1. Introduction
Psoriasis is classified as an autoimmune disease that affects 1–3% of the population. The exact pathogenesis of this disease is unknown, but it is assumed that genetic and environmental factors have an important role. Psoriasis is manifested through reddish-brown papules on the body, usually covered with silvery scales [
1,
2]. The lesions tend to spread circumferentially and merge with each other. The turn over time in patients with psoriasis is reduced to 3–4 days. Within the psoriatic lesions, the microvascular system is dysfunctional. Overgrown dermal papillae contain dilated and tortuous capillary loops. Research by Golińska and others shows that the diameter of the capillary bushes presenting in psoriatic plaques was 50–146 μm [
3,
4,
5]. The increased microcirculation of the skin plays a significant role in the development and maintenance of the inflammation associated with psoriasis, as it enables the movement of leukocytes from the bloodstream to the skin. Therefore, inhibiting leukocyte transport by selectively damaging dilated blood vessels may be an effective treatment for psoriasis [
4,
5]. The genetic background of psoriasis makes it impossible to cure it completely. The purpose of the available therapy is to reduce psoriatic changes, improve the quality of life and lead to an extension of the remission period. Thus far, there are no known methods that would completely cure psoriasis, but new, more effective therapies, tailored to the needs of patients, are still being developed [
6]. Conventional systemic treatments for psoriasis (methotrexate, cyclosporin A and acitretin) present some limitations, such as an unfavorable safety profile and cumulative toxicity of target organs, which does not make them an ideal choice for long-term therapy. Biological drugs are an interesting alternative, but their long-term side effects are still unknown [
7,
8]. Topical treatments may be insufficient for patients with moderate to severe forms of psoriasis. Phototherapy contributes to a significant reduction in the PASI index (psoriasis area and severity index), but it is associated with numerous and regular irradiations. It commonly covers the irradiation of the total body surface, which may lead to an increased risk of skin cancer. An alternative to this type of treatment could be laser therapy, particularly for patients with small numbers of psoriatic changes and lesions located in areas difficult to treat. Laser therapy has the possibility to focus on the lesional skin, avoiding unaffected areas and not requiring the irradiation of the whole body [
9,
10,
11,
12].
Studies recently published in the literature have confirmed the usefulness of the Nd:YAG laser in the therapy of psoriasis. The Nd:YAG laser emits wavelengths of 1064 nm, which are absorbed primarily by oxyhemoglobin, but also melanin and water [
13,
14]. The Nd:YAG laser light penetrates to a depth of 5–6 mm, and the wavelength falls within the wide absorption band of hemoglobin (800–1100 nm) [
15,
16]. The effect of the Nd:YAG laser is related to selective light absorption by oxyhemoglobin, causing the photothermolysis of blood vessels without damaging other tissue [
5]. The laser causes the destruction of the dilated capillaries, which contributes to the inhibition of leukocyte transport within psoriatic lesions and may be an effective method of psoriasis therapy. The degradation of capillaries reduces blood circulation within the affected skin and prevents the supply of nutrients, leading to the reduction in psoriatic lesions.
The most common 1064 nm Nd:YAG lasers have longer pulse durations of 3 to 30 milliseconds. The laser used in the present research has a shorter pulse duration of 650 microseconds, a time below the skin’s thermal relaxation time, allowing the tissue to cool between pulses. This provides greater clinical efficacy and reduces the risk of burns to the surrounding tissue. The pulse is delivered to the skin structure very quickly, resulting in the target tissue having less time to lose heat by conduction to the surrounding area and reaching a high temperature. The rapid heating of the target tissue contributes to its effective destruction [
17].
The aim of the research was (1) to compare skin parameters of uninvolved psoriatic skin and psoriatic plaques, and (2) to evaluate the effectiveness of the Nd:YAG laser with a short pulse duration of 650 μs in the treatment of psoriasis using non-invasive imaging methods.
2. Materials and Methods
2.1. Patients
Twenty volunteers (eleven men, nine women) with a mean age of 35.6 ± 10.5 with stable plaque-type psoriasis were classified in this study. Eleven patients had a positive family history of psoriasis. Half of the respondents noticed the first symptoms of psoriasis between the ages of 20–30, five patients up to the age of 20, four suffered from this disease from childhood and only one after the age of 40. In 14 patients, psoriatic lesions appeared constantly on the skin; only 6 patients had a short period of remission. To date, nineteen subjects used topical steroids, four used phototherapy, two used general treatment and one used biological treatments. Nine patients used home care.
The inclusion criteria for the research were:
The exclusion criteria for the study were:
Use of anti-psoriatic agents for a minimum period of 3 months from the end of treatment;
Pregnancy and breastfeeding;
Existing or past cancers;
Age under 18;
Taking photosensitizing drugs;
Epilepsy;
Tan;
Liver and kidney failure.
2.2. Ethics Statement
The research was conducted after receiving a positive opinion of the Bioethics Committee of the SUM, no. PCN/0022/KB1/12/I/20, on 19 May 2020. All volunteers gave informed consent to participate in the study.
2.3. The Course of the Study
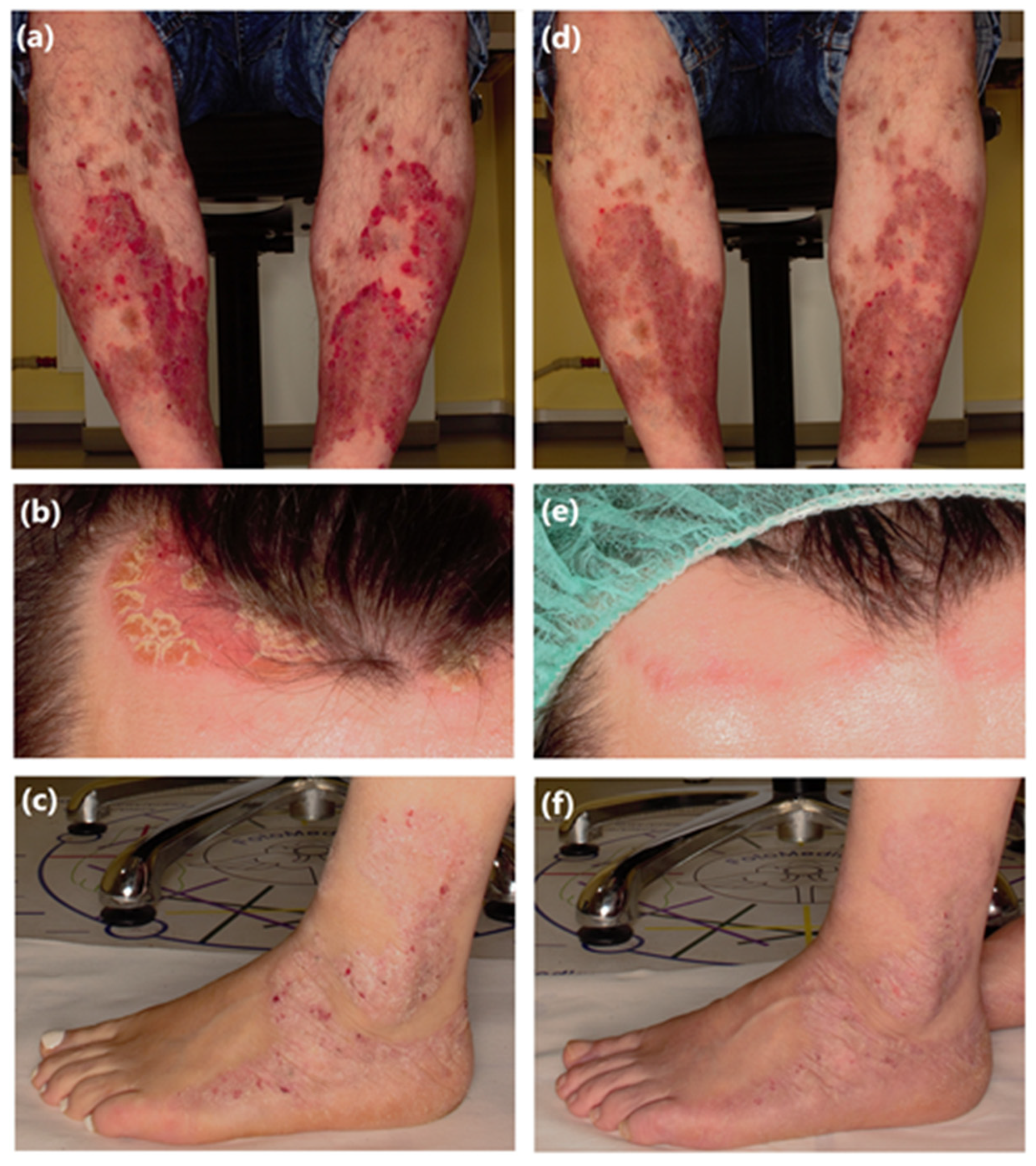
Before the therapy and two weeks after the end of the therapy, the patients had a series of clinical photography performed using the Fotomedicus system (
Figure 1) and dermatoscopic photos using the Firefly dermatoscope (×35 magnification) (
Figure 2).
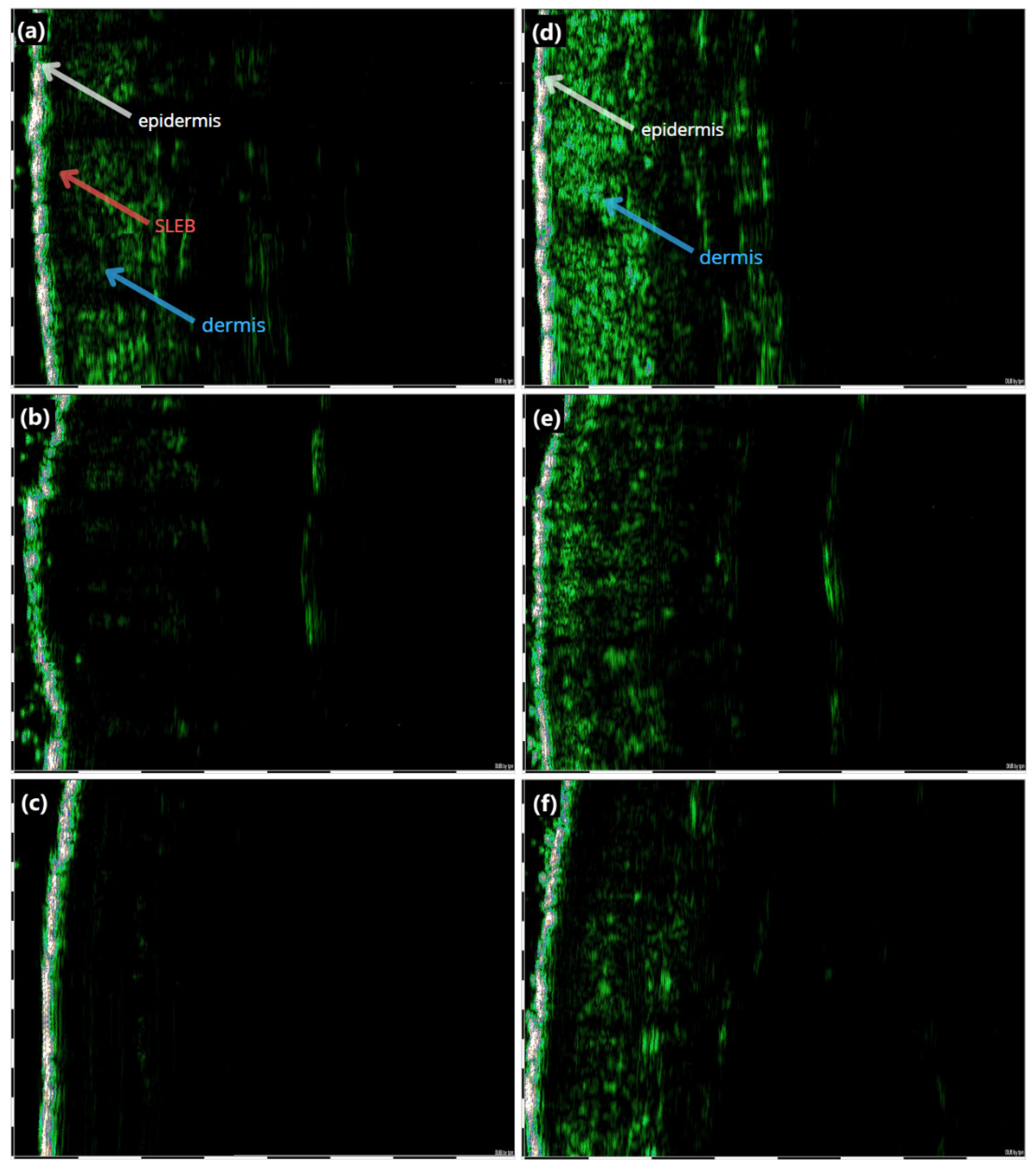
The skin areas affected by psoriatic lesions were imaged using a DUB SkinScanner high-frequency ultrasound equipped with a 33 MHz transducer. The images were captured in presentation B, and then computer-analyzed to determine the epidermal thickness and skin density. The DUB SkinScanner 75 5.21 software was used to perform the measurements within the determined parameters. The thickness of the epidermis was measured as the length between the outer surface of the epidermis and the point of contact with the dermis. Skin density was measured by delineating three regions of interest (ROI) on ultrasound images that included the dermis, and then averaging the results. The thickness of the SLEB (sub-epidermal low-echogenic band) area was also measured before and after the treatment.
Skin hydration (Corneometer® CM 825), melanin and hemoglobin levels (Mexameter® MX 18) (Courage + Khazaka Electronic GmbH, Germany) were measured before and after laser therapy. On the day of imaging, the patients did not apply any cosmetics to their skin.
The Nd:YAG laser with a wavelength of 1064 nm and a pulse duration of 0.65 msec pulse was used to reduce psoriatic lesions. The patients underwent two treatments at two-week intervals. With the use of the laser, areas of the body affected by psoriasis were treated. The treatment parameters were the same for all patients, 2 mm lens, 650-microsecond pulse width and a 255 J/cm2 fluence. One pass of each treatment area was used. At the time of research, patients were not taking substances with an anti-psoriatic effect. The use of skin softeners and moisturizers was allowed.
2.4. Statistical Analysis
Statistical data analysis was conducted with the use of Statistica 13.3 (TIBCO Software, Palo Alto, CA, USA) and MS Excel 2016 (Microsoft, Redmond, WA, USA). The Shapiro–Wilk test was used to assess the normality of data distribution. The paired-samples Wilcoxon test was used to compare the results before and after Nd:YAG laser therapy. p-values less than 0.05 were deemed as significant.
3. Results
Differences in skin density and epidermis thickness between skin without psoriatic lesions and involved psoriatic skin before laser therapy were found (
Figure 3). The differences were statistically significant. Higher skin density values were observed in uninvolved skin compared with psoriatic plaques (Me = 30.3 vs. Me = 4.7) (
Figure 4A). Lower epidermis thickness values were found in uninvolved skin compared with psoriatic plaques (Me = 0.180 vs. Me = 0.320) (
Figure 2b). The effects of the completed laser therapy were skin density and epidermis thickness changes. The difference in skin density and epidermis thickness before and after the therapy were statistically significant. The skin density increased to 11.98 at psoriatic plaques (
p < 0.001). The epidermis thickness decreased to 0.252 at psoriatic plaques (
p < 0.001).
Before the therapy, the median value of the SLEB (sub-epidermal low-echogenic band) was 0.340 mm, while after the therapy it decreased to 0.195 mm (
p < 0.001) (
Figure 5). The reduction in the thickness of the SLEB band indicated a reduction in inflammation caused by the applied laser therapy.
Differences in skin parameters, including the stratum corneum hydration (Me = 37.9 vs. Me = 10.4), melanin (Me = 135 vs. Me = 149) and hemoglobin (Me = 270 vs. Me = 435) values between skin without psoriatic lesions and involved psoriatic skin before laser therapy, were found. The parameters were modified after Nd:YAG laser therapy. The melanin value decreased after laser therapy to 137, but non-significantly (
Figure 6A). The hemoglobin value decreased after laser therapy to 400 at psoriatic plaques (
p < 0.005) (
Figure 6B). The stratum corneum hydration increased after laser therapy to 19.9 at the psoriatic plaques (
p < 0.005) (
Figure 6C). These differences were statistically significant.
4. Discussion
The use of lasers for reducing psoriatic lesions is a response to the search for effective and safe methods of treatment. The aim of laser therapy is the photothermolysis of excessively vascularized psoriatic lesions. There are reports confirming the effectiveness of various types of lasers in the treatment of psoriasis. The most commonly used type of laser is the excimer laser, which is an effective and safe therapy option for psoriatic patients. Abrouk M et al. [
18] demonstrated the effectiveness of the excimer laser in the therapy of lesions in pustular psoriasis on different areas, and in scalp and nails psoriasis. The excimer laser can be used in combination therapy with topical agents, as well as in monotherapy in the case of psoriasis resistant to systemic therapy.
The 1064 nm Nd:YAG laser therapy is used to treat different types of psoriasis, such as plaque psoriasis and nail psoriasis, due to its ability to act on the overly branched and dilated blood vessels in psoriatic skin. In the study by Marta Kołt-Kamińska and others [
19], ten patients underwent four treatments using a Nd:YAG 1064 nm laser with a 650-microsecond pulse width at weekly intervals. Patients showed a significant improvement in all elements of mPASI, with a maximum mean reduction in total mPASI of 30.3%. Before the initiation of treatment, three patients were assessed as “moderate” and seven as “mild” on the IGA scale. In contrast, on the 28th day of initiating the therapy, eight patients were qualified as “mild” and two as “almost clear”. The itching was completely reduced in all participants. Local side effects were also noticed, which caused the treatment to be less tolerable for four patients. Three patients observed a significant improvement in skin condition seven days after the end of treatment, while 30% of patients did not see any benefit. All patients with dotted and linear vessels and hemorrhagic spots observed during pre-treatment dermoscopy noticed some improvement after the therapy. Half of the six patients with globular vessels did not respond to laser. In the studies by Marta Kołt-Kamińska et al. [
19], no clinical response was obtained in some of the patients. In our study, a reduction in psoriatic lesions was observed in all patients. Kołt-Kamińska’s research was qualitative, while our research was quantitative; this allowed us to better assess the effectiveness of the therapy used.
Nestor [
20] compared the effectiveness and safety of a 0.65 msec Nd:YAG laser with an excimer laser in the treatment of mild and moderate forms of psoriatic lesions located on the arms and legs. The effectiveness of the treatments was assessed based on the mPASI score and observation of local skin reactions. Both lasers were effective in treating psoriatic lesions. The differences between the two types of lasers were not significant for the redness, thickness, flaking and mPASI scores. The ratings of the parameters, such as erosion/ulceration, vesicles, erythema, scaling, edema and atrophy, were low and did not differ depending on the laser used.
Rosanne G van Lingen et al. [
21] in their research used the Nd:YAG laser to treat plaque psoriasis. They concluded that the treatments performed every four weeks did not reduce the skin lesions. The authors reported that targeting more superficial blood vessels in psoriasis appeared to produce better clinical outcomes than in deeper vessels. However, they found that further research and methodology changes, especially shortening the intervals between irradiations, were necessary to confirm this position. In the studies of G van Lingen et al. [
21], laser treatments were performed every 4 weeks and did not reduce psoriatic lesions. In our studies, the intervals between treatments were shorter. Treatments were performed at two-week intervals and a reduction in psoriatic lesions was observed in all patients.
The 1064 nm Nd:YAG laser has been used in reducing psoriatic changes on the nails. In the study by Kartal [
22], irradiance with a Nd:YAG laser with a 15-millisecond pulse duration, a 6 mm lens and an energy of 10 J/cm
2 led to the clinical improvement of the nails. Before laser therapy, the mean NAPSI score was 26 ± 7.2. After the first, second and third laser irradiation, the mean NAPSI scores were 22 ± 6.6, 13 ± 6 and 5.7 ± 4.3, respectively. The reduction in the NAPSI score was statistically significant. The condition of the nail bed and matrix significantly improved after the laser treatments. Studies by Ali Elwan [
23] showed an improvement in the nail matrix without a significant improvement in the nail bed after six laser treatments (with the energy used being 110 J/cm
2 in the first irradiation and its gradual increase to 130 J/cm
2). However, there was no statistically significant difference in the assessment of the NAPSI index or the assessment of the nail bed before and after. Psoriatic skin is characterized by a reduced density compared to healthy skin. The reduction in skin density is related to the infiltration of inflammation. In psoriatic skin, the distance between the collagen fibers increases as a result of edema, which contributes to the reduction in tissue density. An ultrasound of psoriatic skin showed a bold entrance echo. The thickness of the epidermis within the skin lesion was increased, and its reduction as a result of the applied therapy could be objectively visualized. Some of the ultrasound examinations of psoriatic skin showed a difference in the thickness of the SLEB band, the measurement of which can be used as an objective parameter monitoring the course of the disease [
24]. The increase in skin density and the reduction in the epidermal thickness after the applied laser therapy proved the effectiveness of the Nd:YAG laser in the therapy of psoriatic lesions. The reduction in the thickness of the SLEB band indicated the reduction in inflammation under the influence of the laser therapy.
Skin with psoriatic lesions is less moisturized than skin without psoriatic changes [
25]. The increase in the stratum corneum hydration proved the positive effect of the therapy on the epidermal barrier function. The decrease in the hemoglobin value after the laser therapy in the area of psoriatic lesions proved the closure of blood vessels and reduction in inflammation.
The limitations of the study were:


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





