





Computational Fluid Dynamics Analysis of Varied Cross-Sectional Areas in Sleep Apnea Individuals across Diverse Situations

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
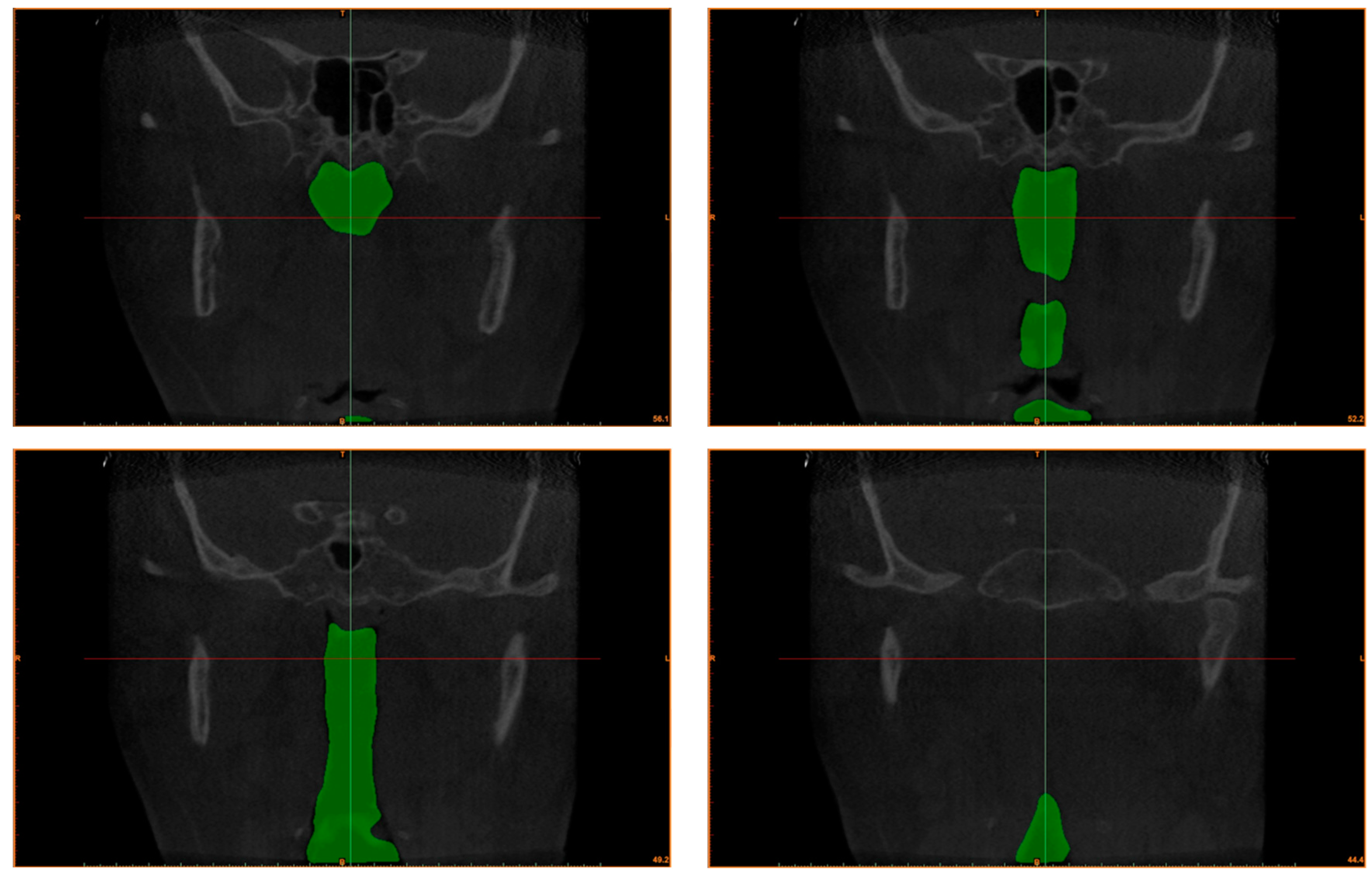
2.1. Subject
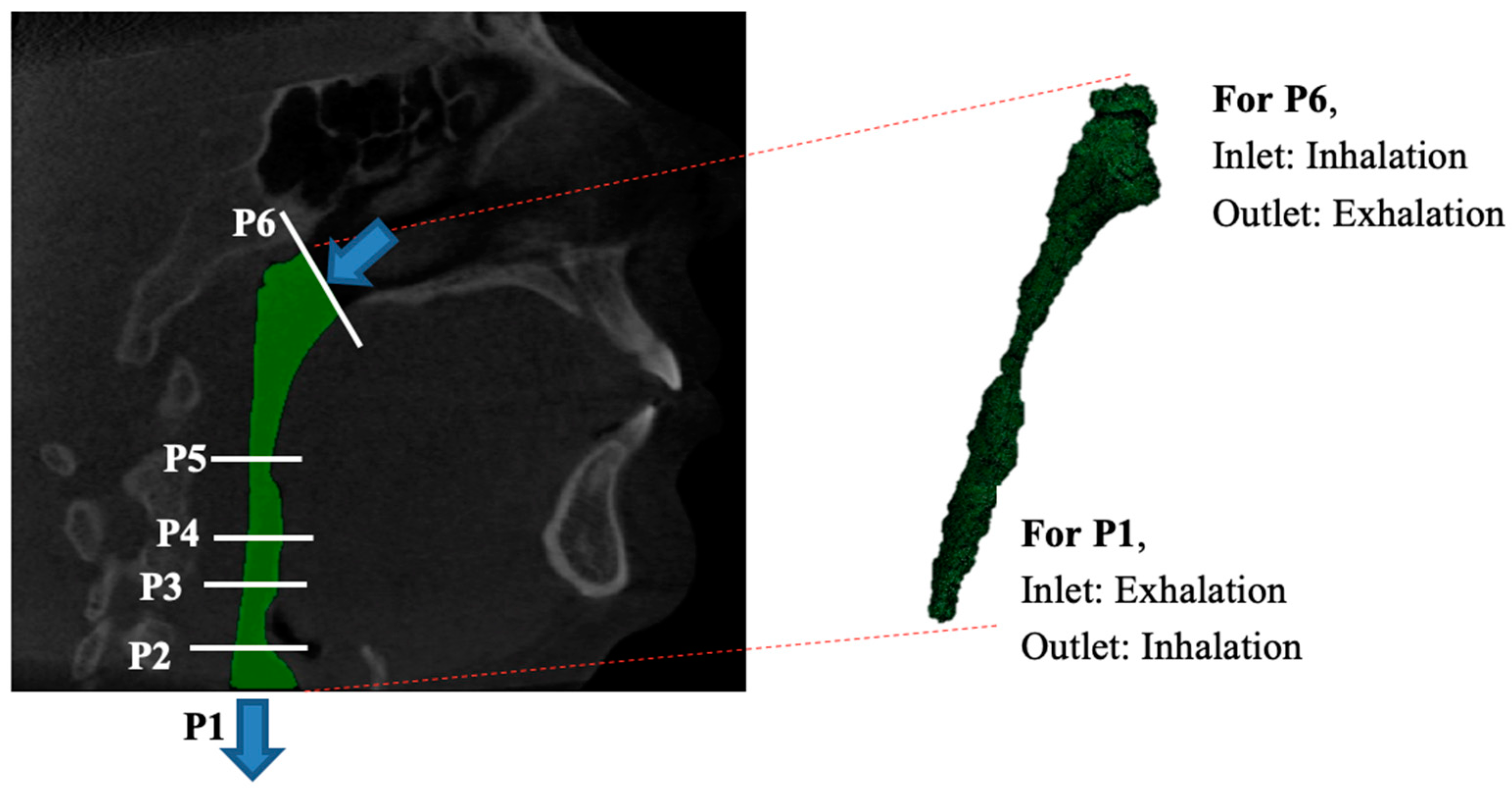
2.2. Numerical Modeling
2.3. TKE Model and Turbulent Reynolds Number
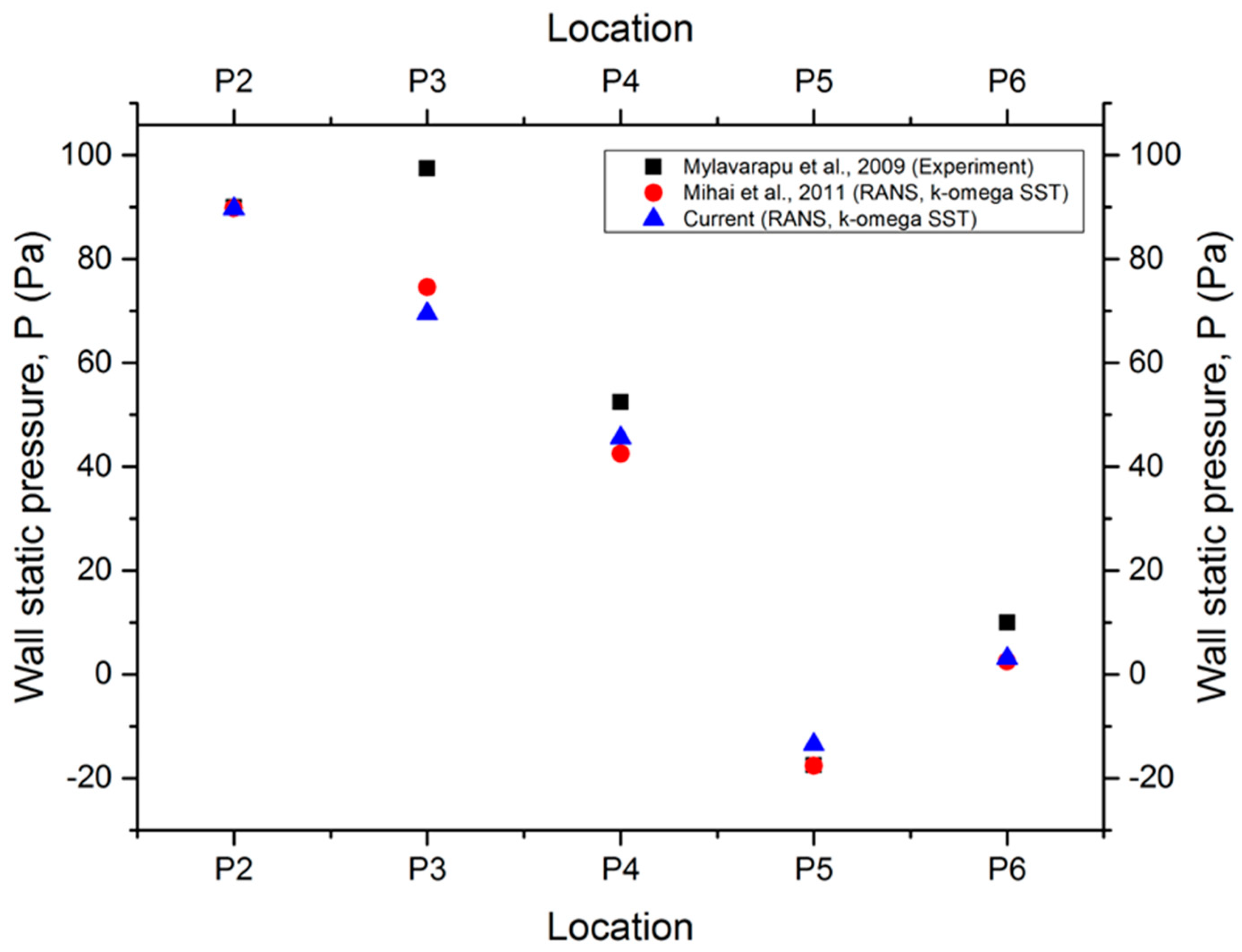
2.4. Grid Sensitivity and Solver Verification
3. Results and Discussion
3.1. Cross-Sectional Area
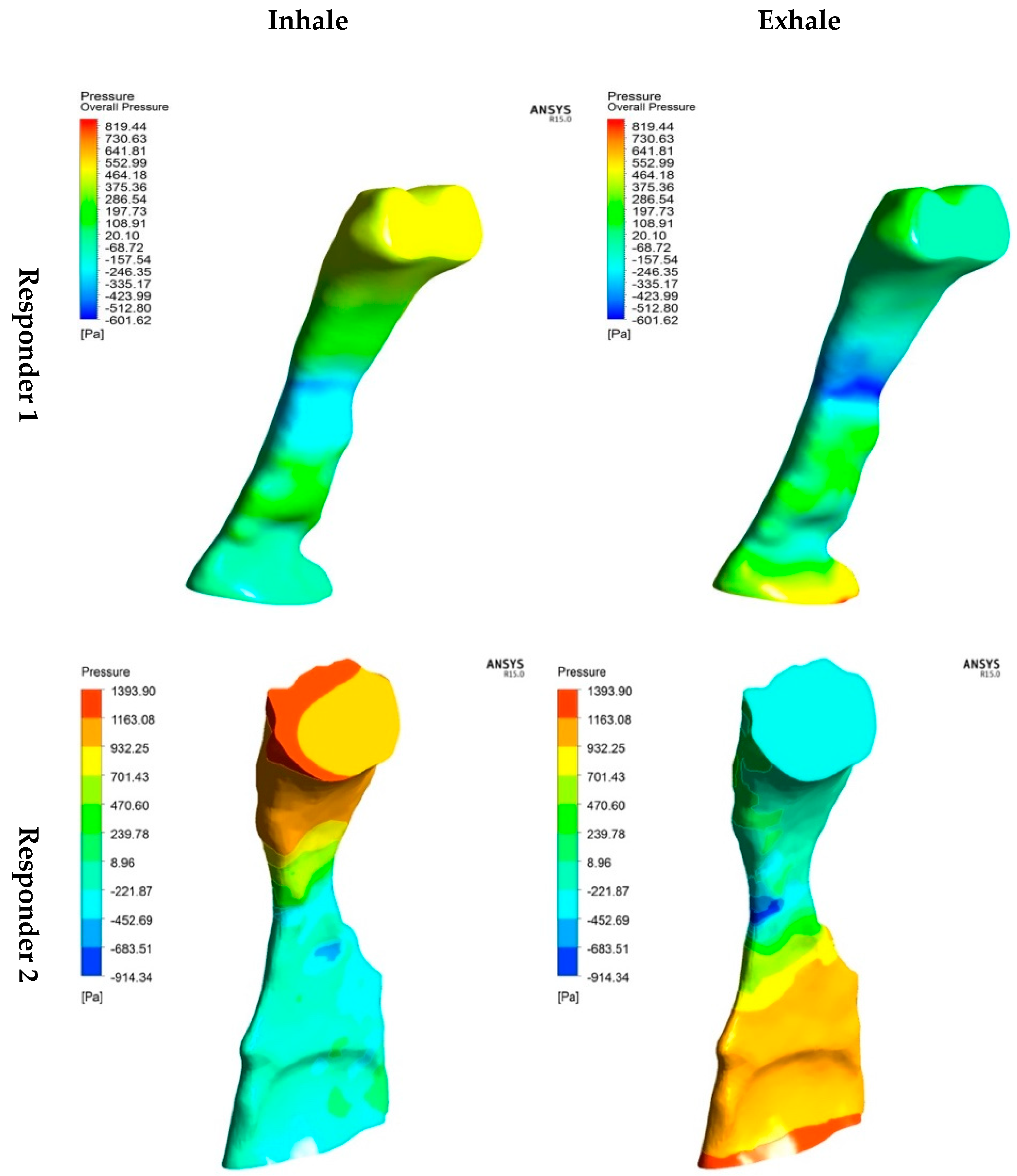
3.2. Static Pressure
3.3. Velocity
3.4. Turbulent Reynolds Number
3.5. Turbulent Kinetic Energy
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wang, J.; Zhao, Y.; Yang, W.; Shen, T.; Xue, P.; Yan, X.; Chen, D.; Qiao, Y.; Chen, M.; Ren, R.; et al. Correlations between obstructive sleep apnea and adenotonsillar hypertrophy in children of different weight status. Sci. Rep. 2019, 9, 11455. [Google Scholar] [CrossRef] [PubMed]
- Tham, K.W.; Lee, P.C.; Lim, C.H. Weight Management in Obstructive Sleep Apnea: Medical and Surgical Options. Sleep Med. Clin. 2019, 14, 143–153. [Google Scholar] [CrossRef]
- Corda, J.V.; Shenoy, B.S.; Ahmad, K.A.; Lewis, L.; Prakashini, K.; Khader, S.M.A.; Zuber, M. Nasal airflow comparison in neonates, infant and adult nasal cavities using computational fluid dynamics. Comput. Methods Programs Biomed. 2022, 214, 106538. [Google Scholar] [CrossRef] [PubMed]
- Modena, D.A.O.; Cazzo, E.; Candido, E.C.; Baltieri, L.; Silveira, L.; Almeida, A.M.N.; Gobato, R.C.; Chaim, E.A. Obstructive sleep apnea syndrome among obese individuals: A cross-sectional study. Rev. Assoc. Med. Bras. 2017, 63, 862–868. [Google Scholar] [CrossRef]
- Randerath, W.; Bassetti, C.L.; Bonsignore, M.R.; Farre, R.; Ferini-Strambi, L.; Grote, L.; Hedner, J.; Kohler, M.; Martinez-Garcia, M.A.; Mihaicuta, S.; et al. Challenges and perspectives in obstructive sleep apnoea: Report by an ad hoc working group of the Sleep Disordered Breathing Group of the European Respiratory Society and the European Sleep Research Society. Eur. Respir. J. 2018, 52, 1702616. [Google Scholar] [CrossRef]
- Carberry, J.C.; Amatoury, J.; Eckert, D.J. Personalized Management Approach for OSA. Chest 2018, 153, 744–755. [Google Scholar] [CrossRef]
- Suzuki, M. Obstructive sleep apnea—Consideration of its pathogenesis. Auris Nasus Larynx 2022, 49, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Passali, D.; Passali, F.M.; Cambi, J.; Bellussi, L. Role of adenotonsillectomy in OSAS children and behavioural disturbance. Otolaryngol. Pol. 2013, 67, 187–191. [Google Scholar] [CrossRef]
- Hudgel, D.W.; Patel, S.R.; Ahasic, A.M.; Bartlett, S.J.; Bessesen, D.H.; Coaker, M.A.; Fiander, P.M.; Grunstein, R.R.; Gurubhagavatula, I.; Kapur, V.K.; et al. The Role of Weight Management in the Treatment of Adult Obstructive Sleep Apnea. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e70–e87. [Google Scholar] [CrossRef]
- Lin, H.C.; Friedman, M. Volumetric Tongue Reduction for Obstructive Sleep Apnea. Sleep Med. Clin. 2019, 14, 59–65. [Google Scholar] [CrossRef]
- Lin, H.; Xiong, H.; Ji, C.; Wang, C.; Li, Y.; An, Y.; Li, G.; Guo, J.; Huang, X.; Zhang, H.; et al. Upper airway lengthening caused by weight increase in obstructive sleep apnea patients. Respir. Res. 2020, 21, 272. [Google Scholar] [CrossRef]
- Faizal, W.M.; Ghazali, N.N.N.; Khor, C.Y.; Zainon, M.Z.; Badruddin, I.A.; Kamangar, S.; Ibrahim, N.B.; Razi, R.M. Computational Analysis of Airflow in Upper Airway under Light and Heavy Breathing Conditions for a Realistic Patient Having Obstructive Sleep Apnea. Comput. Model. Eng. Sci. 2021, 128, 583–604. [Google Scholar] [CrossRef]
- Vinha, P.P.; Thuler, E.R.; de Mello-Filho, F.V. Effects of surgically assisted rapid maxillary expansion on the modification of the pharynx and hard palate and on obstructive sleep apnea, and their correlations. J. Craniomaxillofac. Surg. 2020, 48, 339–348. [Google Scholar] [CrossRef]
- Klopper, G.J.; Adeniyi, O.V.; Stephenson, K. Adolescent and adult laryngotracheal stenosis: A review. Egypt. J. Otolaryngol. 2021, 37, 36. [Google Scholar] [CrossRef]
- Yang, I. TLR4 Asp299Gly polymorphism is not associated with coronary artery stenosis. Atherosclerosis 2003, 170, 187–190. [Google Scholar] [CrossRef]
- Buczkowski, P.W.; Fombon, F.N.; Russell, W.C.; Thompson, J.P. Effects of helium on high frequency jet ventilation in model of airway stenosis. Br. J. Anaesth. 2005, 95, 701–705. [Google Scholar] [CrossRef]
- Cheng, T.; Carpenter, D.; Cohen, S.; Witsell, D.; Frank-Ito, D.O. Investigating the effects of laryngotracheal stenosis on upper airway aerodynamics. Laryngoscope 2018, 128, E141–E149. [Google Scholar] [CrossRef]
- Xu, X.; Wu, J.; Weng, W.; Fu, M. Investigation of inhalation and exhalation flow pattern in a realistic human upper airway model by PIV experiments and CFD simulations. Biomech. Model. Mechanobiol. 2020, 19, 1679–1695. [Google Scholar] [CrossRef]
- Ganimedov, V.L.; Muchnaya, M.I. Numerical simulation of particle deposition in the human nasal cavity. Thermophys. Aeromechanics 2020, 27, 303–312. [Google Scholar] [CrossRef]
- Bates, A.J.; Schuh, A.; Amine-Eddine, G.; McConnell, K.; Loew, W.; Fleck, R.J.; Woods, J.C.; Dumoulin, C.L.; Amin, R.S. Assessing the relationship between movement and airflow in the upper airway using computational fluid dynamics with motion determined from magnetic resonance imaging. Clin. Biomech. 2019, 66, 88–96. [Google Scholar] [CrossRef]
- Chan, A.S.; Sutherland, K.; Schwab, R.J.; Zeng, B.; Petocz, P.; Lee, R.W.; Darendeliler, M.A.; Cistulli, P.A. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax 2010, 65, 726–732. [Google Scholar] [CrossRef]
- Powell, N.B.; Mihaescu, M.; Mylavarapu, G.; Weaver, E.M.; Guilleminault, C.; Gutmark, E. Patterns in pharyngeal airflow associated with sleep-disordered breathing. Sleep Med. 2011, 12, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.K.; Kim, K.B.; McQuilling, M.W.; Movahed, R. Fluid structure interaction simulations of the upper airway in obstructive sleep apnea patients before and after maxillomandibular advancement surgery. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Haghnegahdar, A.; Zhao, J.; Kozak, M.; Williamson, P.; Feng, Y. Development of a hybrid CFD-PBPK model to predict the transport of xenon gas around a human respiratory system to systemic regions. Heliyon 2019, 5, e01461. [Google Scholar] [CrossRef]
- Schendel, S.; Powell, N.; Jacobson, R. Maxillary, mandibular, and chin advancement: Treatment planning based on airway anatomy in obstructive sleep apnea. J. Oral. Maxillofac. Surg. 2011, 69, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Wakayama, T.; Suzuki, M.; Tanuma, T. Effect of Nasal Obstruction on Continuous Positive Airway Pressure Treatment: Computational Fluid Dynamics Analyses. PLoS ONE 2016, 11, e0150951. [Google Scholar] [CrossRef] [PubMed]
- Mylavarapu, G.; Mihaescu, M.; Fuchs, L.; Papatziamos, G.; Gutmark, E. Planning human upper airway surgery using computational fluid dynamics. J. Biomech. 2013, 46, 1979–1986. [Google Scholar] [CrossRef]
- Wilcox, D.C. Reassessment of the scale-determining equation for advanced turbulence models. Am. Inst. Aeronaut. J. 1988, 26, 1299–1310. [Google Scholar] [CrossRef]
- Faizal, W.M.; Ghazali, N.N.N.; Khor, C.Y.; Zainon, M.Z.; Ibrahim, N.B.; Razif, R.M. Turbulent Kinetic Energy of Flow during Inhale and Exhale to Characterise the Severity of Obstructive Sleep Apnea Patient. Comput. Model. Eng. Sci. 2023, 136, 43–61. [Google Scholar] [CrossRef]
- Mylavarapu, G.; Murugappan, S.; Mihaescu, M.; Kalra, M.; Khosla, S.; Gutmark, E. Validation of computational fluid dynamics methodology used for human upper airway flow simulations. J. Biomech. 2009, 42, 1553–1559. [Google Scholar] [CrossRef]
- Mihaescu, M.; Mylavarapu, G.; Gutmark, E.J.; Powell, N.B. Large eddy simulation of the pharyngeal airflow associated with obstructive sleep apnea syndrome at pre and post-surgical treatment. J. Biomech. 2011, 44, 2221–2228. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, X.; Ma, J. Combined application of pharyngeal volume and minimal cross-sectional area may be helpful in screening persons suspected of obstructive sleep apnea (OSA). Sleep Breath. 2022, 26, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Wang, C.; Zhang, H.; Xiong, H.; Li, Z.; Huang, X.; Ji, C.; Xian, J.; Huang, Y. Threshold of the upper airway cross-section for hypopnea onset during sleep and its identification under waking condition. Respir. Res. 2019, 20, 280. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Kim, J.H.; Yu, H.; Jung, H.D.; Chang, S.W.; Park, J.J.; Hong, S.; Cho, H.J.; Choi, Y.J.; Choi, J.; et al. Diagnosis of obstructive sleep apnea with prediction of flow characteristics according to airway morphology automatically extracted from medical images: Computational fluid dynamics and artificial intelligence approach. Comput. Methods Programs Biomed. 2021, 208, 106243. [Google Scholar] [CrossRef]
- Hu, G.; Grossman, B. The computation of massively separated flows using compressible vorticity confinement methods. Comput. Fluids 2006, 35, 781–789. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Responder 1 | Responder 2 | |
|---|---|---|
| Sex | Female | Male |
| Age (years) | 33 | 44 |
| BMI (kg/m2) | 28.5 | 25.42 |
| OSA Level | 12.5 (Mild) | 27.1 (Moderate) |
| Responder 1 | Responder 2 | Diff (%) | ||
|---|---|---|---|---|
| Cross-sectional area | 7.68 mm2 | 5.42 mm2 | 29.47% | |
| TKE | Inhale | 82.37 | 90.84 | 10.28% |
| Exhale | 64.72 | 71.31 | 10.18% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faizal, W.M.; Khor, C.Y.; Shahrin, S.; Hazwan, M.H.M.; Ahmad, M.; Misbah, M.N.; Haidiezul, A.H.M. Computational Fluid Dynamics Analysis of Varied Cross-Sectional Areas in Sleep Apnea Individuals across Diverse Situations. Computation 2024, 12, 16. https://doi.org/10.3390/computation12010016
Faizal WM, Khor CY, Shahrin S, Hazwan MHM, Ahmad M, Misbah MN, Haidiezul AHM. Computational Fluid Dynamics Analysis of Varied Cross-Sectional Areas in Sleep Apnea Individuals across Diverse Situations. Computation. 2024; 12(1):16. https://doi.org/10.3390/computation12010016
Chicago/Turabian StyleFaizal, W. M., C. Y. Khor, Suhaimi Shahrin, M. H. M. Hazwan, M. Ahmad, M. N. Misbah, and A. H. M. Haidiezul. 2024. "Computational Fluid Dynamics Analysis of Varied Cross-Sectional Areas in Sleep Apnea Individuals across Diverse Situations" Computation 12, no. 1: 16. https://doi.org/10.3390/computation12010016
APA StyleFaizal, W. M., Khor, C. Y., Shahrin, S., Hazwan, M. H. M., Ahmad, M., Misbah, M. N., & Haidiezul, A. H. M. (2024). Computational Fluid Dynamics Analysis of Varied Cross-Sectional Areas in Sleep Apnea Individuals across Diverse Situations. Computation, 12(1), 16. https://doi.org/10.3390/computation12010016