

Therapy for Temporomandibular Disorders: 3D-Printed Splints from Planning to Evaluation

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Etiology of Temporomandibular Disorders
1.2. Treatment Options of Temporomandibular Disorders
2. Materials and Methods
2.1. Intraoral Scanner, Digital Facebow, 3D CAD Design and 3D Printing
- Trios 3 wireless intraoral scanner (3Shape Unite, software version 21.4, Copenhagen, Denmark);
- Zebris for Ceramill digital facebow device (software version: 1.2.4, Amman Girrbach, Pforzheim, Germany);
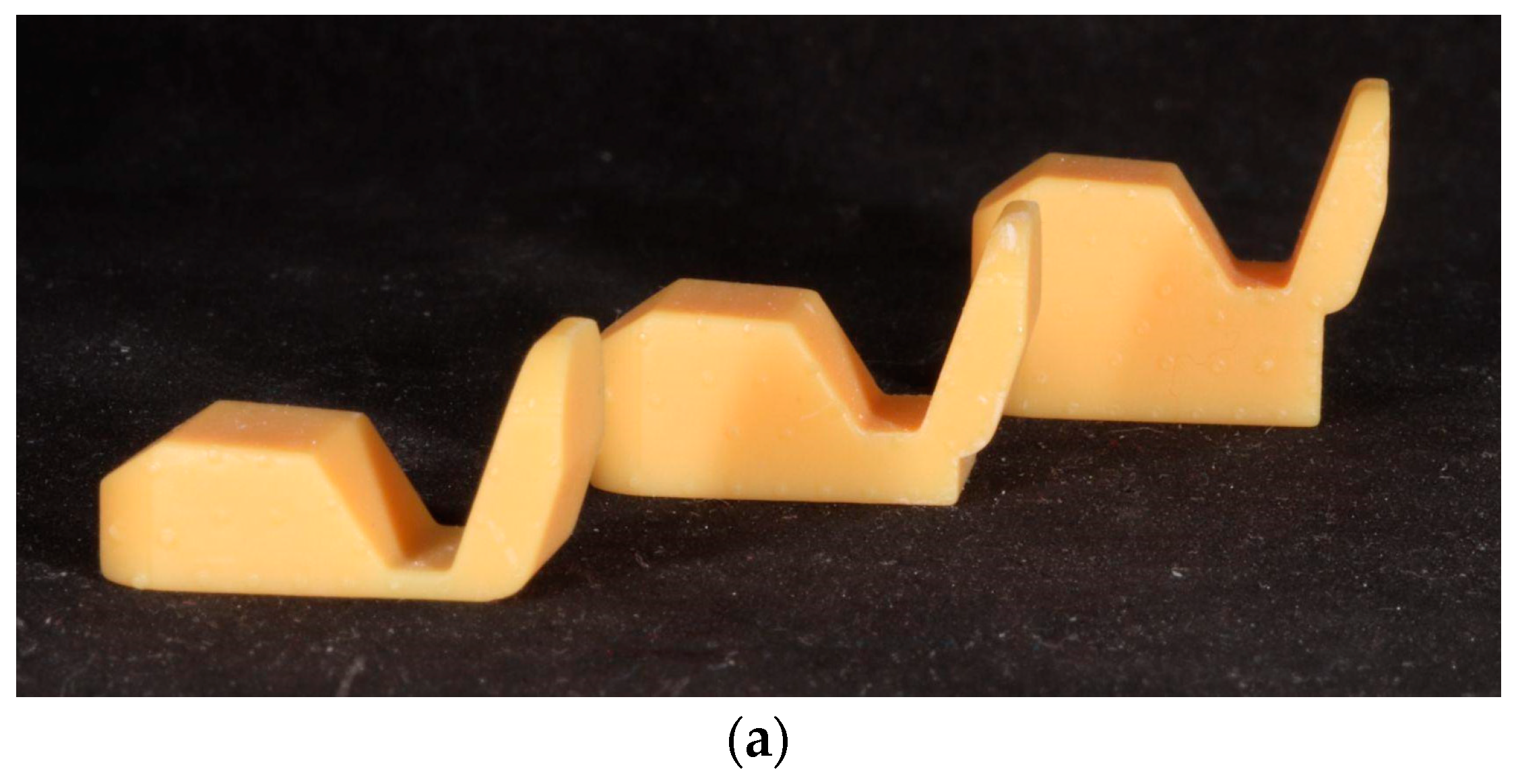
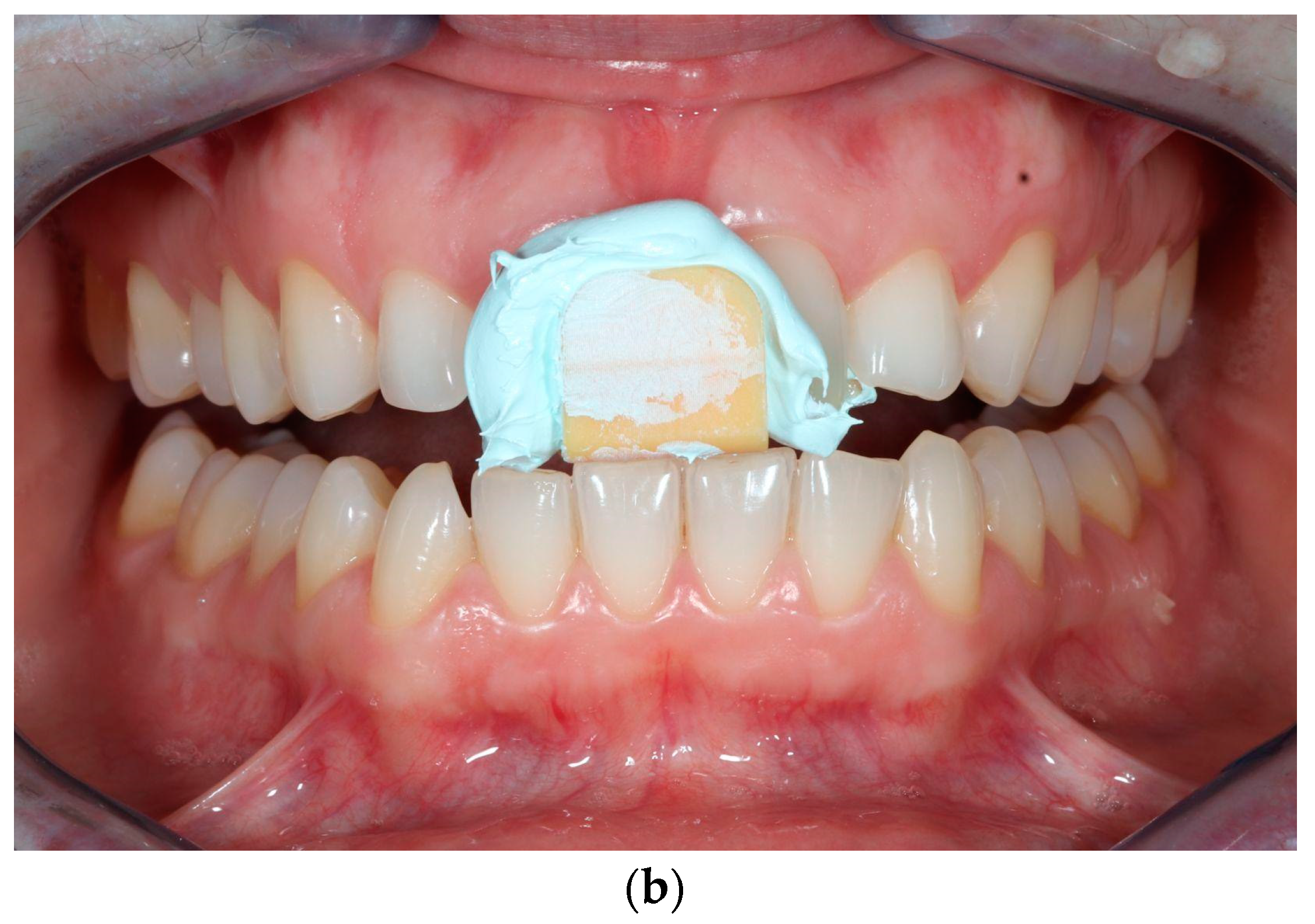
- Self-designed anterior flat plane deprogramming appliance (Lucia Jig);
- Zebris Ceramill Mind computer-aided design software (version: 4.2, Amman Girrbach, Pforzheim, Germany);
- NextDent 5100 (software version: 2.13 NextDent, Soesterberg, Netherlands);
- NextDent Ortho Rigid print resin (NextDent, Soesterberg, Netherlands).
2.2. Step by Step Workflow of the Fully Digital Process
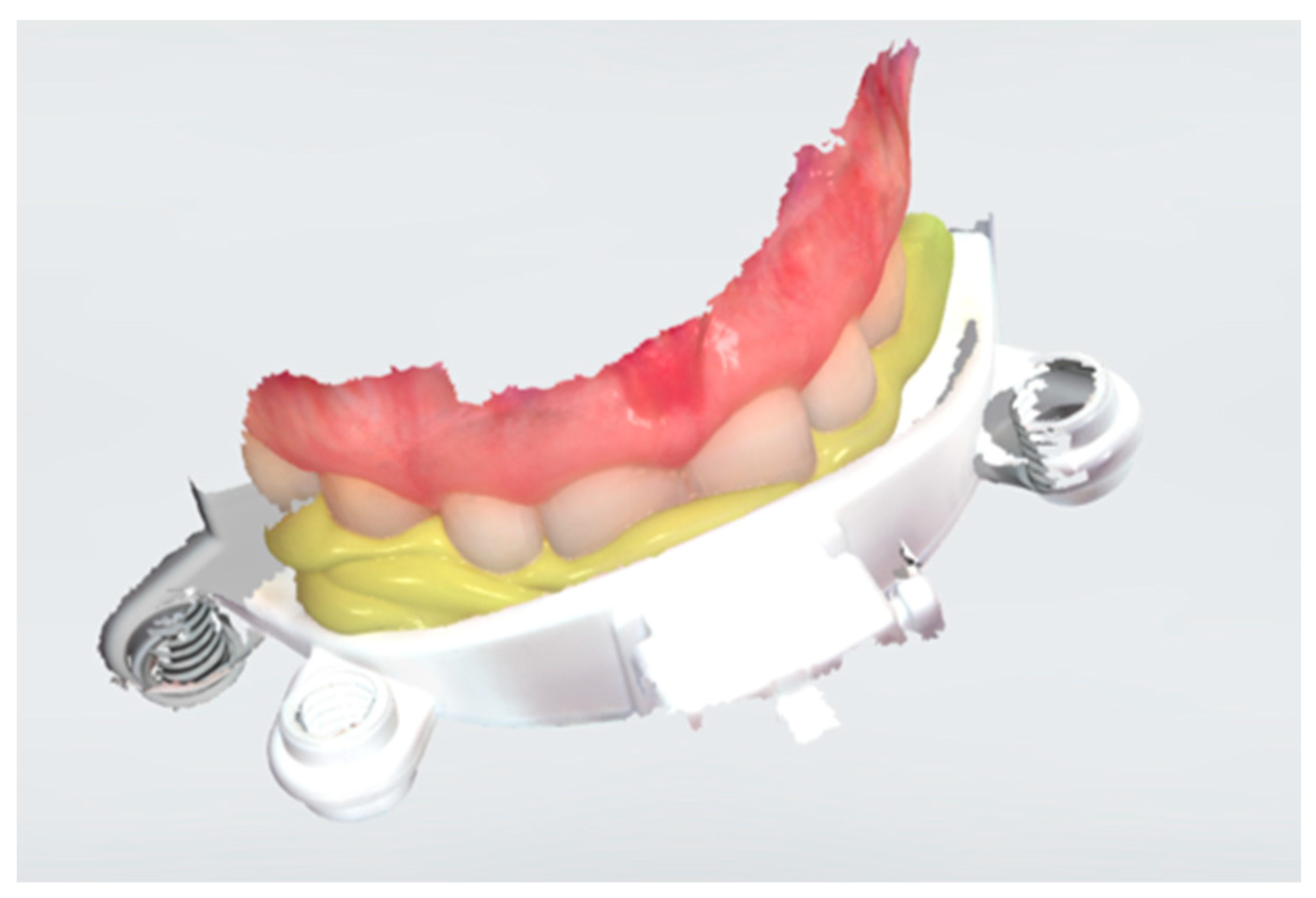
2.2.1. Registration Phase
2.2.2. Laboratory Phase
2.2.3. Delivery Phase
3. Results
3.1. Time
3.2. Measurement of CR and Individual Values
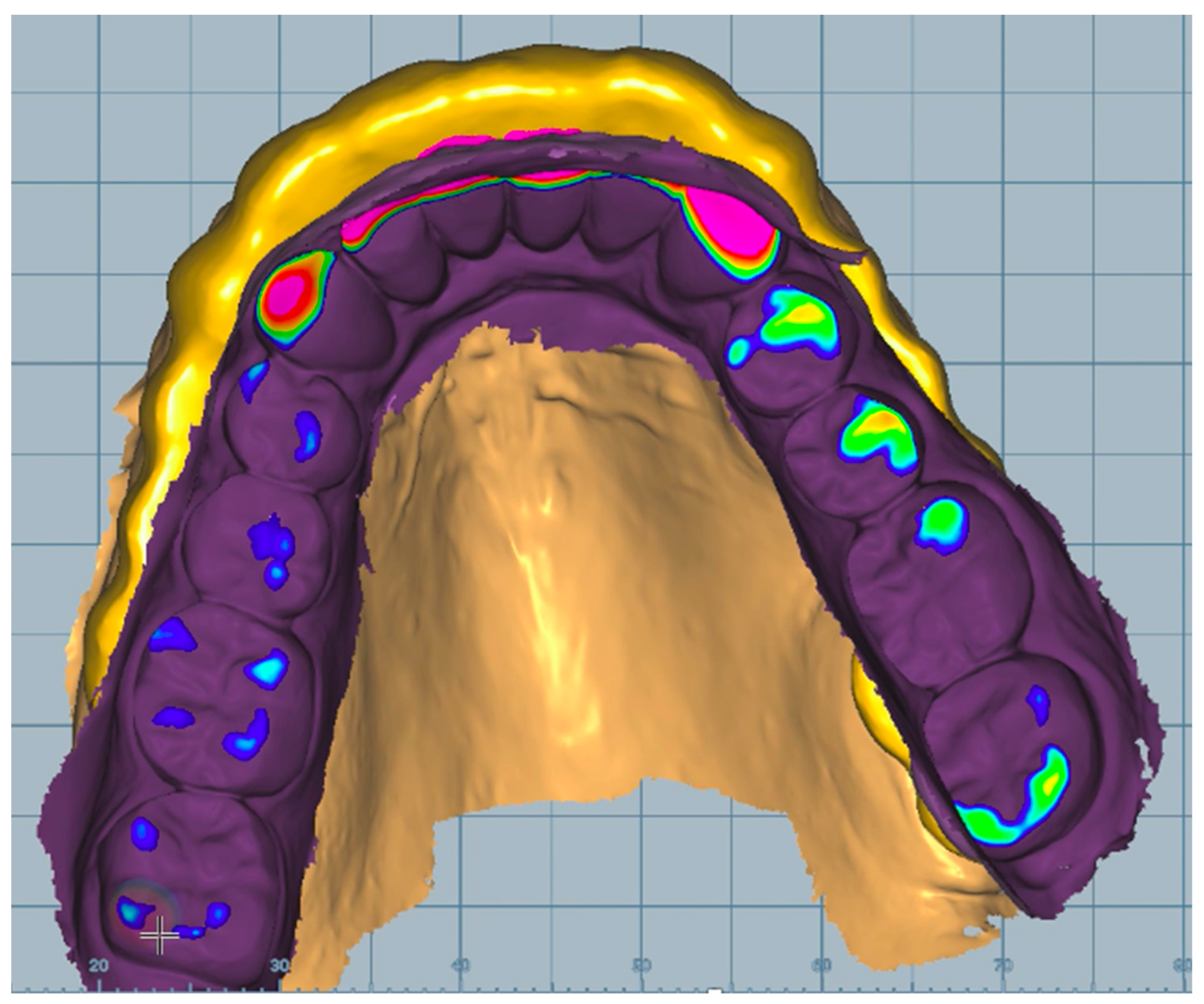
3.3. Planning
3.4. Three-dimensional Printing
3.5. Evaluation
3.6. Wearing Splint Experience
4. Discussion
4.1. Materials
4.2. Cost
4.3. Planning
4.4. Time
4.5. Sustainability
4.6. Wearing Splint Experience
4.7. Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santos, G.C., Jr.; Santos, M.J., Jr.; Rizkalla, A.S.; Madani, D.A.; El-Mowafy, O. Overview of CEREC CAD/CAM chairside system. Gen. Dent. 2013, 61, 36–40. [Google Scholar] [PubMed]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, G.; Nitsch, S.; Edelmayer, M.; Janjic, K.; Muller, A.S.; Agis, H. 3D Printing-Encompassing the Facets of Dentistry. Front. Bioeng. Biotechnol. 2018, 6, 172. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Chandran, J.; Balakrishnan, N.; Sreenivasagan, S. Awareness on three-dimensional printing of orthodontic appliances among dental students. J. Adv. Pharm. Technol. Res. 2022, 13, S563–S567. [Google Scholar]
- Alharbi, N.; Alharbi, S.; Cuijpers, V.; Osman, R.B.; Wismeijer, D. Three-dimensional evaluation of marginal and internal fit of 3D-printed interim restorations fabricated on different finish line designs. J. Prosthodont. Res. 2018, 62, 218–226. [Google Scholar] [CrossRef]
- Al-Khalifa, K.S.; Al-Swuailem, A.S.; AlSheikh, R.; Muazen, Y.Y.; Al-Khunein, Y.A.; Halawany, H.; Al-Abidi, K.S. The use of social media for professional purposes among dentists in Saudi Arabia. BMC Oral Health 2021, 21, 26. [Google Scholar] [CrossRef]
- Manfredini, D.; Lombardo, L.; Siciliani, G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: End of an era? J. Oral Rehabil. 2017, 44, 908–923. [Google Scholar] [CrossRef]
- Scrivani, S.J.; Keith, D.A.; Kaban, L.B. Temporomandibular Disorders. New Engl. J. Med. 2008, 359, 2693–2705. [Google Scholar] [CrossRef]
- Conti, P.C.; Pinto-Fiamengui, L.M.; Cunha, C.O.; Conti, A.C. Orofacial pain and temporomandibular disorders: The impact on oral health and quality of life. Braz. Oral Res. 2012, 26, 120–123. [Google Scholar] [CrossRef]
- Wadhwa, S.; Kapila, S. TMJ disorders: Future innovations in diagnostics and therapeutics. J. Dent. Educ. 2008, 72, 930–947. [Google Scholar] [CrossRef] [PubMed]
- Giannakopoulos, N.N.; Keller, L.; Rammelsberg, P.; Kronmuller, K.T.; Schmitter, M. Anxiety and depression in patients with chronic temporomandibular pain and in controls. J. Dent. 2010, 38, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Li, D.T.S.; Leung, Y.Y. Temporomandibular Disorders: Current Concepts and Controversies in Diagnosis and Management. Diagnostics 2021, 11, 459. [Google Scholar] [CrossRef]
- Ash, M.M., Jr.; Ramfjord, S.P. Reflections on the Michigan splint and other intraocclusal devices. J. Mich. Dent. Assoc. 1998, 80, 32–35. [Google Scholar] [PubMed]
- Kerstein, R.B. Reducing chronic masseter and temporalis muscular hyperactivity with computer-guided occlusal adjustments. Compend. Contin. Educ. Dent. 2010, 31, 530–534. [Google Scholar]
- Buduru, S.; Mesaros, A.; Talmaceanu, D.; Baru, O.; Ghiurca, R.; Cosgarea, R. Occlusion in the digital era: A report on 3 cases. Med. Pharm. Rep. 2019, 92, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Shopova, D.; Yordanova, M.; Yordanova, S. 3Shape Digital Design Software in Splints Creation—A Pilot Study. Eur J. Dent. 2021, 16, 815–819. [Google Scholar] [CrossRef]
- Kerstein, R.B. Current applications of computerized occlusal analysis in dental medicine. Gen. Dent. 2001, 49, 521–530. [Google Scholar]
- Ayuso-Montero, R.; Mariano-Hernandez, Y.; Khoury-Ribas, L.; Rovira-Lastra, B.; Willaert, E.; Martinez-Gomis, J. Reliability and Validity of T-scan and 3D Intraoral Scanning for Measuring the Occlusal Contact Area. J. Prosthodont. 2020, 29, 19–25. [Google Scholar] [CrossRef]
- Grymak, A.; Waddell, J.N.; Aarts, J.M.; Ma, S.; Choi, J.J.E. Evaluation of wear behaviour of various occlusal splint materials and manufacturing processes. J. Mech. Behav. Biomed. Mater. 2022, 126, 105053. [Google Scholar] [CrossRef]
- Reyes-Sevilla, M.; Kuijs, R.H.; Werner, A.; Kleverlaan, C.J.; Lobbezoo, F. Comparison of wear between occlusal splint materials and resin composite materials. J. Oral Rehabil. 2018, 45, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Shopova, D.; Bozhkova, T.; Yordanova, S.; Yordanova, M. Case Report: Digital analysis of occlusion with T-Scan Novus in occlusal splint treatment for a patient with bruxism. F1000Research 2022, 10, 915. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Zeitler, J.M.; Kois, D.E.; Kois, J.C. Utilizing an additively manufactured Kois deprogrammer to record centric relation: A simplified workflow and delivery technique. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.S.; Palinkas, M.; Regalo, S.C.; Sousa, L.G.; Siessere, S.; Semprini, M.; Bataglion, C. The effect of a Lucia jig for 30 minutes on neuromuscular re-programming, in normal subjects. Braz. Oral Res. 2012, 26, 530–535. [Google Scholar] [CrossRef]
- Salmi, M.; Paloheimo, K.-S.; Tuomi, J.; Ingman, T.; Mäkitie, A. A digital process for additive manufacturing of occlusal splints: A clinical pilot study. J. R. Soc. Interface 2013, 10, 20130203. [Google Scholar] [CrossRef]
- Karl, P.J.; Foley, T.F. The use of a deprogramming appliance to obtain centric relation records. Angle Orthod. 1999, 69, 117–124, discussion 24-5. [Google Scholar]
- Cameron, A.B.; Evans, J.L.; Abuzar, M.A.; Tadakamadla, S.K.; Love, R.M. Trueness assessment of additively manufactured maxillary complete denture bases produced at different orientations. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Revilla-León, M.; Özcan, M. Additive Manufacturing Technologies Used for Processing Polymers: Current Status and Potential Application in Prosthetic Dentistry. J. Prosthodontics 2019, 28, 146–158. [Google Scholar] [CrossRef]
- Loumprinis, N.; Maier, E.; Belli, R.; Petschelt, A.; Eliades, G.; Lohbauer, U. Viscosity and stickiness of dental resin composites at elevated temperatures. Dent. Mater. 2021, 37, 413–422. [Google Scholar] [CrossRef]
- Bürgers, R.; Schubert, A.; Müller, J.; Krohn, S.; Rödiger, M.; Leha, A.; Wassmann, T. Cytotoxicity of 3D-printed, milled, and conventional oral splint resins to L929 cells and human gingival fibroblasts. Clin. Exp. Dent. Res. 2022, 8, 650–657. [Google Scholar] [CrossRef]
- Xu, Y.; Xepapadeas, A.B.; Koos, B.; Geis-Gerstorfer, J.; Li, P.; Spintzyk, S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent. Mater. 2021, 37, e314–e327. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Cascos-Sánchez, R.; Zeitler, J.M.; Barmak, A.B.; Kois, J.C.; Gómez-Polo, M. Influence of print orientation and wet-dry storage time on the intaglio accuracy of additively manufactured occlusal devices. J. Prosthet. Dent. 2023. [Google Scholar] [CrossRef]
- Róth, I.; Czigola, A.; Joós-Kovács, G.L.; Dalos, M.; Hermann, P.; Borbély, J. Learning curve of digital intraoral scanning—An in vivo study. BMC Oral Health 2020, 20, 287. [Google Scholar] [CrossRef]
- Hegedus, T.; Kreuter, P.; Kismarczi-Antalffy, A.A.; Demeter, T.; Banyai, D.; Vegh, A.; Géczi, Z.; Hermann, P.; Payer, M.; Zsembery, Á.; et al. User Experience and Sustainability of 3D Printing in Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 1921. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somogyi, A.; Végh, D.; Róth, I.; Hegedüs, T.; Schmidt, P.; Hermann, P.; Géczi, Z. Therapy for Temporomandibular Disorders: 3D-Printed Splints from Planning to Evaluation. Dent. J. 2023, 11, 126. https://doi.org/10.3390/dj11050126
Somogyi A, Végh D, Róth I, Hegedüs T, Schmidt P, Hermann P, Géczi Z. Therapy for Temporomandibular Disorders: 3D-Printed Splints from Planning to Evaluation. Dentistry Journal. 2023; 11(5):126. https://doi.org/10.3390/dj11050126
Chicago/Turabian StyleSomogyi, Andrea, Dániel Végh, Ivett Róth, Tamás Hegedüs, Péter Schmidt, Péter Hermann, and Zoltán Géczi. 2023. "Therapy for Temporomandibular Disorders: 3D-Printed Splints from Planning to Evaluation" Dentistry Journal 11, no. 5: 126. https://doi.org/10.3390/dj11050126
APA StyleSomogyi, A., Végh, D., Róth, I., Hegedüs, T., Schmidt, P., Hermann, P., & Géczi, Z. (2023). Therapy for Temporomandibular Disorders: 3D-Printed Splints from Planning to Evaluation. Dentistry Journal, 11(5), 126. https://doi.org/10.3390/dj11050126