
Histological Evidences of Autograft of Dentin/Cementum Granules into Unhealed Socket at 5 Months after Tooth Extraction for Implant Placement

 ,
,  , and
, and 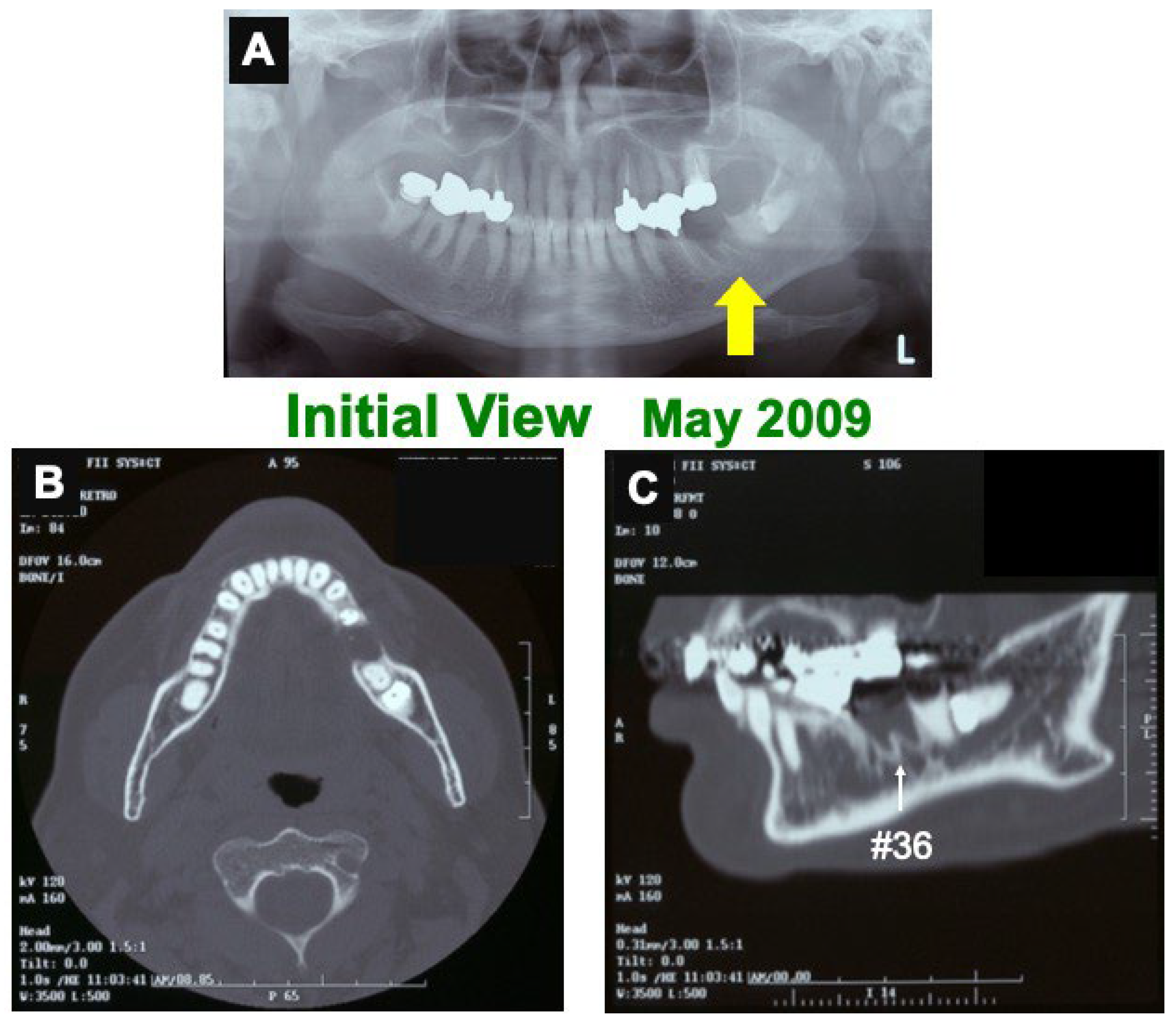{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Case
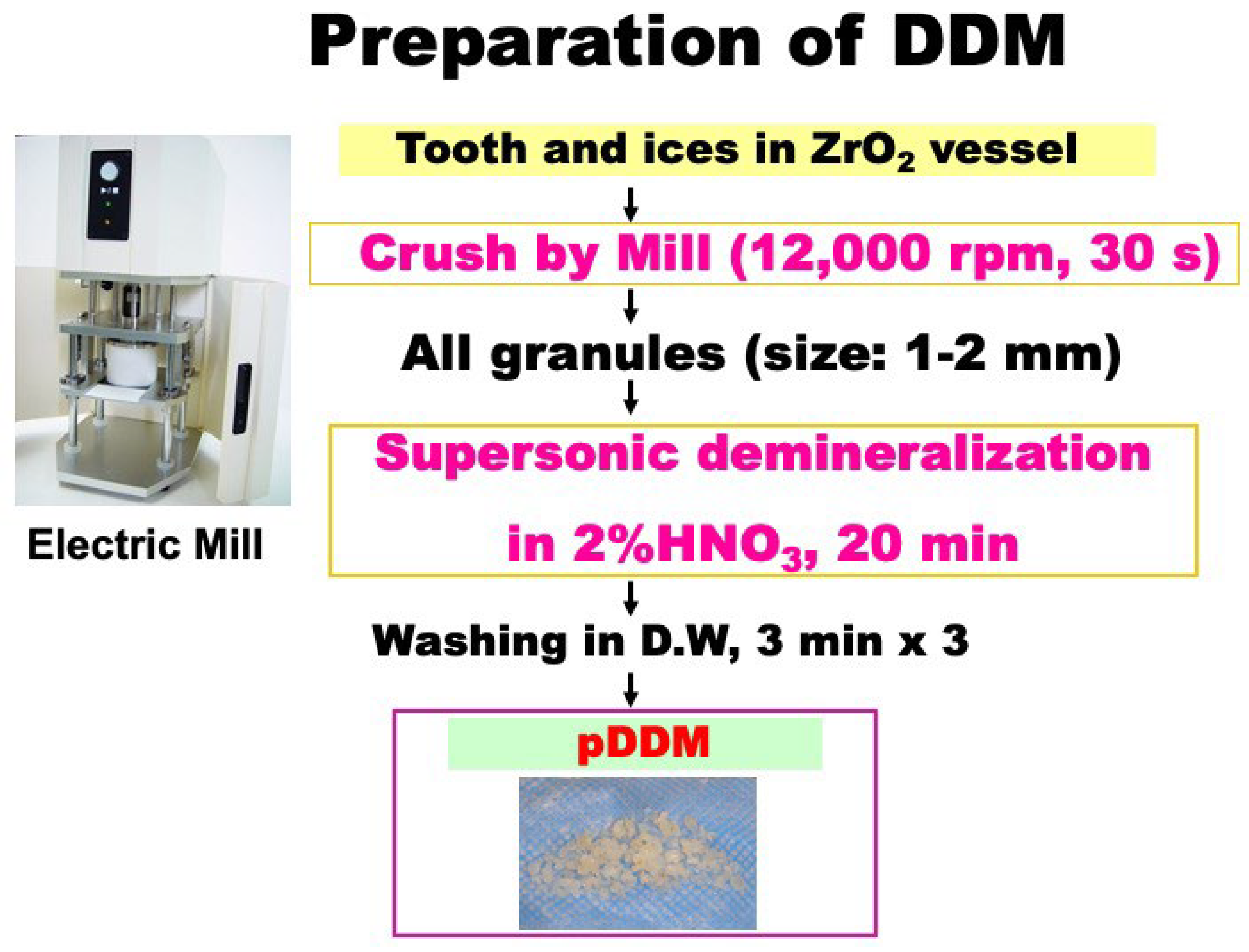
2.2. Surgical Procedure 1 and Preparation of pDDM
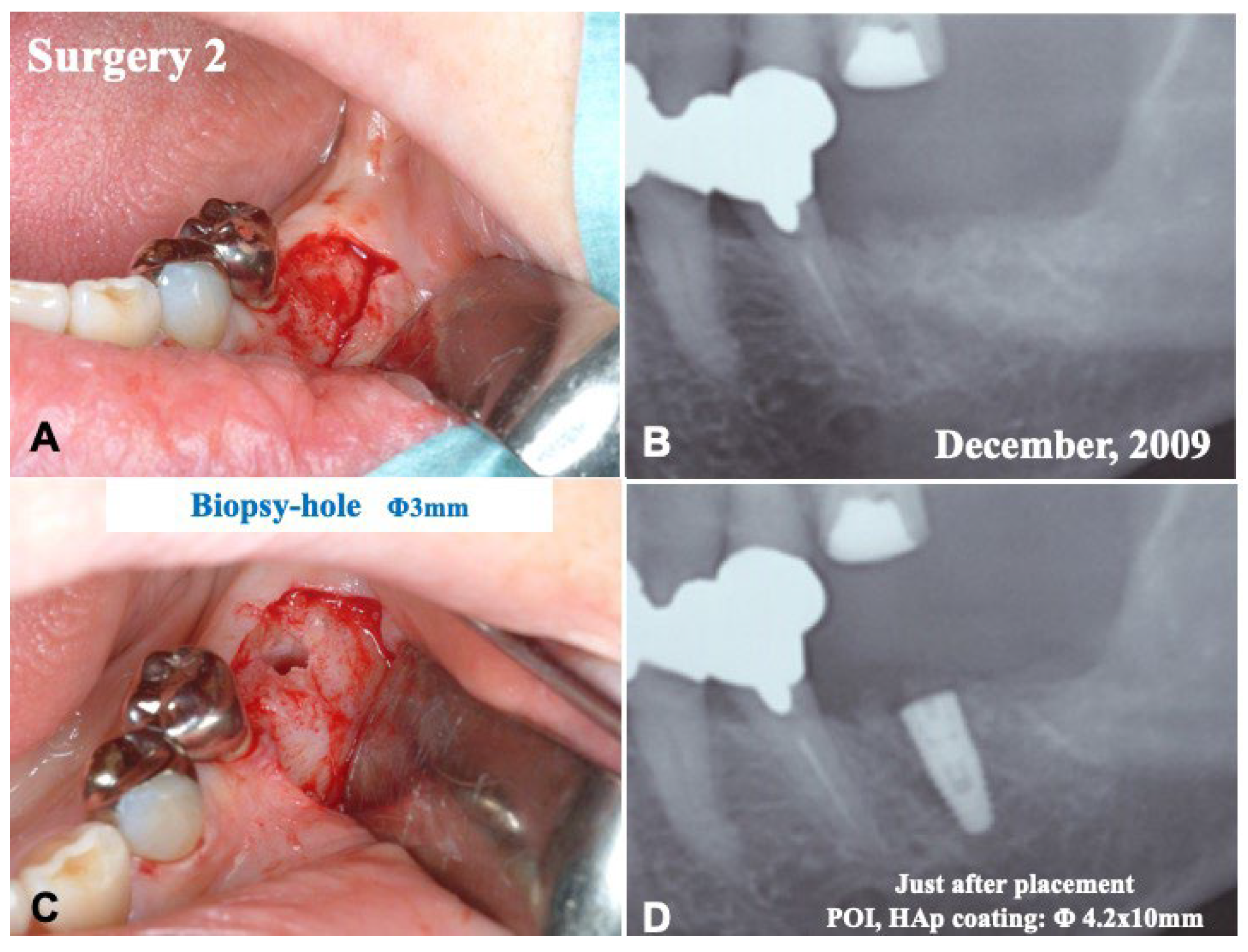
2.3. Surgical Procedure 2 and Tissue Biopsy
2.4. Radiographic Evaluation
2.5. Tissue Preparation
3. Results
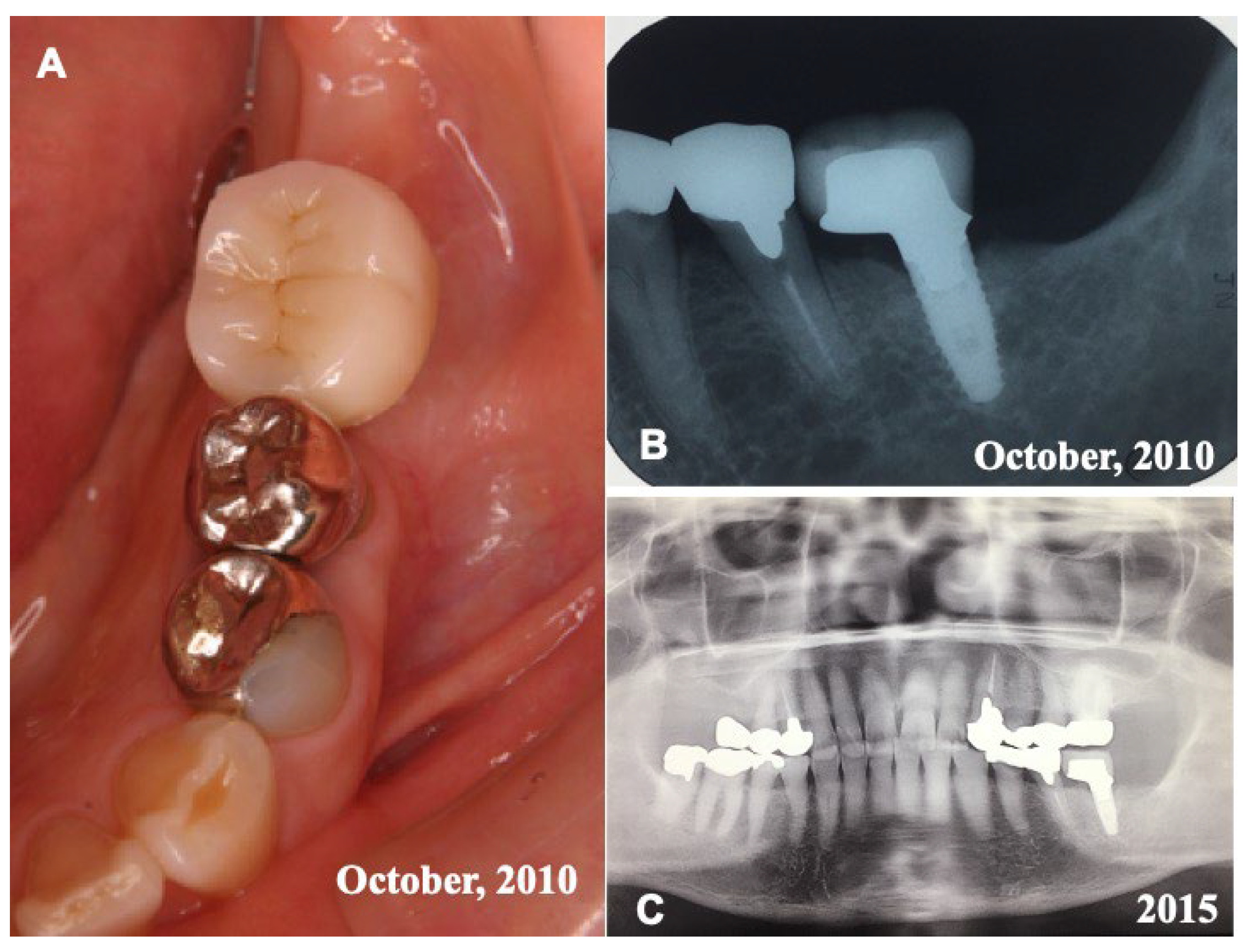
3.1. Gross View and Radiographic Evaluation
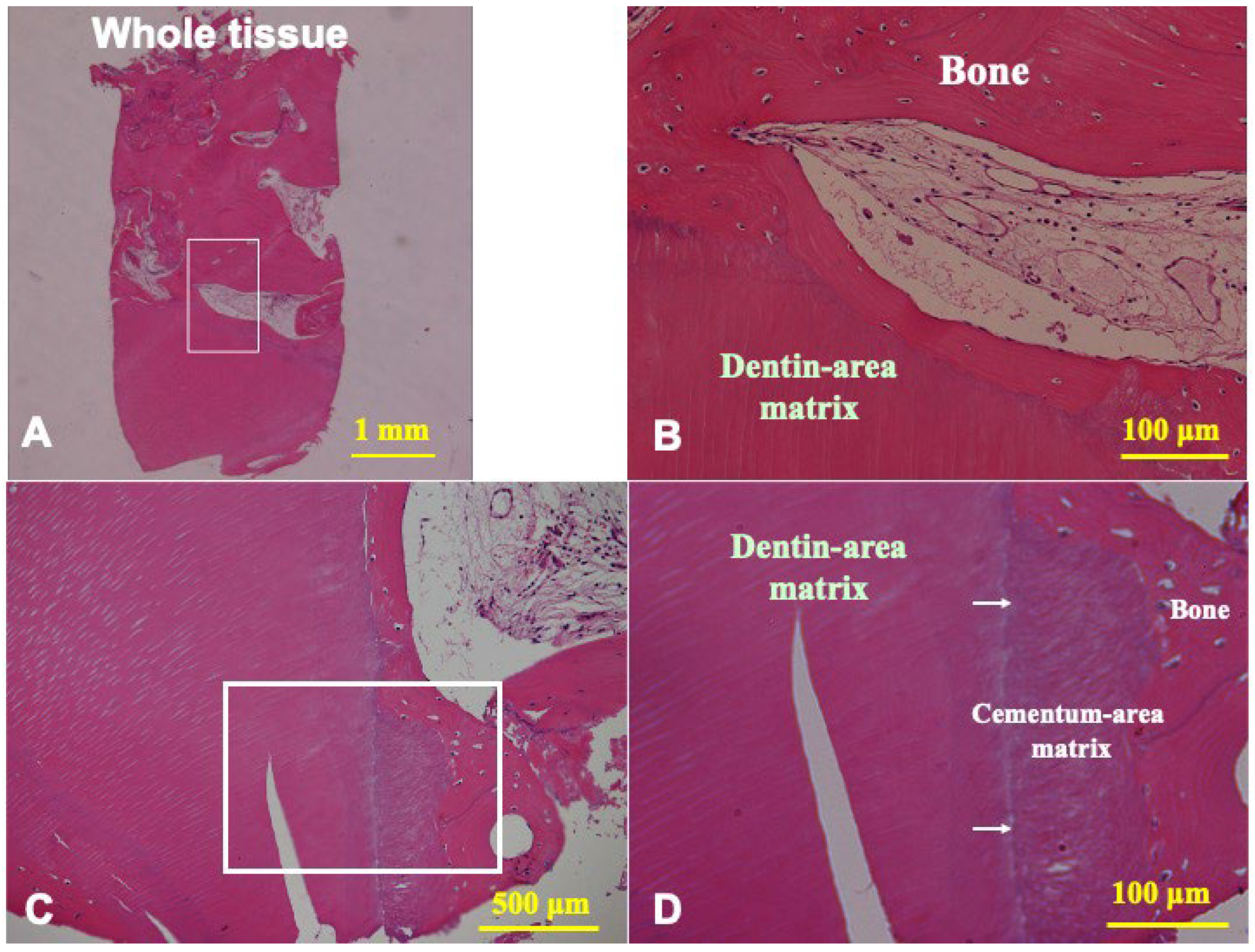
3.2. Histological Findings of Biopsy Tissue at 5 Months after pDDM Autograft
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kamiura, Y.; Kumazawa, R.; Kumazawa, T.; Murata, M.; Akazawa, T. Maxillary implant restration with autograft of decalcified dentin matrix. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co. Inc.: Chicago, IL, USA, 2014; pp. 51–53. [Google Scholar]
- Murata, M.; Akazawa, T.; Mitsugi, M.; Kabir, M.A.; Minamida, Y.; Um, I.W.; Kim, K.W.; Kim, Y.; Sun, Y.; Qin, C. Autograft of Dentin Materials for Bone Regeneration. In Advances in Biomaterials Science and Biomedical Applications; Pignatello, R., Ed.; INTECH Publisher: Rijeka, Croatia, 2013; pp. 391–403. [Google Scholar]
- Akazawa, T.; Murata, M.; Hino, J.; Nakamura, K.; Kikuchi, M.; Mitsugi, M.; Um, I.W. Surfaces design and functional control of demineralized dentin matrix granules derived from human teeth. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 37–42. [Google Scholar]
- Kabir, M.A.; Murata, M.; Kusano, K.; Zakaria, S.M.; Noor, A.H.; Khuda, F.; Hossain, I.; Sultana, S.; Saito, T. Radiological evaluation of human dentin autografts in Bangladesh. J. Hard Tissue Biol. 2014, 23, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Zhu, H.; Huang, D. Autogenous DDM versus Bio-Oss granules in GBR for immediate implantation in periodontal postextraction sites: A prospective clinical study. Clin. Implant. Dent. Relat. Res. 2018, 20, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, Y.K.; Park, Y.H.; Park, J.C.; Ku, J.K.; Um, I.W.; Kim, J.Y. Evaluation of the healing potential of demineralized dentin matrix fixed with recombinant human bone morphogenetic protein-2 in bone grafts. Materials 2017, 10, 1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Um, I.W.; Ku, J.K.; Kim, Y.M.; Yun, P.Y.; Chang, N.H.; Kim, Y.K.; Choi, Y. Allogenic demineralized dentin matrix graft for guided bone regeneration in dental implants. Appl. Sci. 2020, 10, 4661. [Google Scholar] [CrossRef]
- Umebayashi, M.; Ohba, S.; Kurogi, T.; Noda, S.; Asahina, I. Full regeneration of maxillary alveolar bone using autogenous partially demineralized dentin matrix and particulate cancellous bone and marrow for implant-supported full arch rehabilitation. J. Oral Implantol. 2020, 1, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Okubo, N.; Ishikawa, M.; Shakya, M.; Hosono, H.; Maehara, O.; Ohkawara, T.; Ohnishi, S.; Akazawa, T.; Murata, M. Autograft of demineralized dentin matrix prepared immediately after extraction for horizontal bone augmentation of the anterior atrophic maxilla: A first case of non-vital tooth-derived dentin. J. Hard Tissue Biol. 2022, 23, 363–370. [Google Scholar] [CrossRef]
- Um, I.W.; Lee, J.K. Familial tooth bone graft. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 67–72. [Google Scholar]
- Murata, M.; Okubo, N.; Shakya, M.; Kabir, M.A.; Yokozeki, K.; Zhu, B.W.; Ishikawa, M.; Kitamura, R.; Akazawa, T. Dentin Materials as Biological Scaffolds for Tissue Engineering. In Biomaterial-Supported Tissue Reconstruction or Regeneration; IntechOpen: London, UK, 2019; pp. 25–36. [Google Scholar]
- Bang, G.; Urist, M.R. Bone induction in excavation chambers in matrix of decalcified dentin. Arch. Surg. 1964, 94, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, J.D.; Urist, M.R. Bone induction by decalcified dentine implanted into oral, osseous and muscle tissues. Arch. Oral Biol. 1964, 12, 999–1008. [Google Scholar] [CrossRef]
- Huggins, C.; Wiseman, S.; Reddi, A.H. Transformation of fibroblasts by allogeneic and xenogeneic transplants of demineralized tooth and bone. J. Exp. Med. 1970, 132, 1250–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakya, M.; Yokozeki, K.; Akazawa, T.; Murata, M. Rapid bone induction of cortical bone treated with ultrasonic demineralization in acidic electrolyzed water. J. Hard Tissue Biol. 2018, 27, 269–271. [Google Scholar] [CrossRef] [Green Version]
- Koga, T.; Minamizato, T.; Kawai, Y.; Miura, K.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone regeneration using dentin matrix depends on the degree of demineralization and particle size. PLoS ONE 2016, 11, e0147235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakya, M.; Murata, M.; Yokozeki, K.; Akazawa, T.; Nagayasu, H.; Adhikari, B.R.; Upadhyaya, C. Accelerated bone induction of adult rat compact bone plate scratched by ultrasonic scaler using acidic electrolyzed water. Materials 2021, 17, 3347. [Google Scholar] [CrossRef] [PubMed]
- Murata, M.; Akazawa, T.; Takahata, M.; Ito, M.; Tazaki, J.; Hino, J.; Nakamura, K.; Iwasaki, N.; Shibata, T.; Arisue, M. Bone induction of human tooth and bone crushed by newly developed automatic mill. J. Ceram. Soc. Jpn. 2010, 118, 434–437. [Google Scholar] [CrossRef] [Green Version]
- Murata, M.; Maki, F.; Sato, D.; Shibata, T.; Arisue, M. Bone augmentation by onlay implant using recombinant human BMP-2 and collagen on adult rat skull without periosteum. Clin. Oral Implant. Res. 2000, 11, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Finkelman, R.D.; Mohan, S.; Jennings, J.C.; Taylor, A.K.; Jepsen, S.; Baylink, D.J. Quantitation of growth factors IGF-I, SGF/IGF-II, and TGF-beta in human dentin. J. Bone Min. Res. 1990, 5, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Arakawa, T.; Murata, M.; Takuma, T.; Arisue, M. Expression of bone morphogenetic proteins (BMPs) in human dental pulp tissues. J. Hard Tissue Biol. 2007, 16, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Urist, M.R.; Iwata, H.; Ceccotti, P.L.; Dorfman, R.L.; Boyd, S.D.; McDowell, R.M.; Chien, C. Bone morphogenesis in implants of insoluble bone gelatin. Proc. Nat. Acad. Sci. USA 1973, 70, 3511–3515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddi, A.H. Bone matrix in the solid state: Geometric influence on differentiation of fibroblasts. Adv. Biol. Med. Phys. 1974, 15, 1–18. [Google Scholar] [PubMed]
- Luyten, F.P.; Cunningham, N.S.; Ma, S.; Muthukumaran, N.; Hammonds, R.G.; Nevins, W.B.; Woods, W.I.; Reddi, A.H. Purification and partial amino acid sequence of osteogenin, a protein initiating bone differentiation. J. Biol. Chem. 1989, 264, 13377–13380. [Google Scholar] [CrossRef]
- Fujita, M.; Uehara, O.; Miyakawa, H.; Naito, S.; Kabir, M.A.; Murata, M.; Nakazawa, F. Detection of bacteria in human tooth-derived biomaterials. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 31–32. [Google Scholar]
- Patil, S.; Alkahtani, A.; Bhandi, S.; Mashyakhy, M.; Alvarez, M.; Alroomy, R.; Hendi, A.; Varadarajan, S.; Reda, R.; Raj, A.T.; et al. Ultrasound imaging versus radiographs in differentiating periapical lesions: A systematic review. Diagnostics 2021, 3, 1208. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murata, M.; Kabir, M.A.; Hirose, Y.; Ochi, M.; Okubo, N.; Akazawa, T.; Kashiwazaki, H. Histological Evidences of Autograft of Dentin/Cementum Granules into Unhealed Socket at 5 Months after Tooth Extraction for Implant Placement. J. Funct. Biomater. 2022, 13, 66. https://doi.org/10.3390/jfb13020066
Murata M, Kabir MA, Hirose Y, Ochi M, Okubo N, Akazawa T, Kashiwazaki H. Histological Evidences of Autograft of Dentin/Cementum Granules into Unhealed Socket at 5 Months after Tooth Extraction for Implant Placement. Journal of Functional Biomaterials. 2022; 13(2):66. https://doi.org/10.3390/jfb13020066
Chicago/Turabian StyleMurata, Masaru, Md Arafat Kabir, Yukito Hirose, Morio Ochi, Naoto Okubo, Toshiyuki Akazawa, and Haruhiko Kashiwazaki. 2022. "Histological Evidences of Autograft of Dentin/Cementum Granules into Unhealed Socket at 5 Months after Tooth Extraction for Implant Placement" Journal of Functional Biomaterials 13, no. 2: 66. https://doi.org/10.3390/jfb13020066
APA StyleMurata, M., Kabir, M. A., Hirose, Y., Ochi, M., Okubo, N., Akazawa, T., & Kashiwazaki, H. (2022). Histological Evidences of Autograft of Dentin/Cementum Granules into Unhealed Socket at 5 Months after Tooth Extraction for Implant Placement. Journal of Functional Biomaterials, 13(2), 66. https://doi.org/10.3390/jfb13020066