulfide levels in human plasma. J. Gerontol. A Biol. Sci Med. Sci. 2006, 61, 1030–1038. [Google Scholar] [CrossRef] [Green Version]
- van der Voort, P.H.J.; Moser, J.; Zandstra, D.F.; Muller Kobold, A.C.; Knoester, M.; Calkhoven, C.F.; Hamming, I.; van Meurs, M. Leptin levels in SARS-CoV-2 infection related respiratory failure: A cross-sectional study and a pathophysiological framework on the role of fat tissue. Heliyon 2020, 6, e04696. [Google Scholar] [CrossRef]
- Anraku, M.; Chuang, V.T.; Maruyama, T.; Otagiri, M. Redox properties of serum albumin. Biochim. Biophys. Acta 2013, 1830, 5465–5472. [Google Scholar] [CrossRef] [PubMed]
- Hortin, G.L.; Sviridov, D.; Anderson, N.L. High-abundance polypeptides of the human plasma proteome comprising the top 4 logs of polypeptide abundance. Clin. Chem. 2008, 54, 1608–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgonje, M.F.; Bourgonje, A.R.; Abdulle, A.E.; Kieneker, L.M.; la Bastide-van Gemert, S.; Gansevoort, R.T.; Bakker, S.J.L.; Mulder, D.J.; Pasch, A.; Saleh, J.; et al. Systemic Oxidative Stress, Aging and the Risk of Cardiovascular Events in the General Female Population. Front. Cardiovasc. Med. 2021, 8, 630543. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.A.; Fossali, T.; Pandolfi, L.; Carsana, L.; Ottolina, D.; Frangipane, V.; Rech, R.; Tosoni, A.; Lopez, G.; Agarossi, A.; et al. Hypoalbuminemia in COVID-19: Assessing the hypothesis for underlying pulmonary capillary leakage. J. Intern. Med. 2021, 289, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Danielski, M.; Ikizler, T.A.; McMonagle, E.; Kane, J.C.; Pupim, L.; Morrow, J.; Himmelfarb, J. Linkage of hypoalbuminemia, inflammation, and oxidative stress in patients receiving maintenance hemodialysis therapy. Am. J. Kidney Dis. 2003, 42, 286–294. [Google Scholar] [CrossRef]
- Damba, T.; Bourgonje, A.R.; Abdulle, A.E.; Pasch, A.; Sydor, S.; van den Berg, E.H.; Gansevoort, R.T.; Bakker, S.J.L.; Blokzijl, H.; Dullaart, R.P.F.; et al. Oxidative stress is associated with suspected non-alcoholic fatty liver disease and all-cause mortality in the general population. Liver Int. 2020, 40, 2148–2159. [Google Scholar] [CrossRef]
- Sutton, T.R.; Minnion, M.; Barbarino, F.; Koster, G.; Fernandez, B.O.; Cumpstey, A.F.; Wischmann, P.; Madhani, M.; Frenneaux, M.P.; Postle, A.D.; et al. A robust and versatile mass spectrometry platform for comprehensive assessment of the thiol redox metabolome. Redox Biol. 2018, 16, 359–380. [Google Scholar] [CrossRef]
- Deneke, S.M. Thiol-based antioxidants. Curr. Top. Cell. Regul. 2000, 36, 151–180. [Google Scholar]
- Renieris, G.; Katrini, K.; Damoulari, C.; Akinosoglou, K.; Psarrakis, C.; Kyriakopoulou, M.; Dimopoulos, G.; Lada, M.; Koufargyris, P.; Giamarellos-Bourboulis, E.J. Serum Hydrogen Sulfide and Outcome Association in Pneumonia by the SARS-CoV-2 Coronavirus. Shock 2020, 54, 633–637. [Google Scholar] [CrossRef]
- Assimakopoulos, S.F.; Aretha, D.; Komninos, D.; Dimitropoulou, D.; Lagadinou, M.; Leonidou, L.; Oikonomou, I.; Mouzaki, A.; Marangos, M. N-acetyl-cysteine reduces the risk for mechanical ventilation and mortality in patients with COVID-19 pneumonia: A two-center retrospective cohort study. Infect. Dis. (Lond) 2021, 53, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Iwegbulem, O.; Wang, J.; Pfirrmann, R.W.; Redmond, H.P. The role of taurine derivatives in the putative therapy of COVID-19-induced inflammation. Ir. J. Med. Sci. 2021, 1–2. [Google Scholar] [CrossRef]
- Olas, B.; Nowak, P.; Wachowicz, B. Resveratrol protects against peroxynitrite-induced thiol oxidation in blood platelets. Cell. Mol. Biol. Lett. 2004, 9, 577–587. [Google Scholar] [PubMed]
- Guo, J.Z.; Li, Y.L.; Zhong, L.M.; Bian, L.G.; Ai, Q.L.; Wang, W.M.; Lu, D. Resveratrol regulates endogenous thiol antioxidants of the hippocampal in status epilepticus rat model. Acta Anat. Sin. 2011, 42, 582–587. [Google Scholar]
- Seyyedebrahimi, S.; Khodabandehloo, H.; Nasli Esfahani, E.; Meshkani, R. The effects of resveratrol on markers of oxidative stress in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled clinical trial. Acta. Diabetol. 2018, 55, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Ter Ellen, B.M.; Dinesh Kumar, N.; Bouma, E.M.; Troost, B.; van de Pol, D.P.I.; van der Ende-Metselaar, H.H.; Apperloo, L.; van Gosliga, D.; van den Berge, M.; Nawijn, M.C.; et al. Resveratrol and Pterostilbene Inhibit SARS-CoV-2 Replication in Air-Liquid Interface Cultured Human Primary Bronchial Epithelial Cells. Viruses 2021, 13, 1335. [Google Scholar] [CrossRef]
- Di Pierro, F.; Iqtadar, S.; Khan, A.; Ullah Mumtaz, S.; Masud Chaudhry, M.; Bertuccioli, A.; Derosa, G.; Maffioli, P.; Togni, S.; Riva, A.; et al. Potential Clinical Benefits of Quercetin in the Early Stage of COVID-19: Results of a Second, Pilot, Randomized, Controlled and Open-Label Clinical Trial. Int. J. Gen. Med. 2021, 14, 2807–2816. [Google Scholar] [CrossRef]
- Farnoosh, G.; Akbariqomi, M.; Badri, T.; Bagheri, M.; Izadi, M.; Saeedi-Boroujeni, A.; Rezaie, E.; Ghaleh, H.E.G.; Aghamollaei, H.; Fasihi-Ramandi, M.; et al. Efficacy of a Low Dose of Melatonin as an Adjunctive Therapy in Hospitalized Patients with COVID-19: A Randomized, Double-blind Clinical Trial. Arch. Med. Res. 2021, 21, 00141–00147. [Google Scholar] [CrossRef] [PubMed]
- Hermel, M.; Sweeney, M.; Ni, Y.M.; Bonakdar, R.; Triffon, D.; Suhar, C.; Mehta, S.; Dalhoumi, S.; Gray, J. Natural Supplements for COVID19-Background, Rationale, and Clinical Trials. J. Evid. Based Integr. Med. 2021, 26, 2515690X211036875. [Google Scholar] [CrossRef]
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; Thornton, C.A.; Whitaker, I.S. Could Vitamins Help in the Fight Against COVID-19? Nutrients 2020, 12, 2550. [Google Scholar] [CrossRef]
- Atkuri, K.R.; Mantovani, J.J.; Herzenberg, L.A.; Herzenberg, L.A. N-Acetylcysteine—A safe antidote for cysteine/glutathione deficiency. Curr. Opin. Pharmacol. 2007, 7, 355–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 | HC | p-Value | ||
|---|---|---|---|---|
| n = 29 | n = 30 | |||
| Age (years) | 59.8 ± 8.2 | 59.1 ± 8.0 | 0.719 | |
| Female, n (%) | 17 (58.6) | 18 (60) | 0.914 | |
| BMI (kg/m2) | 26.5 ± 3.7 | 26.3 ± 3.8 | 0.828 | |
| Ever smoker, n (%) | 14 (50) * | 15 (50) | 1.000 | |
| Comorbidities | ||||
| Hypertension, n (%) | 4 (13.8) | 6 (20) | 0.731 | |
| Chronic cardiac disease (not hypertension), n (%) | 2 (6.9) | 3 (10) | 1.000 | |
| Diabetes mellitus, n (%) | 2 (6.9) | 2 (6.7) | 1.000 | |
| Chronic pulmonary disease, n (%) | 4 (13.8) | 4 (13.3) | 1.000 | |
| Laboratory measurements | ||||
| Serum free thiols (μM) | ↓ | 267.8 ± 50.4 | 295.3 ± 31.2 | 0.014 |
| Hemoglobin (g/dL) | 8.9 [8.7–9.4] | 8.9 [8.4–9.4] | 0.601 | |
| CRP (mg/L) | ↑ | 1.9 [1.1–5.5] | 1.1 [0.7–1.4] | 0.041 |
| WBC (×10⁹/L) | ↓ | 4.3 [3.6–5.9] | 5.6 [4.8–7.1] | 0.001 |
| Platelets (×10⁹/L) | 228.1 ± 60.8 | 252.6 ± 68.5 | 0.157 | |
| Albumin (g/L) | ↓ | 44.0 ± 3.2 | 45.7 ± 2.2 | 0.020 |
| eGFR (mL/min × 1.73 m²) | 86.0 [78.0–95.0] | 86.0 [74.5–96.0] | 0.967 | |
| Creatinine (μmol/L) | 71.0 [61.0–80.0] | 75.0 [65.5–86.0] | 0.277 | |
| COVID-19 | HC | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| St. β * | p-Value | St. β * | p-Value | St. β * | p-Value | St. β * | p-Value | |
| Age | −0.178 | 0.357 | −0.497 | 0.005 | −0.401 | 0.011 | ||
| Gender | −0.019 | 0.920 | −0.220 | 0.242 | ||||
| BMI | −0.258 | 0.185 | −0.027 | 0.887 | ||||
| Laboratory measurements | ||||||||
| Hemoglobin (g/dL) | 0.183 | 0.353 | 0.345 | 0.062 | ||||
| CRP (mg/L) | −0.434 | 0.027 | −0.280 | 0.134 | ||||
| WBC (×10⁹/L) | 0.215 | 0.272 | −0.247 | 0.188 | ||||
| Platelets (×10⁹/L) | 0.129 | 0.514 | 0.029 | 0.880 | ||||
| Albumin (g/L) | 0.710 | <0.001 | 0.641 | <0.001 | 0.571 | 0.001 | 0.494 | 0.002 |
| eGFR (mL/min × 1.73 m²) | 0.147 | 0.463 | 0.481 | 0.008 | ||||
| Creatinine (μmol/L) | −0.017 | 0.932 | −0.201 | 0.288 | ||||
| COVID-19, Day 0 | COVID-19, Day 7 | p-Value | ||
|---|---|---|---|---|
| n = 29 | n = 29 | |||
| Serum free thiols (μM) | 267.8 ± 50.4 | ↓ | 247.0 ± 48.5 | 0.001 |
| Hemoglobin (g/dL) | 9.1 ± 0.7 | ↓ | 8.9 ± 0.7 | 0.006 |
| CRP (mg/L) | 1.9 [1.0–5.5] | 2.9 [0.9–9.5] | 0.170 | |
| WBC (×10⁹/L) | 4.3 [3.6–5.9] | 4.8 [4.0–6.3] | 0.063 | |
| Platelets (×10⁹/L) | 228.1 ± 60.8 | 249.3 ± 57.7 | 0.117 | |
| Albumin (g/L) | 44.0 ± 3.2 | ↓ | 42.6 ± 3.0 | 0.001 |
| eGFR (mL/min × 1.73 m²) | 85.1 ± 13.4 | ↑ | 88.9 ± 11.9 | 0.010 |
| Creatinine (μmol/L) | 71.0 [61.0–80.0] | ↓ | 69.0 [59.0–82.0] | 0.005 |
| Non-Hospitalized | Hospitalized | p-Value | ||
|---|---|---|---|---|
| n = 29 | n = 7 | |||
| Serum free thiols (μM) | 255.5 [233.8–296.8] | 262.1 [206.4–268.1] | 0.325 | |
| Hemoglobin (g/dL) | 8.9 [8.7–9.4] | 8.8 [7.9–9.4] | 0.479 | |
| CRP (mg/L) | 1.9 [1.0–5.5] | ↑ | 48.0 [9.0–81.0] | <0.001 |
| WBC (×10⁹/L) | 4.3 [3.6–5.9] | 4.8 [3.4–7.7] | 0.952 | |
| Platelets (×10⁹/L) | 230.0 [169.3–265.8] | 173.0 [144.0–207.0] | 0.079 | |
| Albumin (g/L) | 44.0 [42.0–46.0] | ↓ | 39.1 [37.7–42.1] | 0.010 |
| eGFR (mL/min × 1.73 m²) | 86.0 [78.0–95.0] | 69.1 [68.9–84.1] | 0.109 | |
| Creatinine (μmol/L) | 71.0 [61.0–80.0] | ↑ | 91.8 [85.5–97.2] | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Eijk, L.E.; Tami, A.; Hillebrands, J.-L.; den Dunnen, W.F.A.; de Borst, M.H.; van der Voort, P.H.J.; Bulthuis, M.L.C.; Veloo, A.C.M.; Wold, K.I.; Vincenti González, M.F.; et al. Mild Coronavirus Disease 2019 (COVID-19) Is Marked by Systemic Oxidative Stress: A Pilot Study. Antioxidants 2021, 10, 2022. https://doi.org/10.3390/antiox10122022
van Eijk LE, Tami A, Hillebrands J-L, den Dunnen WFA, de Borst MH, van der Voort PHJ, Bulthuis MLC, Veloo ACM, Wold KI, Vincenti González MF, et al. Mild Coronavirus Disease 2019 (COVID-19) Is Marked by Systemic Oxidative Stress: A Pilot Study. Antioxidants. 2021; 10(12):2022. https://doi.org/10.3390/antiox10122022
Chicago/Turabian Stylevan Eijk, Larissa E., Adriana Tami, Jan-Luuk Hillebrands, Wilfred F. A. den Dunnen, Martin H. de Borst, Peter H. J. van der Voort, Marian L. C. Bulthuis, Alida C. M. Veloo, Karin I. Wold, María F. Vincenti González, and et al. 2021. "Mild Coronavirus Disease 2019 (COVID-19) Is Marked by Systemic Oxidative Stress: A Pilot Study" Antioxidants 10, no. 12: 2022. https://doi.org/10.3390/antiox10122022
APA Stylevan Eijk, L. E., Tami, A., Hillebrands, J. -L., den Dunnen, W. F. A., de Borst, M. H., van der Voort, P. H. J., Bulthuis, M. L. C., Veloo, A. C. M., Wold, K. I., Vincenti González, M. F., van der Gun, B. T. F., van Goor, H., & Bourgonje, A. R. (2021). Mild Coronavirus Disease 2019 (COVID-19) Is Marked by Systemic Oxidative Stress: A Pilot Study. Antioxidants, 10(12), 2022. https://doi.org/10.3390/antiox10122022