Distributed Manufacturing of Open Source Medical Hardware for Pandemics


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Ventilators
3.2. Alcohol-Based Hand-Rub
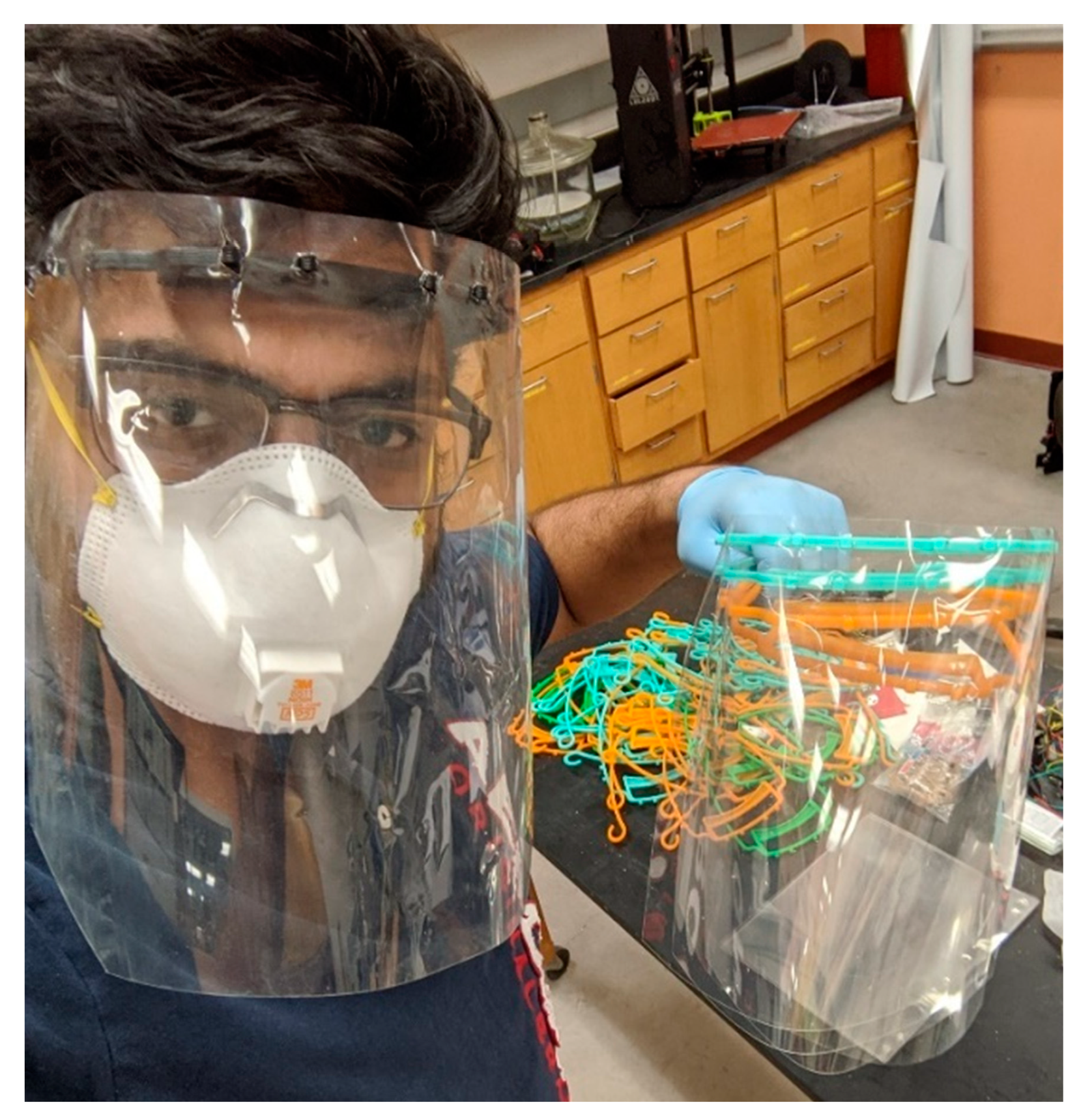
3.3. Face Shield (Eye, Nose, and Mouth Protection)
3.4. N95 Masks
3.5. Latex Single-Use Gloves (Clinical)
3.6. Reusable Vinyl/Rubber Gloves (Cleaning)
3.7. Eye Protection (Visor/Goggles)
3.8. Protective Gowns/Aprons
3.9. Disposable Thermometers
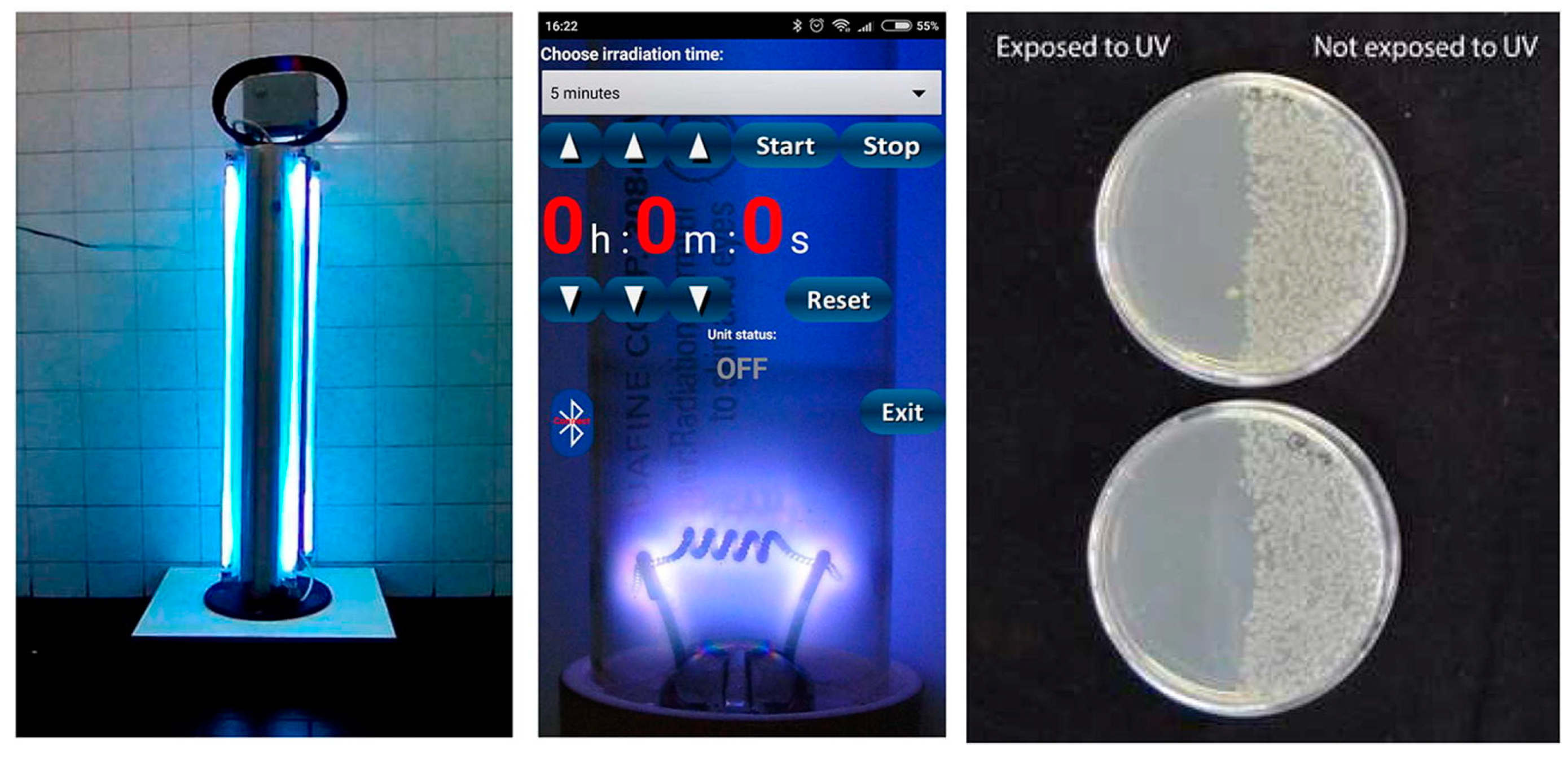
3.10. UV Tube Light for Sterilization
3.11. Medical Masks (Surgical/Procedure)
3.12. Detergent/Disinfectant
3.13. Single-Use Towels
3.14. Biohazard Bags
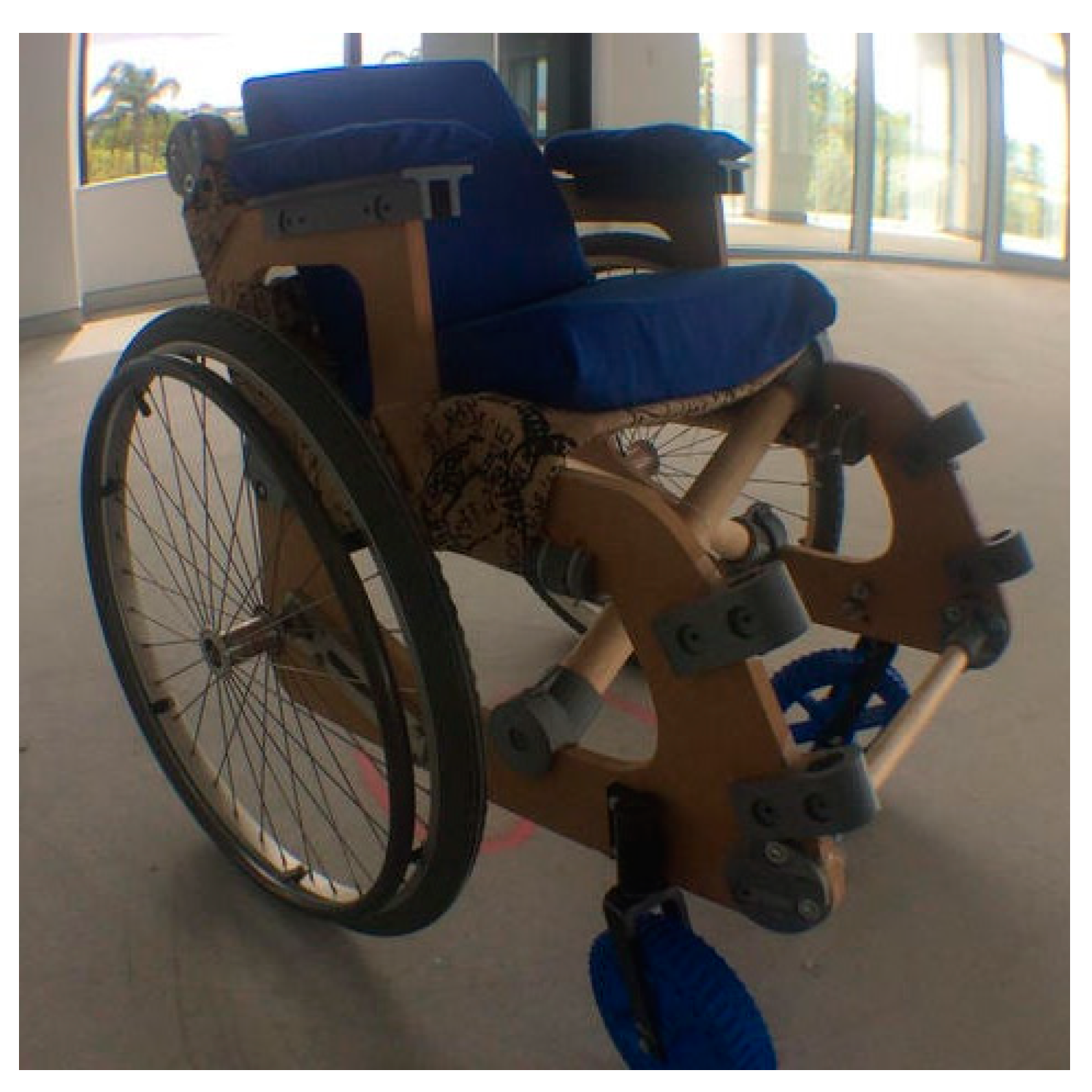
3.15. Wheelchair
3.16. Glucometer with Strips
3.17. Medicine
3.18. IV Fluid-DNS
3.19. IV Fluid-Dextrose
3.20. Hard-Frozen Gel Packs
3.21. Summary of Results
4. Discussion
4.1. Diversity of Solutions Needed
4.2. Protecting Laboratories, MakerSpaces, and Fabrication Facilities During ‘Shelter in Place’
4.3. Streamline Regulatory Processes
4.4. Development of a Good-Samaritan Law for Protection of Makers and Designers of Open Source Medical Hardware
4.5. Require All Citizen Funded Research Be Released Freely under Open Source Licenses
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Itzwerth, R.L.; MacIntyre, C.R.; Shah, S.; Plant, A.J. Pandemic influenza and critical infrastructure dependencies: Possible impact on hospitals. Med. J. Aust. 2006, 185, S70–S72. [Google Scholar] [CrossRef] [PubMed]
- Fair, J.M.; LeClaire, R.J.; Wilson, M.L.; Turk, A.L.; DeLand, S.M.; Powell, D.R.; Klare, P.C.; Ewers, M.; Dauelsberg, L.; Izraelevitz, D. An Integrated Simulation of Pandemic Influenza Evolution, Mitigation and Infrastructure Response. In Proceedings of the 2007 IEEE Conference on Technologies for Homeland Security, Woburn, MA, USA, 16–17 May 2007; pp. 240–245. [Google Scholar]
- Williams, V.J. Fluconomics: Preserving our hospital infrastructure during and after a pandemic. Yale J. Health Policy Law Ethics 2007, 7, 99. [Google Scholar]
- Adini, B.; Goldberg, A.; Cohen, R.; Bar-Dayan, Y. Relationship between equipment and infrastructure for pandemic influenza and performance in an avian flu drill. Emerg. Med. J. 2009, 26, 786–790. [Google Scholar] [CrossRef] [PubMed]
- Homeland Security Council. National Strategy for Pandemic Influenza; Homeland Security Council: Washington, DC, USA, 2005.
- World Health Organization Critical Preparedness, Readiness and Response Actions for COVID-19. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/critical-preparedness-readiness-and-response-actions-for-covid-19 (accessed on 31 March 2020).
- Lancet, T. COVID-19: Too little, too late? Lancet 2020, 395, 755. [Google Scholar] [CrossRef]
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.-Y.; D’Ortenzio, E.; Yazdanpanah, Y.; Eholie, S.P.; Altmann, M.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, P.S. Shamika Ravi, and Sikim COVID-19 | Is India’s Health Infrastructure Equipped to Handle an Epidemic? Brookings 2020. Available online: https://www.brookings.edu/blog/up-front/2020/03/24/is-indias-health-infrastructure-equipped-to-handle-an-epidemic/ (accessed on 31 March 2020).
- CDC Coronavirus Disease 2019 (COVID-19) Situation Summary. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/summary.html (accessed on 31 March 2020).
- Ramsey, L. Hospitals Could be Overwhelmed with Patients and Run out of Beds and Ventilators as the Coronavirus Pushes the US Healthcare System to Its Limits. Available online: https://www.businessinsider.com/coronavirus-intensive-care-unit-shortages-of-ventilators-staff-space-2020-3 (accessed on 31 March 2020).
- Armour, M.E. Hospital Capacity Crosses Tipping Point in U.S. Coronavirus Hot Spots. Wall Str. J. 2020. Available online: https://www.wsj.com/articles/hospital-capacity-crosses-tipping-point-in-u-s-coronavirus-hot-spots-11585215006 (accessed on 31 March 2020).
- Choe, S.; Hinnant, L.; Press, T.S.A. Comments, 6:40 pm Email to a Friend Share on Facebook Share on TwitterPrint This Article View Italian Hospitals Overwhelmed by Deaths Amid Coronavirus Outbreak—The Boston Globe. Available online: https://www.bostonglobe.com/2020/03/12/nation/italian-hospitals-overwhelmed-by-deaths-amid-coronavirus-outbreak/ (accessed on 31 March 2020).
- Tondo, L. Italian Hospitals Short of Beds as Coronavirus Death Toll Jumps. The Guardian 2020. Available online: https://www.theguardian.com/world/2020/mar/09/italian-hospitals-short-beds-coronavirus-death-toll-jumps (accessed on 31 March 2020).
- Van Beusekom, M. 2020 Doctors: COVID-19 Pushing Italian ICUs Toward Collapse. Available online: http://www.cidrap.umn.edu/news-perspective/2020/03/doctors-covid-19-pushing-italian-icus-toward-collapse (accessed on 31 March 2020).
- Jennings, L.C.; Monto, A.S.; Chan, P.K.-S.; Szucs, T.D.; Nicholson, K.G. Stockpiling prepandemic influenza vaccines: A new cornerstone of pandemic preparedness plans. Lancet Infect. Dis. 2008, 8, 650–658. [Google Scholar] [CrossRef]
- Hashikura, M.; Kizu, J. Stockpile of personal protective equipment in hospital settings: Preparedness for influenza pandemics. Am. J. Infect. Control. 2009, 37, 703–707. [Google Scholar] [CrossRef]
- Radonovich, L.J.; Magalian, P.D.; Hollingsworth, M.K.; Baracco, G. Stockpiling Supplies for the Next Influenza Pandemic. Emerg. Infect. Dis. 2009, 15, e1. [Google Scholar] [CrossRef]
- Dimitrov, N.B.; Goll, S.; Hupert, N.; Pourbohloul, B.; Meyers, L.A. Optimizing Tactics for Use of the U.S. Antiviral Strategic National Stockpile for Pandemic Influenza. PLoS ONE 2011, 6. [Google Scholar] [CrossRef]
- Einav, S.; Hick, J.L.; Hanfling, D.; Erstad, B.L.; Toner, E.S.; Branson, R.D.; Kanter, R.K.; Kissoon, N.; Dichter, J.R.; Devereaux, A.V.; et al. Surge Capacity Logistics. Chest 2014, 146, e17–e43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramovich, M.N.; Hershey, J.C.; Callies, B.; Adalja, A.A.; Tosh, P.K.; Toner, E.S. Hospital influenza pandemic stockpiling needs: A computer simulation. Am. J. Infect. Control. 2017, 45, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-C.; Araz, O.M.; Morton, D.P.; Johnson, G.P.; Damien, P.; Clements, B.; Meyers, L.A. Stockpiling Ventilators for Influenza Pandemics. Emerg. Infect. Dis. 2017, 23, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Else, D.H. Defense Production Act: Purpose and Scope; Library of Congress Washington DC Congressional Reaearch Service: Washington, DC, USA, 2009.
- Scanlan, A.L. The Defense Production Act of 1950. Rutgers Law Rev. 1950, 5, 518. [Google Scholar]
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical Supply Shortages—The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Freyer-Biggs, Z. The Government’s Secret Ventilator Stockpile Is Nowhere Near Enough to Fight the Coronavirus. Available online: https://publicintegrity.org/health/coronavirus-and-inequality/the-governments-secret-ventilator-stockpile-is-nowhere-near-enough-to-fight-the-coronavirus/ (accessed on 31 March 2020).
- Scher, I. The US Government Has a Stockpile of 16,000 Extra Ventilators in Case of an Emergency Like COVID-19. It Isn’t Enough. Available online: https://www.businessinsider.com/us-government-ventilator-stockpile-too-small-coronavirus-2020-3 (accessed on 31 March 2020).
- Greenfiled Boyce, N. Why Even a Huge Medical Stockpile Will Be of Limited Use Against COVID-19. Available online: https://www.npr.org/sections/health-shots/2020/03/14/814121891/why-even-a-huge-medical-stockpile-will-be-of-limited-use-against-covid-19 (accessed on 31 March 2020).
- Siddiqui, M.R.; Edmunds, W.J. Cost-effectiveness of Antiviral Stockpiling and Near-Patient Testing for Potential Influenza Pandemic. Emerg. Infect. Dis. 2008, 14, 267–274. [Google Scholar] [CrossRef]
- Balicer, R.D.; Huerta, M.; Davidovitch, N.; Grotto, I. Cost-Benefit of Stockpiling Drugs for Influenza Pandemic. Emerg. Infect. Dis. 2005, 11, 1280–1282. [Google Scholar] [CrossRef]
- Boldrin, M.; Levine, D. AER (92,2) p. 209-The Case Against Intellectual Property. Am. Econ. Rev. 2002, 92, 209–212. [Google Scholar] [CrossRef]
- Boldrin, M.; Levine, D.K. 2003 Lawrence R. Klein Lecture the Case Against Intellectual Monopoly*. Int. Econ. Rev. 2004, 45, 327–350. [Google Scholar] [CrossRef]
- Pagano, U. The crisis of intellectual monopoly capitalism. Camb. J. Econ. 2014, 38, 1409–1429. [Google Scholar] [CrossRef] [Green Version]
- Durand, C.; Milberg, W. Intellectual monopoly in global value chains. Rev. Int. Polit. Econ. 2019, 27, 404–429. [Google Scholar] [CrossRef] [Green Version]
- Martin, G.; Sorenson, C.; Faunce, T. Balancing intellectual monopoly privileges and the need for essential medicines. Glob. Health 2007, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Stiglitz, J.E.; Jayadev, A. Medicine for tomorrow: Some alternative proposals to promote socially beneficial research and development in pharmaceuticals. J. Generic Med. Bus. J. Generic Med. Sect. 2010, 7, 217–226. [Google Scholar] [CrossRef] [Green Version]
- 3D printed face shields for medics and professionals. Prusa3D-3D Print. Josef Průša. Available online: https://www.prusa3d.com/covid19/ (accessed on 31 March 2020).
- Masnick, M. SoftBank Owned Patent Troll, Using Monkey Selfie Law Firm, Sues to Block Covid-19 Testing, Using Theranos Patents. Available online: https://www.techdirt.com/articles/20200316/14584244111/softbank-owned-patent-troll-using-monkey-selfie-law-firm-sues-to-block-covid-19-testing-using-theranos-patents.shtml (accessed on 31 March 2020).
- Morrison, S. Trump Isn’t Making America’s Ventilator Shortage Any Easier. Available online: https://www.vox.com/recode/2020/3/20/21186749/ventilators-coronavirus-covid-19-elon-musk (accessed on 31 March 2020).
- Temple, J. We Need More Ventilators. Here’s What It Will Take to Get Them. Available online: https://www.technologyreview.com/s/615380/we-need-more-ventilators-heres-what-it-will-take-to-get-them/ (accessed on 31 March 2020).
- World Trade Organization COVID-19 and World Trade. Available online: https://www.wto.org/english/tratop_e/covid19_e/covid19_e.htm (accessed on 31 March 2020).
- Tong, S. Countries Race to Limit or Ban Mask and Ventilator Exports. Marketplace 2020. Available online: https://www.marketplace.org/2020/03/30/countries-race-to-limit-ban-exports-of-masks-ventilators-other-gear/ (accessed on 31 March 2020).
- Farrell, H.; Newman, A.L. Harvard Business Review; 2020. Available online: https://hbr.org/2020/03/will-governments-restrict-foreign-access-to-pandemic-supplies (accessed on 31 March 2020).
- Evenett, S. Sickening thy neighbour: Export Restraints on Medical Supplies during a Pandemic. 2020. Available online: https://voxeu.org/article/export-restraints-medical-supplies-during-pandemic (accessed on 31 March 2020).
- Wagtendonk, A. The Government is Distributing Emergency Covid-19 Supplies. But Some States Are Losing Out. Available online: https://www.vox.com/policy-and-politics/2020/3/29/21198704/emergency-covid-19-supplies-fema-states-federal-government (accessed on 31 March 2020).
- Srai, J.S.; Kumar, M.; Graham, G.; Phillips, W.; Tooze, J.; Ford, S.; Beecher, P.; Raj, B.; Gregory, M.; Tiwari, M.K.; et al. Distributed manufacturing: Scope, challenges and opportunities. Int. J. Prod. Res. 2016, 54, 1–19. [Google Scholar] [CrossRef]
- Helo, P.; Suorsa, M.; Hao, Y.; Anussornnitisarn, P. Toward a cloud-based manufacturing execution system for distributed manufacturing. Comput. Ind. 2014, 65, 646–656. [Google Scholar] [CrossRef]
- Laplume, A.; Anzalone, G.C.; Pearce, J.M. Open-source, self-replicating 3-D printer factory for small-business manufacturing. Int. J. Adv. Manuf. Technol. 2015, 85, 633–642. [Google Scholar] [CrossRef] [Green Version]
- Sells, E.; Bailard, S.; Smith, Z.; Bowyer, A.; Olliver, V.; Piller, F.T.; Tseng, M.M. RepRap: The Replicating Rapid Prototyper: Maximizing Customizability by Breeding the Means of Production. In Handbook of Research in Mass Customization and Personalization; World Scientific Pub Co Pte Lt: Singapore, 2009; pp. 568–580. [Google Scholar]
- Jones, R.; Haufe, P.; Sells, E.; Iravani, P.; Olliver, V.; Palmer, C.; Bowyer, A. RepRap—The replicating rapid prototyper. Robotica 2011, 29, 177–191. [Google Scholar] [CrossRef] [Green Version]
- Campbell, I.; Diegel, O.; Kowen, J.; Wohlers, T. Wohlers Report 2018: 3D Printing and Additive Manufacturing State of the Industry: Annual Worldwide Progress Report; Wohlers Associates: Fort Collins, CO, USA, 2018; ISBN 978-0-9913332-4-0. [Google Scholar]
- O Laplume, A.; Petersen, B.; Pearce, J.M. Global value chains from a 3D printing perspective. J. Int. Bus. Stud. 2016, 47, 595–609. [Google Scholar] [CrossRef]
- Böhme, T.; Birtchnell, T. 3DP and the Domestication of Supply Chains in the Future. In Managing 3D Printing; Springer Science and Business Media LLC: Berlin, Germany, 2020; pp. 179–190. [Google Scholar]
- Pearce, J.M.; Blair, C.M.; Laciak, K.J.; Andrews, R.; Nosrat, A.; Zelenika-Zovko, I. 3-D Printing of Open Source Appropriate Technologies for Self-Directed Sustainable Development. J. Sustain. Dev. 2010, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Devor, R.E.; Kapoor, S.G.; Cao, J.; Ehmann, K. Transforming the Landscape of Manufacturing: Distributed Manufacturing Based on Desktop Manufacturing (DM)2. J. Manuf. Sci. Eng. 2012, 134, 041004. [Google Scholar] [CrossRef]
- King, D.L.; Babasola, A.; Rozario, J.; Pearce, J.M. Mobile Open-Source Solar-Powered 3-D Printers for Distributed Manufacturing in Off-Grid Communities. Chall. Sustain. 2014, 2, 18–27. [Google Scholar] [CrossRef]
- Gwamuri, J.; Wittbrodt, B.T.; Anzalone, N.C.; Pearce, J.M. Reversing the Trend of Large Scale and Centralization in Manufacturing: The Case of Distributed Manufacturing of Customizable 3-D-Printable Self-Adjustable Glasses. Chall. Sustain. 2014, 2, 30–40. [Google Scholar] [CrossRef]
- Wittbrodt, B.; Laureto, J.; Tymrak, B.; Pearce, J.M. Distributed manufacturing with 3-D printing: A case study of recreational vehicle solar photovoltaic mounting systems. J. Frugal Innov. 2015, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Petersen, E.E.; Pearce, J.M. Emergence of Home Manufacturing in the Developed World: Return on Investment for Open-Source 3-D Printers. Technology 2017, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Woern, A.L.; Pearce, J.M. Distributed Manufacturing of Flexible Products: Technical Feasibility and Economic Viability. Technology 2017, 5, 71. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Hong, C.; Lin, J.; Jin, X.; Xu, W. Make it swing: Fabricating personalized roly-poly toys. Comput. Aided Geom. Des. 2016, 43, 226–236. [Google Scholar] [CrossRef]
- Petersen, E.E.; Kidd, R.W.; Pearce, J.M. Impact of DIY Home Manufacturing with 3D Printing on the Toy and Game Market. Technology 2017, 5, 45. [Google Scholar] [CrossRef]
- Song, P.; Wang, X.; Tang, X.; Fu, C.-W.; Xu, H.; Liu, L.; Mitra, N.J. Computational design of wind-up toys. ACM Trans. Graph. 2017, 36, 1–13. [Google Scholar] [CrossRef]
- Pearce, J.M. Building Research Equipment with Free, Open-Source Hardware. Science 2012, 337, 1303–1304. [Google Scholar] [CrossRef]
- Daniel, K.F.; Peter, J.G. Open-Source Hardware Is a Low-Cost Alternative for Scientific Instrumentation and Research. Mod. Instrum. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.M. Open-Source Lab: How to Build Your Own Hardware and Reduce Research Costs; Elsevier: Amsterdam, The Netherlands, 2013; ISBN 978-0-12-410486-0. [Google Scholar]
- Pearce, J.M. Cut costs with open-source hardware. Nature 2014, 505, 618. [Google Scholar] [CrossRef] [Green Version]
- Damase, T.R.; Stephens, D.; Spencer, A.; Allen, P.B. Open source and DIY hardware for DNA nanotechnology labs. J. Boil. Methods 2015, 2, e24. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Wijnen, B.; Pearce, J.M. Open-Source 3-D Platform for Low-Cost Scientific Instrument Ecosystem. J. Lab. Autom. 2016, 21, 517–525. [Google Scholar] [CrossRef] [Green Version]
- Coakley, M.; Hurt, D. 3D Printing in the Laboratory. J. Lab. Autom. 2016, 21, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Dryden, M.D.M.; Fobel, R.; Fobel, C.; Wheeler, A.R. Upon the Shoulders of Giants: Open-Source Hardware and Software in Analytical Chemistry. Anal. Chem. 2017, 89, 4330–4338. [Google Scholar] [CrossRef] [Green Version]
- Gwamuri, J.; Gwamuri, J.; Pearce, J.M.; Pearce, J.M. Open Source 3-D Printers: An Appropriate Technology for Building Low Cost Optics Labs for the Developing Communities. In Proceedings of the ETOP 2017 Proceedings (2017), Hangzhou, China, 29–31 May 2017; p. 104522S. [Google Scholar]
- Kera, D. Science Artisans and Open Science Hardware. Bull. Sci. Technol. Soc. 2017, 37, 97–111. [Google Scholar] [CrossRef]
- Chagas, A.M. Haves and have nots must find a better way: The case for open scientific hardware. PLoS Boil. 2018, 16, e3000014. [Google Scholar] [CrossRef] [Green Version]
- Gibb, A.; Abadie, S. Building Open Source Hardware: DIY Manufacturing for Hackers and Makers; Pearson Education: London, UK, 2014; ISBN 978-0-321-90604-5. [Google Scholar]
- Nilsiam, Y.; Pearce, J.M. Free and Open Source 3-D Model Customizer for Websites to Democratize Design with OpenSCAD. Designs 2017, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Oberloier, S.; Pearce, J.M. General Design Procedure for Free and Open-Source Hardware for Scientific Equipment. Designs 2017, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Wittbrodt, B.; Glover, A.; Laureto, J.; Anzalone, G.; Oppliger, D.; Irwin, J.; Pearce, J.M. Life-cycle economic analysis of distributed manufacturing with open-source 3-D printers. Mechatronics 2013, 23, 713–726. [Google Scholar] [CrossRef] [Green Version]
- Tatham, P.; Loy, J.; Peretti, U. Three dimensional printing—A key tool for the humanitarian logistician? J. Humanit. Logist. Supply Chain Manag. 2015, 5, 188–208. [Google Scholar] [CrossRef] [Green Version]
- Saripalle, S.; Maker, H.; Bush, A.; Lundman, N. 3D printing for disaster preparedness: Making life-saving supplies on-site, on-demand, on-time. In Proceedings of the 2016 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 29 October–1 November 2016; pp. 205–208. [Google Scholar]
- Savonen, B.L.; Mahan, T.; Curtis, M.W.; Schreier, J.W.; Gershenson, J.K.; Pearce, J.M. Development of a Resilient 3-D Printer for Humanitarian Crisis Response. Technology 2018, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Kats, D.; Spicher, L.; Savonen, B.; Gershenson, J. Paper 3D Printing to Supplement Rural Healthcare Supplies—What Do Healthcare Facilities Want? In Proceedings of the 2018 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 17–20 October 2018; pp. 1–8. [Google Scholar]
- DelCore, A.; Herrera, A. Sustainable solar headlamp: An open source consumer medical device. In Proceedings of the 2015 IEEE International Conference on Consumer Electronics (ICCE), Berlin, Germany, 6–9 September 2015; pp. 395–397. [Google Scholar]
- Purdon, P.L.; Millan, H.; Fuller, P.L.; Bonmassar, G. An open-source hardware and software system for acquisition and real-time processing of electrophysiology during high field MRI. J. Neurosci. Methods 2008, 175, 165–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferretti, J.; Di Pietro, L.; De Maria, C. Open-source automated external defibrillator. HardwareX 2017, 2, 61–70. [Google Scholar] [CrossRef]
- Bravo-Martinez, J. Open source automated western blot processor. HardwareX 2019, 6, e00088. [Google Scholar] [CrossRef]
- Rotermund, D.; Ernst, U.A.; Pawelzik, K.R. Open Hardware for neuro-prosthesis research: A study about a closed-loop multi-channel system for electrical surface stimulations and measurements. HardwareX 2019, 6, e00078. [Google Scholar] [CrossRef]
- Lund, J.; Paris, A.; Brock, J. Mouthguard-based wireless high-bandwidth helmet-mounted inertial measurement system. HardwareX 2018, 4, e00041. [Google Scholar] [CrossRef]
- E Michaels, R.; Pearce, J.M. 3-D printing open-source click-MUAC bands for identification of malnutrition. Public Health Nutr. 2017, 20, 2063–2066. [Google Scholar] [CrossRef] [Green Version]
- Newman, J.P.; Zeller-Townson, R.; Fong, M.-F.; Desai, S.A.; Gross, R.E.; Potter, S.M. Closed-Loop, Multichannel Experimentation Using the Open-Source NeuroRighter Electrophysiology Platform. Front. Neural Circuits 2013, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Blomqvist, K.H.; Sepponen, R.E.; Lundbom, N.; Lundbom, J. An open-source hardware for electrical bioimpedance measurement. In Proceedings of the 2012 13th Biennial Baltic Electronics Conference, Tallinn, Estonia, 3–5 October 2012; pp. 199–202. [Google Scholar]
- Rolston, J.D.; Gross, R.E.; Potter, S.M. Closed-Loop, Open-Source Electrophysiology. Front. Mol. Neurosci. 2010, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Niezen, G.; Eslambolchilar, P.; Thimbleby, H. Open-source hardware for medical devices. BMJ Innov. 2016, 2, 78–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, J. Maximizing returns for public funding of medical research with open-source hardware. Health Policy Technol. 2017, 6, 381–382. [Google Scholar] [CrossRef] [Green Version]
- Chavez, A.; Kovarik, C. Open Source Technology for Medical Practice in Developing Countries. Available online: www.igi-global.com/chapter/open-source-technology-for-medical-practice-in-developing-countries/209161 (accessed on 31 March 2020).
- Winter, L.; Pellicer-Guridi, R.; Broche, L.; Winkler, S.A.; Reimann, H.M.; Han, H.; Arndt, F.; Hodge, R.; Günyar, S.; Moritz, M.; et al. Open Source Medical Devices for Innovation, Education and Global Health: Case Study of Open Source Magnetic Resonance Imaging. In New Horizons in Positive Leadership and Change; Springer Science and Business Media LLC: Berlin, Germany, 2018; pp. 147–163. [Google Scholar]
- Pearce, J.M. Maximizar la rentabilidad de la inversión para la salud pública con hardware médico de código abierto. Gac. Sanit. 2015, 29, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, J.M. Quantifying the Value of Open Source Hard-ware Development. Mod. Econ. 2015, 6, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.M. Emerging Business Models for Open Source Hardware. J. Open Hardw. 2017, 1, 84. [Google Scholar] [CrossRef] [Green Version]
- Chagas, A.M.; Molloy, J.C.; Prieto-Godino, L.L.; Baden, T. Leveraging open hardware to alleviate the burden of COVID-19 on global health systems. PLoS Boil. 2020, 18, e3000730. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Micro, Small and Medium Enterprises, Government of India. Manufacturing or Supply of Following Items Related to Use in COVID-19. Available online: http://jan-sampark.nic.in/campaigns/2020/26-Mar/MSME/index.html (accessed on 31 March 2020).
- OSHWA Definition (English). Available online: https://www.oshwa.org/definition/ (accessed on 31 March 2020).
- CERN Home Wiki Projects/CERN Open Hardware Licence. Available online: https://ohwr.org/project/cernohl/wikis/home (accessed on 31 March 2020).
- TAPR The TAPR Open Hardware License—TAPR. Available online: https://tapr.org/the-tapr-open-hardware-license/ (accessed on 31 March 2020).
- Free Software Foundation GNU General Public License. Available online: https://www.gnu.org/licenses/gpl-3.0.en.html (accessed on 31 March 2020).
- Creative Commons Creative Commons—Attribution-ShareAlike 3.0 United States—CC BY-SA 3.0 US. Available online: https://creativecommons.org/licenses/by-sa/3.0/us/ (accessed on 31 March 2020).
- OSI Licenses & Standards|Open Source Initiative. Available online: https://opensource.org/licenses (accessed on 31 March 2020).
- Sanchez, F.A.C.; Lanza, S.; Boudaoud, H.; Hoppe, S.; Camargo, M. Polymer Recycling and Additive Manufacturing in an Open Source Context: Optimization of Processes and Methods. In Proceedings of the Annual International Solid Freeform Fabrication Symposium, Austin, TX, USA, 10–12 August 2015; p. 1591. [Google Scholar]
- Cruz Sanchez, F.A.; Boudaoud, H.; Hoppe, S.; Camargo, M. The green Fablab concept: A local and distributed recycling approach for open source additive manufacturing. In Proceedings of the 2nd Journée de l’innovation Abbé Grégoire (JAG), Paris, France, 28 March 2017. [Google Scholar]
- Zhong, S.; Pearce, J.M. Tightening the loop on the circular economy: Coupled distributed recycling and manufacturing with recyclebot and RepRap 3-D printing. Resour. Conserv. Recycl. 2018, 128, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Pavlo, S.; Fabio, C.; Hakim, B.; Mauricio, C. 3D-Printing Based Distributed Plastic Recycling: A Conceptual Model for Closed-Loop Supply Chain Design. In Proceedings of the 2018 IEEE International Conference on Engineering, Technology and Innovation (ICE/ITMC), Stuttgart, Germany,, 17–20 June 2018; pp. 1–8. [Google Scholar]
- Byard, D.J.; Woern, A.L.; Oakley, R.B.; Fiedler, M.J.; Snabes, S.L.; Pearce, J.M. Green fab lab applications of large-area waste polymer-based additive manufacturing. Addit. Manuf. 2019, 27, 515–525. [Google Scholar] [CrossRef] [Green Version]
- Dertinger, S.C.; Gallup, N.; Tanikella, N.G.; Grasso, M.; Vahid, S.; Foot, P.J.S.; Pearce, J.M. Technical pathways for distributed recycling of polymer composites for distributed manufacturing: Windshield wiper blades. Resour. Conserv. Recycl. 2020, 157, 104810. [Google Scholar] [CrossRef]
- Ravindran, A.; Scsavnicki, S.; Nelson, W.; Gorecki, P.; Franz, J.; Oberloier, S.; Meyer, T.; Barnard, A.; Pearce, J.M. Open Source Waste Plastic Granulator. Technology 2019, 7, 74. [Google Scholar] [CrossRef] [Green Version]
- Woern, A.L.; Pearce, J.M. 3-D Printable Polymer Pelletizer Chopper for Fused Granular Fabrication-Based Additive Manufacturing. Inventions 2018, 3, 78. [Google Scholar] [CrossRef] [Green Version]
- Baechler, C.; DeVuono, M.; Pearce, J.M. Distributed recycling of waste polymer into RepRap feedstock. Rapid Prototyp. J. 2013, 19, 118–125. [Google Scholar] [CrossRef]
- Zhong, S.; Rakhe, P.; Pearce, J.M. Energy Payback Time of a Solar Photovoltaic Powered Waste Plastic Recyclebot System. Recycling 2017, 2, 10. [Google Scholar] [CrossRef]
- Woern, A.L.; McCaslin, J.R.; Pringle, A.M.; Pearce, J.M. RepRapable Recyclebot: Open source 3-D printable extruder for converting plastic to 3-D printing filament. HardwareX 2018, 4. [Google Scholar] [CrossRef]
- Hunt, E.J.; Zhang, C.; Anzalone, N.; Pearce, J.M. Polymer recycling codes for distributed manufacturing with 3-D printers. Resour. Conserv. Recycl. 2015, 97, 24–30. [Google Scholar] [CrossRef]
- Zander, N.E.; Gillan, M.; Lambeth, R.H. Recycled polyethylene terephthalate as a new FFF feedstock material. Addit. Manuf. 2018, 21, 174–182. [Google Scholar] [CrossRef]
- Zander, N.E. Recycled Polymer Feedstocks for Material Extrusion Additive Manufacturing. In Polymer-Based Additive Manufacturing: Recent Developments; ACS Symposium Series; American Chemical Society: Washongton, DC, USA, 2019; Volume 1315, pp. 37–51. ISBN 978-0-8412-3426-0. [Google Scholar]
- Mohammed, M.I.; Wilson, D.; Gomez-Kervin, E.; Vidler, C.; Rosson, L.; Long, J. The Recycling of E-Waste ABS Plastics by Melt Extrusion and 3D Printing Using Solar Powered Devices as a Transformative Tool for Humanitarian Aid. 13. Available online: https://pdfs.semanticscholar.org/bb18/94b5b601719eafb85ce314a90c805819b3a7.pdf (accessed on 3 April 2020).
- Singh, A.K.; Patil, B.; Hoffmann, N.; Saltonstall, B.; Doddamani, M.; Gupta, N. Additive Manufacturing of Syntactic Foams: Part 1: Development, Properties, and Recycling Potential of Filaments. JOM 2018, 70, 303–309. [Google Scholar] [CrossRef]
- Chong, S.; Pan, G.-T.; Yang, T.C.-K.; Hung, S.-T.; Huang, C.-M. Physical Characterization and Pre-assessment of Recycled High-Density Polyethylene as 3D Printing Material. J. Polym. Environ. 2016, 25, 136–145. [Google Scholar] [CrossRef]
- Pringle, A.M.; Rudnicki, M.; Pearce, J. Wood Furniture Waste-Based Recycled 3-D Printing Filament. For. Prod. J. 2017, 68, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Hart, K.R.; Frketic, J.B.; Brown, J.R. Recycling meal-ready-to-eat (MRE) pouches into polymer filament for material extrusion additive manufacturing. Addit. Manuf. 2018, 21, 536–543. [Google Scholar] [CrossRef]
- Zander, N.E.; Gillan, M.; Burckhard, Z.; Gardea, F. Recycled polypropylene blends as novel 3D printing materials. Addit. Manuf. 2019, 25, 122–130. [Google Scholar] [CrossRef]
- Pacheco, V.M. Manufacture of Furniture under Demand with Low Environmental Impact Through 3D Printing of Recycled Plastic. 6. Available online: https://www.researchgate.net/publication/335608900_Recycled_3d_printing_applied_to_low_environmental_impact_furniture_manufacturing (accessed on 3 April 2020).
- Löschke, S.K.; Mai, J.; Proust, G.; Brambilla, A. Microtimber: The Development of a 3D Printed Composite Panel Made from Waste Wood and Recycled Plastics. In Digital Wood Design: Innovative Techniques of Representation in Architectural Design; Bianconi, F., Filippucci, M., Eds.; Lecture Notes in Civil Engineering; Springer International Publishing: Cham, Switzerland, 2019; pp. 827–848. ISBN 978-3-030-03676-8. [Google Scholar]
- Volpato, N.; Kretschek, D.; Foggiatto, J.A.; Cruz, C.M.G.D.S. Experimental analysis of an extrusion system for additive manufacturing based on polymer pellets. Int. J. Adv. Manuf. Technol. 2015, 81, 1519–1531. [Google Scholar] [CrossRef]
- Liu, X.; Chi, B.; Jiao, Z.; Tan, J.; Liu, F.; Yang, W. A large-scale double-stage-screw 3D printer for fused deposition of plastic pellets. J. Appl. Polym. Sci. 2017, 134, 45147. [Google Scholar] [CrossRef]
- Woern, A.L.; Byard, D.J.; Oakley, R.B.; Fiedler, M.J.; Snabes, S.L.; Pearce, J.M. Fused Particle Fabrication 3-D Printing: Recycled Materials’ Optimization and Mechanical Properties. Material 2018, 11, 1413. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Jain, P.K.; Tandon, P.; Pandey, P.M. Additive manufacturing of flexible electrically conductive polymer composites via CNC-assisted fused layer modeling process. J. Braz. Soc. Mech. Sci. Eng. 2018, 40, 175. [Google Scholar] [CrossRef]
- Whyman, S.; Arif, K.M.; Potgieter, J. Design and development of an extrusion system for 3D printing biopolymer pellets. Int. J. Adv. Manuf. Technol. 2018, 96, 3417–3428. [Google Scholar] [CrossRef]
- Reich, M.J.; Woern, A.L.; Tanikella, N.G.; Pearce, J.M. Mechanical Properties and Applications of Recycled Polycarbonate Particle Material Extrusion-Based Additive Manufacturing. Material 2019, 12, 1642. [Google Scholar] [CrossRef] [Green Version]
- Nilsiam, Y.; Pearce, J.M. Open Source Database and Website to Provide Free and Open Access to Inactive U.S. Patents in the Public Domain. Inventions 2016, 1, 24. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.M. A review of open source ventilators for COVID-19 and future pandemics. F1000Research 2020, 9, 218. [Google Scholar] [CrossRef] [Green Version]
- Ii, C.W.K.; Cutchis, P.N.; Vincent, J.A.; Smith, D.G.; Wenstrand, D.S. Development of Field Portable Ventilator Systems for Domestic and Military Emergency Medical Response. Tech. Dig. 2004, 25, 9. [Google Scholar]
- Powelson, S.K. Design and prototyping of a low-cost portable mechanical ventilator. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2010. [Google Scholar]
- Al Husseini, A.M.; Lee, H.J.; Negrete, J.; Powelson, S.; Servi, A.T.; Slocum, A.H.; Saukkonen, J. Design and Prototyping of a Low-Cost Portable Mechanical Ventilator. J. Med Devices 2010, 4, 027514. [Google Scholar] [CrossRef] [Green Version]
- Fogarty, M.; Orr, J.; Westenskow, D.; Brewer, L.; Sakata, D. Electric Blower Based Portable Emergency Ventilator; Utah Space Grant Consort: 2013. Available online: https://digitalcommons.usu.edu/spacegrant/2013/Session4/2 (accessed on 3 April 2020).
- Fuchs, P.; Obermeier, J.; Kamysek, S.; Degner, M.; Nierath, H.; Jürß, H.; Ewald, H.; Schwarz, J.; Becker, M.; Schubert, J. Safety and applicability of a pre-stage public access ventilator for trained laypersons: A proof of principle study. BMC Emerg. Med. 2017, 17, 37. [Google Scholar] [CrossRef] [PubMed]
- Jürß, H.; Degner, M.; Ewald, H. A new compact and low-cost respirator concept for one way usage. IFAC-PapersOnLine 2018, 51, 367–372. [Google Scholar] [CrossRef]
- Shahid, M. Prototyping of Artificial Respiration Machine Using AMBU Bag Compression. In Proceedings of the 2019 International Conference on Electronics, Information, and Communication (ICEIC), Auckland, The Netherland, 22–25 January 2019; pp. 1–6. [Google Scholar]
- PubInv/Covid19-Vent-List. Public Invention: 2020. Available online: https://github.com/PubInv/covid19-vent-list (accessed on 3 April 2020).
- AmboVent. AmboVent/AmboVent. 2020. Available online: https://github.com/AmboVent/AmboVent (accessed on 3 April 2020).
- Garmendia, O.; Rodríguez-Lazaro, M.A.; Otero, J.; Phan, P.; Stoyanova, A.; Dinh-Xuan, A.T.; Gozal, D.; Navajas, D.; Montserrat, J.M.; Farré, R. Low-cost, easy-to-build non-invasive pressure support ventilator for under-resourced regions: Open source hardware description, performance and feasibility testing. Eur. Respir. J. 2020, 2000846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OxyGEN. Available online: https://www.oxygen.protofy.xyz (accessed on 3 April 2020).
- Margolis, M. Arduino Cookbook: Recipes to Begin, Expand, and Enhance Your Projects; O’Reilly Media, Inc.: Newton, MA, USA, 2011; ISBN 978-1-4493-2120-8. [Google Scholar]
- D’Ausilio, A. Arduino: A low-cost multipurpose lab equipment. Behav. Res. Methods 2011, 44, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Banzi, M.; Shiloh, M. Getting Started with Arduino: The Open Source Electronics Prototyping Platform; Maker Media, Inc.: Sevastopol, CA, USA, 2014; ISBN 978-1-4493-6329-1. [Google Scholar]
- Tran, K.; Cimon, K.; Severn, M.; Pessoa-Silva, C.L.; Conly, J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE 2012, 7, e35797. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.S.; Chow, B.K.; Lo, T.; Tsang, O.T.; Ko, F.W.; Ng, S.S.; Gin, T.; Chan, M.T. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different masks. Eur. Respir. J. 2019, 53, 1802339. [Google Scholar] [CrossRef]
- Pulmonary, S.M.F. Is the Creator of P. org H. is an Associate Professor of; Vermont, C.C.M. at the U. of PulmCrit Wee- Could the Best Mode of Noninvasive Support for COVID-19 be CPAP? EMCrit Proj. 2020. Available online: https://emcrit.org/pulmcrit/cpap-covid/ (accessed on 31 March 2020).
- CDC Show Me the Science—When & How to Use Hand Sanitizer in Community Settings|Handwashing|CDC. Available online: https://www.cdc.gov/handwashing/show-me-the-science-hand-sanitizer.html (accessed on 31 March 2020).
- World Health Organization WHO|WHO-Recommended Handrub Formulations. Available online: https://www.who.int/gpsc/information_centre/handrub-formulations/en/ (accessed on 31 March 2020).
- Appropedia Ethanol-Based Hand Sanitizer-Appropedia: The Sustainability Wiki. Available online: https://www.appropedia.org/Ethanol-based_hand_sanitizer (accessed on 31 March 2020).
- Bruijn, E. YouMagine—COVID19 Collection by Erik de Bruijn. Available online: https://www.youmagine.com/ultierik/collections/covid19 (accessed on 31 March 2020).
- Prusa Prusa Protective Face Shield-RC3. Available online: https://www.prusaprinters.org/prints/25857-prusa-protective-face-shield-rc3 (accessed on 31 March 2020).
- 3DVerkstan 3D-Printed Protective Visor-3DVerkstan-Quick to Print, Easy to Assemble. Available online: https://3dverkstan.se/protective-visor/ (accessed on 31 March 2020).
- Simple Face Shield|Overview. Available online: https://wikifactory.com/@adammiklosidesign/simple-face-shield (accessed on 3 April 2020).
- Meisenzahl, M. A 3D Printer Company is Creating Medical Face Shields for Doctors and Nurses Fighting Coronavirus—Here’s How It Works. Available online: https://www.businessinsider.com/coronavirus-3d-printed-face-mask-shield-healthcare-workers-2020-3 (accessed on 31 March 2020).
- UCLA Engineers Using 3-D Printing in Race to Get Coronavirus Face Shields to Hospitals. Dly. News 2020. Available online: https://www.dailynews.com/ucla-engineers-using-3d-printing-laser-cutting-in-race-to-get-coronavirus-fighting-face-shields-to-depleted-hospitals (accessed on 31 March 2020).
- Hack the Pandemic–Copper 3D|Antibacterial 3D Printing. Available online: https://copper3d.com/hackthepandemic/ (accessed on 31 March 2020).
- COVID-19 MASK (Easy-to-Print, no Support, Filter Required). Available online: https://cults3d.com/en/3d-model/tool/covid-19-mask-easy-to-print-no-support-filter-required (accessed on 31 March 2020).
- Billings Help with Personal Protective Equipment for Staff and Patients. Available online: https://www.billingsclinic.com/foundation/ (accessed on 31 March 2020).
- Davies, A.; Thompson, K.-A.; Giri, K.; Kafatos, G.; Walker, J.; Bennett, A. Testing the Efficacy of Homemade Masks: Would They Protect in an Influenza Pandemic? Disaster Med. Public Health Prep. 2013, 7, 413–418. [Google Scholar] [CrossRef]
- A Doctor Explains How to Make the Safest Face Mask. Available online: https://www.youtube.com/watch?v=W6d3twpHwis&feature=youtu.be (accessed on 31 March 2020).
- Yip, E.; Cacioli, P. The manufacture of gloves from natural rubber latex. J. Allergy Clin. Immunol. 2002, 110, S3–S14. [Google Scholar] [CrossRef]
- Laureto, J.J.; Dessiatoun, S.V.; Ohadi, M.; Pearce, J.M. Open Source Laser Polymer Welding System: Design and Characterization of Linear Low-Density Polyethylene Multilayer Welds. Machines 2016, 4, 14. [Google Scholar] [CrossRef] [Green Version]
- Lasersaur Manual. Available online: https://www.lasersaur.com/ (accessed on 1 April 2020).
- axRap. Available online: http://axrap.blogspot.com/ (accessed on 1 April 2020).
- LaserWeb/LaserWeb4-Binaries; LaserWeb: 2020. Available online: https://github.com/LaserWeb/LaserWeb4-Binaries (accessed on 1 April 2020).
- LaserDuo. Available online: http://laserduo.com/ (accessed on 1 April 2020).
- Calling All Makers: Here’s a 1-Page PDF Facemask Pattern; Now Go Make Some and Help Beat This Thing. Available online: https://freesewing.org/blog/facemask-frenzy (accessed on 1 April 2020).
- Seamly2D. Available online: https://seamly.net/ (accessed on 1 April 2020).
- Pearce, J.M. The case for open source appropriate technology. Environ. Dev. Sustain. 2012, 14, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Kang, G.; Roy, S.; Balraj, V. Appropriate technology for rural India – solar decontamination of water for emergency settings and small communities. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 863–866. [Google Scholar] [CrossRef]
- Kumagai, A.; Liu, T.I.; Khan, M.; Yu, S.; Wargala, B.; Little, A.; Johnson, R.; Bear, J. Manufacturing Methods for Producing Water Pasteurization Indicators (WAPI); ASME International: New York City, NY, USA, 2006; pp. 485–489. [Google Scholar]
- Rodriguez, V. Water Pasteurization Indicator (WAPI) Maker Redesign. 2012. Available online: http://dspace.calstate.edu/handle/10211.9/1543 (accessed on 1 April 2020).
- Linde, A. Technology Encounters Tradition: Evaluating the Water Pasteurization Indicator in China. 2013. Available online: https://scholarsbank.uoregon.edu/xmlui/handle/1794/12863 (accessed on 1 April 2020).
- Denkenberger, D.C.; Pearce, J.M. Design Optimization of Polymer Heat Exchanger for Automated Household-Scale Solar Water Pasteurizer. Designs 2018, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Gong, H.; Beauchamp, M.; Perry, S.; Woolley, A.T.; Nordin, G.P. Optical Approach to Resin Formulation for 3D Printed Microfluidics. RSC Adv. 2015, 5, 106621–106632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attalla, R.; Ling, C.; Selvaganapathy, P.R. Fabrication and characterization of gels with integrated channels using 3D printing with microfluidic nozzle for tissue engineering applications. Biomed. Microdevices 2016, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, N.; Urrios, A.; Kang, S.; Folch, A. The upcoming 3D-printing revolution in microfluidics. Lab Chip 2016, 16, 1720–1742. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.M.; Anzalone, N.C.; Heldt, C.L. Open-Source Wax RepRap 3-D Printer for Rapid Prototyping Paper-Based Microfluidics. J. Lab. Autom. 2016, 21, 510–516. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Wu, Y.; Fu, J.-Z.; Gao, Q.; Qiu, J.-J. Developments of 3D Printing Microfluidics and Applications in Chemistry and Biology: A Review. Electroanalysis 2016, 28, 1658–1678. [Google Scholar] [CrossRef]
- Tothill, A.M.; Partridge, M.; James, S.W.; Tatam, R.P. Fabrication and optimisation of a fused filament 3D-printed microfluidic platform. J. Micromech. Microeng. 2017, 27, 035018. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Yang, J.; Li, K.; Zhu, L.; Tang, W. Fabrication of PDMS microfluidic devices with 3D wax jetting. RSC Adv. 2017, 7, 3313–3320. [Google Scholar] [CrossRef] [Green Version]
- Gaal, G.; Mendes, M.; De Almeida, T.P.; Piazzetta, M.H.; Gobbi, Â.L.; Riul, A.; Rodrigues, V. Simplified fabrication of integrated microfluidic devices using fused deposition modeling 3D printing. Sens. Actuators B Chem. 2017, 242, 35–40. [Google Scholar] [CrossRef]
- Kong, D.S.; A Thorsen, T.; Babb, J.; Wick, S.; Gam, J.J.; Weiss, R.; A Carr, P. Open-source, community-driven microfluidics with Metafluidics. Nat. Biotechnol. 2017, 35, 523–529. [Google Scholar] [CrossRef]
- A Conner-Kerr, T.; Sullivan, P.K.; Gaillard, J.; E Franklin, M.; Jones, R.M. The effects of ultraviolet radiation on antibiotic-resistant bacteria in vitro. Ostomy Wound Manag. 1998, 44, 50–56. [Google Scholar]
- Chang, J.C.; Ossoff, S.F.; Lobe, D.C.; Dorfman, M.H.; Dumais, C.M.; Qualls, R.G.; Johnson, J.D. UV inactivation of pathogenic and indicator microorganisms. Appl. Environ. Microbiol. 1985, 49, 1361–1365. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Li, J.-S.; Jin, M.; Zhen, B.; Kong, Q.-X.; Song, N.; Xiao, W.; Yin, J.; Wei, W.; Wang, G.-J.; et al. Study on the resistance of severe acute respiratory syndrome-associated coronavirus. J. Virol. Methods 2005, 126, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.-M.; Zhao, X.-S.; Wen, R.-F.; Huang, J.-J.; Pi, G.-H.; Zhang, S.-X.; Han, J.; Bi, S.-L.; Ruan, L.; Dong, X.-P. Stability of SARS coronavirus in human specimens and environment and its sensitivity to heating and UV irradiation. Biomed. Environ. Sci. 2003, 16, 246–255. [Google Scholar]
- Bentancor, M.; Vidal, S. Programmable and low-cost ultraviolet room disinfection device. HardwareX 2018, 4, e00046. [Google Scholar] [CrossRef]
- Card, K.J.; Crozier, D.; Dhawan, A.; Dinh, M.; Dolson, E.; Farrokhian, N.; Gopalakrishnan, V.; Ho, E.; King, E.S.; Krishnan, N.; et al. UV Sterilization of Personal Protective Equipment with Idle Laboratory Biosafety Cabinets During the Covid-19 Pandemic. Occup. Environ. Health 2020. [Google Scholar] [CrossRef] [Green Version]
- Health, C. for D. and R. N95 Respirators and Surgical Masks (Face Masks); FDA: Washington, DC, USA, 2020.
- Gordon, I.; Hahn, K.; Fischer, S. Infection. Atlas Bone Scintigr. Pathol. Paediatr. Skelet. 1996, 12, 7–59. [Google Scholar] [CrossRef]
- Van Der Sande, M.A.B.; Teunis, P.; Sabel, R. Professional and Home-Made Face Masks Reduce Exposure to Respiratory Infections among the General Population. PLoS ONE 2008, 3, e2618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JoJoBoBo Fight The Tide! DIY Laundry Detergent. Corp. Monkey CPA 2017. Available online: https://www.corporatemonkeycpa.com/2017/01/11/diy-laundry-detergent/ (accessed on 2 April 2020).
- Marr, K. (No Borax) Homemade Powder Laundry Soap with Natural Fabric Softener. Live Simply 2018. Available online: https://livesimply.me/no-borax-homemade-powder-laundry-soap-with-natural-fabric-softener/ (accessed on 2 April 2020).
- Caudill, M. How To Make Homemade Soap From Scratch In 6 Easy Steps. Available online: https://www.goodhousekeeping.com/home/cleaning/a20705805/how-to-make-homemade-soap/ (accessed on 2 April 2020).
- How to Make Washing Soda from Baking Soda|Wellness Mama. Wellness Mama 2016. Available online: https://wellnessmama.com/76866/washing-soda/ (accessed on 2 April 2020).
- California Legislature Today’s Law As Amended. Available online: https://leginfo.legislature.ca.gov/faces/billCompareClient.xhtml?bill_id=201520160SB225 (accessed on 3 April 2020).
- D20 Committee. Test Method for Propagation Tear Resistance of Plastic Film and Thin Sheeting by Pendulum Method; ASTM International: West Conshohocken, PA, USA, 2015. [Google Scholar]
- D20 Committee. Test Methods for Impact Resistance of Plastic Film by the Free-Falling Dart Method; ASTM International: West Conshohocken, PA, USA, 2016. [Google Scholar]
- Criado, T.S.; Rodríguez-Giralt, I.; Mencaroni, A. Care in the (critical) making. Open prototyping, or the radicalisation of independent-living politics. Alter 2016, 10, 24–39. [Google Scholar] [CrossRef]
- Oyelude, A. Assistive technologies in libraries and the classroom. Libr. Tech. News 2017, 34, 22–23. [Google Scholar] [CrossRef]
- Rossa-Sierra, A.; Cortes-Chavez, F.; Vidana-Zavala, D.; Munno, M.G.T. Design of a Wheelchair for Low-Income Countries, the Second Stage of a Project. In Proceedings of the Advances in Design for Inclusion; Di Bucchianico, G., Ed.; Springer International Publishing: Cham, Seitzerland, 2020; pp. 301–309. [Google Scholar]
- Thingiverse.com Wheelchair for People in Third World Countries “HU-GO” by Hugoarchicad. Available online: https://www.thingiverse.com/thing:1081797 (accessed on 3 April 2020).
- Kigali Chair Project-Clara Romaní Anthony. Available online: https://cargocollective.com/clararomani/Kigali-Chair-Project-1 (accessed on 3 April 2020).
- TooWheels-the Opensource Wheelchair. Available online: https://hackaday.io/project/25757-toowheels-the-opensource-wheelchair (accessed on 3 April 2020).
- SafariSeat. Available online: http://www.safariseat.org/ (accessed on 3 April 2020).
- Cangiano, S.; Romano, Z. Ease of Repair as a Design Ideal: A Reflection on How Open Source Models Can Support Longer Lasting Ownership of, and Care for, Technology|Ephemera. Available online: http://www.ephemerajournal.org/contribution/ease-repair-design-ideal-reflection-how-open-source-models-can-support-longer-lasting (accessed on 3 April 2020).
- Meehan, T. Universal Glucometer. Available online: https://hackaday.io/project/10865-universal-glucometer (accessed on 3 April 2020).
- GitHub-Nebulabio/Gluco: An Open Source Glucometer. Available online: https://github.com/nebulabio/gluco (accessed on 3 April 2020).
- Printing Low-Cost Glucose Test Strips on Paper. Available online: https://www.healthline.com/diabetesmine/printing-low-cost-glucose-test-strips-on-paper-or-from-silk (accessed on 3 April 2020).
- Open Source Pharma. Available online: https://www.opensourcepharma.net/ (accessed on 3 April 2020).
- Vaughan-Nichols, S.J. Supercomputers: All Linux, all the Time. Available online: https://www.zdnet.com/article/supercomputers-all-linux-all-the-time/ (accessed on 3 April 2020).
- Kerner, S. Linux Foundation on Track for Best Year Ever as Open Source Dominates. Available online: https://www.serverwatch.com/server-news/linux-foundation-on-track-for-best-year-ever-as-open-source-dominates.html (accessed on 3 April 2020).
- Hall, C. Survey Shows Linux the Top Operating System for Internet of Things Devices. Available online: https://www.itprotoday.com/iot/survey-shows-linux-top-operating-system-internet-things-devices (accessed on 3 April 2020).
- Maurer, S.M.; Rai, A.; Sali, A. Finding Cures for Tropical Diseases: Is Open Source an Answer? PLoS Med. 2004, 1, e56. [Google Scholar] [CrossRef] [Green Version]
- Allarakhia, M.; Ajuwon, L. Understanding and creating value from open source drug discovery for neglected tropical diseases. Expert Opin. Drug Discov. 2012, 7, 643–657. [Google Scholar] [CrossRef]
- Williamson, A.E.; Ylioja, P.M.; Robertson, M.N.; Antonova-Koch, Y.; Avery, V.; Baell, J.B.; Batchu, H.; Batra, S.; Burrows, J.N.; Bhattacharyya, S.; et al. Open Source Drug Discovery: Highly Potent Antimalarial Compounds Derived from the Tres Cantos Arylpyrroles. ACS Central Sci. 2016, 2, 687–701. [Google Scholar] [CrossRef] [Green Version]
- Ertl, P.; Jelfs, S. Designing drugs on the internet? Free web tools and services supporting medicinal chemistry. Curr. Top. Med. Chem. 2007, 7, 1491–1501. [Google Scholar] [CrossRef]
- Hope, J. Biobazaar: The Open Source Revolution and Biotechnology; Harvard University Press: Cambridge, MA, USA, 2009; ISBN 978-0-674-03360-3. [Google Scholar]
- Woelfle, M.; Olliaro, P.; Todd, M.H. Open science is a research accelerator. Nat. Chem. 2011, 3, 745–748. [Google Scholar] [CrossRef]
- Årdal, C.; Røttingen, J.-A. Open Source Drug Discovery in Practice: A Case Study. PLoS Neglected Trop. Dis. 2012, 6, e1827. [Google Scholar] [CrossRef] [Green Version]
- Robertson, M.; Ylioja, P.M.; Williamson, A.E.; Woelfle, M.; Robins, M.; Badiola, K.A.; Willis, P.; Olliaro, P.; Wells, T.; Todd, M.H. Open source drug discovery—A limited tutorial. Parasitology 2013, 141, 148–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balasegaram, M.; Kolb, P.; McKew, J.; Menon, J.; Olliaro, P.; Sablinski, T.; Thomas, Z.; Todd, M.H.; Torreele, E.; Wilbanks, J. An open source pharma roadmap. PLoS Med. 2017, 14, e1002276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DNS-Fresenius Kabi India. Available online: https://www.fresenius-kabi.com/in/products/dns (accessed on 3 April 2020).
- Commissioner, O. FDA Commissioner Scott Gottlieb, M.D., Updates on Some Ongoing Shortages Related to IV Fluids. Available online: https://www.fda.gov/news-events/press-announcements/fda-commissioner-scott-gottlieb-md-updates-some-ongoing-shortages-related-iv-fluids (accessed on 3 April 2020).
- Mazer-Amirshahi, M.; Fox, E.R. Saline Shortages—Many Causes, No Simple Solution. N. Engl. J. Med. 2018, 378, 1472–1474. [Google Scholar] [CrossRef] [PubMed]
- Dextrose 5%-Fresenius Kabi India. Available online: https://www.fresenius-kabi.com/in/products/dextrose-5 (accessed on 3 April 2020).
- Fishel, H. 7 Ways to Make Your Own Cold Packs at Home. Available online: https://macgyverisms.wonderhowto.com/how-to/7-ways-make-your-own-cold-packs-home-0166182/ (accessed on 3 April 2020).
- Holling, C.S. Resilience and Stability of Ecological Systems. Annu. Rev. Ecol. Syst. 1973, 4, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Christopher, M.; Peck, H. Building the Resilient Supply Chain. Int. J. Logist. Manag. 2004, 15, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Sheffi, Y. Preparing for the big one [supply chain management]. Manuf. Eng. 2005, 84, 12–15. [Google Scholar] [CrossRef]
- Ponomarov, S.Y.; Holcomb, M.C. Understanding the concept of supply chain resilience. Int. J. Logist. Manag. 2009, 20, 124–143. [Google Scholar] [CrossRef]
- Jüttner, U.; Maklan, S. Supply chain resilience in the global financial crisis: An empirical study. Supply Chain Manag. Int. J. 2011, 16, 246–259. [Google Scholar] [CrossRef]
- Lee, S.M.; Rha, J.S. Ambidextrous supply chain as a dynamic capability: Building a resilient supply chain. Manag. Decis. 2016, 54, 2–23. [Google Scholar] [CrossRef]
- Sanchis, R.; Canetta, L.; Poler, R. A Conceptual Reference Framework for Enterprise Resilience Enhancement. Sustainability 2020, 12, 1464. [Google Scholar] [CrossRef] [Green Version]
- Marusek, J.A. Solar Storm Threat Analysis. 2007. Volume 29. Available online: https://pdfs.semanticscholar.org/9fa3/16d0b9bb073d9826d9d4295b36e0f282d3eb.pdf (accessed on 3 April 2020).
- Weintraub, K. Not Just Ventilators: Staff Trained to Run Them Are in Short Supply. Available online: https://www.scientificamerican.com/article/not-just-ventilators-staff-trained-to-run-them-are-in-short-supply/ (accessed on 4 May 2020).
- Gaffney, A. America’s Extreme Neoliberal Healthcare System is Putting the Country at Risk|Adam Gaffney. The Guardian, 2020. Available online: https://www.theguardian.com/commentisfree/2020/mar/21/medicare-for-all-coronavirus-covid-19-single-payer (accessed on 4 May 2020).
- Abrams, A. America’s Health System Will Likely Make the Coronavirus Outbreak Worse. Available online: https://time.com/5794672/health-insurance-deductibles-coronavirus/ (accessed on 4 May 2020).
- Denkenberger, D.; Pearce, J.M. Feeding Everyone No Matter What: Managing Food Security After Global Catastrophe; Academic Press: Cambridge, MA, USA, 2014; ISBN 978-0-12-802358-7. [Google Scholar]
- Denkenberger, D.C.; Pearce, J.M. Feeding everyone: Solving the food crisis in event of global catastrophes that kill crops or obscure the sun. Futures 2015, 72, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Baum, S.D.; Denkenberger, D.C.; Pearce, J.M.; Robock, A.; Winkler, R. Resilience to global food supply catastrophes. Environ. Syst. Decis. 2015, 35, 301–313. [Google Scholar] [CrossRef] [Green Version]
- Wijnen, B.; Hunt, E.J.; Anzalone, G.C.; Pearce, J.M. Open-Source Syringe Pump Library. PLoS ONE 2014, 9, e107216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijnen, B.; Anzalone, G.C.; Haselhuhn, A.S.; Sanders, P.G.; Pearce, J.M. Free and Open-source Control Software for 3-D Motion and Processing. J. Open Res. Softw. 2016, 4, 177. [Google Scholar] [CrossRef] [Green Version]
- Lynch Open Source Syringe Pump Modifications-Appropedia: The Sustainability Wiki. Available online: https://www.appropedia.org/Lynch_open_source_syringe_pump_modifications (accessed on 3 April 2020).
- Amarante, L.; Newport, J.; Mitchell, M.; Wilson, J.; Laubach, M. An Open Source Syringe Pump Controller for Fluid Delivery of Multiple Volumes. eNeuro 2019, 6, 6. [Google Scholar] [CrossRef]
- Cubberley, M.S.; Hess, W.A. An Inexpensive Programmable Dual-Syringe Pump for the Chemistry Laboratory. J. Chem. Educ. 2016, 94, 72–74. [Google Scholar] [CrossRef]
- Pusch, K.; Hinton, T.J.; Feinberg, A.W.W. Large volume syringe pump extruder for desktop 3D printers. HardwareX 2018, 3, 49–61. [Google Scholar] [CrossRef]
- Lake, J.R.; Heyde, K.C.; Ruder, W.C. Low-cost feedback-controlled syringe pressure pumps for microfluidics applications. PLoS ONE 2017, 12, e0175089. [Google Scholar] [CrossRef]
- Klar, V.; Pearce, J.M.; Kärki, P.; Kuosmanen, P. Ystruder: Open source multifunction extruder with sensing and monitoring capabilities. HardwareX 2019, 6, e00080. [Google Scholar] [CrossRef]
- MOST Lab COVID19 Medical Production-Appropedia: The Sustainability Wiki. Available online: https://www.appropedia.org/MOST_Lab_COVID19_Medical_Production (accessed on 3 April 2020).
- Hall, D.E.; Hanusa, B.H.; Stone, R.A.; Ling, B.S.; Arnold, R.M. Time required for institutional review board review at one Veterans Affairs medical center. JAMA Surg. 2015, 150, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Health, C. for D. and R. Medical Devices. Available online: https://www.fda.gov/medical-devices (accessed on 3 April 2020).
- Enforcement Policy for Ventilators and Accessories and Other Respiratory Devices During the Coronavirus Disease 2019 (COVID-19) Public Health Emergency-Guidance for Industry and Food and Drug Administration Staff. 14. Available online: https://www.fda.gov/media/136318/download (accessed on 3 April 2020).
- Commissioner, O. The Emergency Use Authorization; FDA: Washongton, DC, USA, 2020.
- CSMS #42124872 -Information for Filing Personal Protective Equipment and Medical Devices During COVID-19. Available online: https://content.govdelivery.com/accounts/USDHSCBP/bulletins/282c648 (accessed on 3 April 2020).
- Pardun, J.T. Good Samaritan Laws: A Global Perspective. Loyola Los Angel. Int. Comp. Law J. 1997, 20, 591. [Google Scholar]
- A Comparative Study of the Acts of Good Samaritan of Various Countries--<Hebei Law Science>. Available online: http://en.cnki.com.cn/Article_en/CJFDTotal-HBFX200607001.htm (accessed on 3 April 2020).
- FINLEX ®-Translations of Finnish Acts and Decrees: 39/1889 English. Available online: https://finlex.fi/en/laki/kaannokset/1889/en18890039 (accessed on 3 April 2020).
- Heller, M.A. Can Patents Deter Innovation? The Anticommons in Biomedical Research. Science 1998, 280, 698–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowery, D.C.; Nelson, R.R.; Sampat, B.N.; Ziedonis, A. The growth of patenting and licensing by U.S. universities: An assessment of the effects of the Bayh–Dole act of 1980. Res. Policy 2001, 30, 99–119. [Google Scholar] [CrossRef]
- Pearce, J.M. Make nanotechnology research open-source. Nature 2012, 491, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.M. Open-source nanotechnology: Solutions to a modern intellectual property tragedy. Nano Today 2013, 8, 339–341. [Google Scholar] [CrossRef] [Green Version]
- Chesbrough, H. Open Business Models: How To Thrive. In The New Innovation Landscape; Harvard Business Press: Cambridge, MA, USA, 2006; ISBN 978-1-4221-4807-5. [Google Scholar]
- Watson, R.; Boudreau, M.-C.; York, P.T.; Greiner, M.E.; Wynn, D. The business of open source. Commun. ACM 2008, 51, 41–46. [Google Scholar] [CrossRef]
- Wesselius, J. The Bazaar inside the Cathedral: Business Models for Internal Markets. IEEE Softw. 2008, 25, 60–66. [Google Scholar] [CrossRef]
- An Analysis of Open Source Business Models.—Openforum Academy. Available online: http://openforumacademy.org/library/third-party-research/third-party-research/an-analysis-of-open-source-business-models-1 (accessed on 3 April 2020).
- Osborn, L.S.; Pearce, J.M.; Haselhuhn, A. A Case for Weakening Patent Rights. Law Rev. 2015, 89, 1185. [Google Scholar]
- Kulish, N.; Kliff, S.; Silver-Greenberg, J. The U.S. Tried to Build a New Fleet of Ventilators. The Mission Failed. New York Times, 2020. Available online: https://www.nytimes.com/2020/03/29/business/coronavirus-us-ventilator-shortage.html (accessed on 3 April 2020).
- Medtronic Register to Download Ventilator Files. Available online: https://www.medtronic.com/us-en/e/open-files.html (accessed on 31 March 2020).
- Else, H. Radical open-access plan could spell end to journal subscriptions. Nature 2018, 561, 17–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | OS Base Device Status | OS Manufacture of Components Status |
|---|---|---|
| 1. Ventilators | POS | Closed |
| 2. Alcohol based hand-rub | FOSH | FOSH |
| 3. Face shield (eye, nose, and mouth protection) | FOSH | FOSH |
| 4. N95 Masks | FOSH | Closed |
| 5. Latex single use gloves (clinical) | Closed | Closed |
| 6. Reusable vinyl/rubber gloves (cleaning) | Closed | Closed |
| 7. Eye protection (visor/goggles) | POS | Closed |
| 8. Protective gowns/aprons | Closed | Closed |
| 9. Disposable thermometers | Closed | Closed |
| 10. UV tube light for sterilization | FOSH | Closed |
| 11. Medical masks (surgical/procedure) | FOSH | Closed |
| 12. Detergent/Disinfectant | FOSH | FOSH |
| 13. Single-use towels | FOSH | Closed |
| 14. Biohazard bags | FOSH | POS |
| 15. Wheelchair | FOSH | FOSH |
| 16. Glucometer with strips | FOSH | POS |
| 17. Medicine | Closed | Closed |
| 18. IV Fluid-DNS | FOSH | Closed |
| 19. IV Fluid-Dextrose | FOSH | Closed |
| 20. Hard-frozen gel packs | FOSH | FOSH |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearce, J.M. Distributed Manufacturing of Open Source Medical Hardware for Pandemics. J. Manuf. Mater. Process. 2020, 4, 49. https://doi.org/10.3390/jmmp4020049
Pearce JM. Distributed Manufacturing of Open Source Medical Hardware for Pandemics. Journal of Manufacturing and Materials Processing. 2020; 4(2):49. https://doi.org/10.3390/jmmp4020049
Chicago/Turabian StylePearce, Joshua M. 2020. "Distributed Manufacturing of Open Source Medical Hardware for Pandemics" Journal of Manufacturing and Materials Processing 4, no. 2: 49. https://doi.org/10.3390/jmmp4020049
APA StylePearce, J. M. (2020). Distributed Manufacturing of Open Source Medical Hardware for Pandemics. Journal of Manufacturing and Materials Processing, 4(2), 49. https://doi.org/10.3390/jmmp4020049