
A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis

 , , , , , , , , , ,
, , , , , , , , , ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
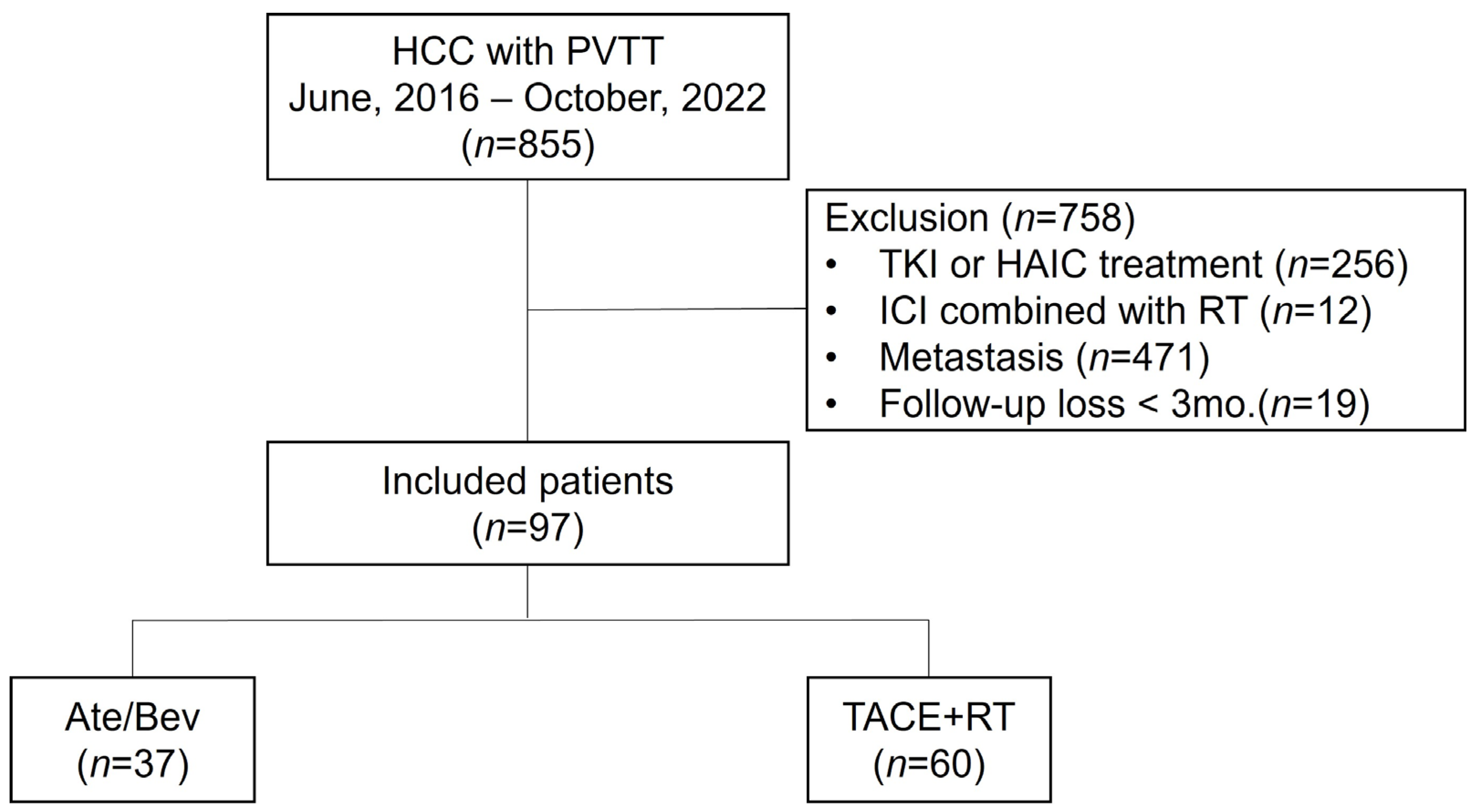
2.1. Patients
2.2. Treatment Regimens
2.3. Assessment of Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. One-Year Survival and PFS in the Entire Population
3.3. Treatment Responses and AEs
3.4. Subgroup Analysis
3.5. Factors Associated with One-Year Survival and PSM Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. S1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kudo, M.; Venook, A.P.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.H.; de Guevara, L.L.; et al. Observational registry of sorafenib use in clinical practice across Child-Pugh subgroups: The GIDEON study. J. Hepatol. 2016, 65, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheon, J.; Yoo, C.; Hong, J.Y.; Kim, H.S.; Lee, D.W.; Lee, M.A.; Kim, J.W.; Kim, I.; Oh, S.B.; Hwang, J.E.; et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2022, 42, 674–681. [Google Scholar] [CrossRef]
- Su, G.L.; Altayar, O.; O’Shea, R.; Shah, R.; Estfan, B.; Wenzell, C.; Sultan, S.; Falck-Ytter, Y. AGA Clinical Practice Guideline on Systemic Therapy for Hepatocellular Carcinoma. Gastroenterology 2022, 162, 920–934. [Google Scholar] [CrossRef]
- Foerster, F.; Gairing, S.J.; Ilyas, S.I.; Galle, P.R. Emerging immunotherapy for HCC: A guide for hepatologists. Hepatology 2022, 75, 1604–1626. [Google Scholar] [CrossRef]
- Valery, M.; Cervantes, B.; Samaha, R.; Gelli, M.; Smolenschi, C.; Fuerea, A.; Tselikas, L.; Klotz-Prieux, C.; Hollebecque, A.; Boige, V.; et al. Immunotherapy and Hepatocellular Cancer: Where Are We Now? Cancers 2022, 14, 4523. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and Safety of Transarterial Chemoembolization Plus External Beam Radiotherapy vs Sorafenib in Hepatocellular Carcinoma with Macroscopic Vascular Invasion: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef]
- 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 583–705. [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Wei, X.; Xu, X. Portal Vein Tumor Thrombosis and Hepatocellular Carcinoma—The Changing Tides. J. Hepatocell. Carcinoma 2021, 8, 1089–1115. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 27 November 2017).
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Goh, M.J.; Sinn, D.H.; Kim, J.M.; Lee, M.W.; Hyun, D.H.; Yu, J.I.; Hong, J.Y.; Choi, M.S. Clinical practice guideline and real-life practice in hepatocellular carcinoma: A Korean perspective. Clin. Mol. Hepatol. 2023, 29, 197–205. [Google Scholar] [CrossRef]
- Guo, L.; Wei, X.; Feng, S.; Zhai, J.; Guo, W.; Shi, J.; Lau, W.Y.; Meng, Y.; Cheng, S. Radiotherapy prior to or after transcatheter arterial chemoembolization for the treatment of hepatocellular carcinoma with portal vein tumor thrombus: A randomized controlled trial. Hepatol. Int. 2022, 16, 1368–1378. [Google Scholar] [CrossRef]
- Facciorusso, A.; Serviddio, G.; Muscatiello, N. Transarterial radioembolization vs chemoembolization for hepatocarcinoma patients: A systematic review and meta-analysis. World J. Hepatol. 2016, 8, 770–778. [Google Scholar] [CrossRef]
- Chang, Y.; Jeong, S.W.; Young Jang, J.; Jae Kim, Y. Recent Updates of Transarterial Chemoembolilzation in Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 8165. [Google Scholar] [CrossRef]
- Raoul, J.L.; Forner, A.; Bolondi, L.; Cheung, T.T.; Kloeckner, R.; de Baere, T. Updated use of TACE for hepatocellular carcinoma treatment: How and when to use it based on clinical evidence. Cancer Treat Rev. 2019, 72, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Choi, J.Y.; Jung, E.S.; Kwon, J.H.; Jang, J.W.; Bae, S.H.; Yoon, S.K. An Immunological Perspective on the Mechanism of Drug Induced Liver Injury: Focused on Drugs for Treatment of Hepatocellular Carcinoma and Liver Transplantation. Int. J. Mol. Sci. 2023, 24, 5002. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, Y.; Qin, S. Atezolizumab and bevacizumab for hepatocellular carcinoma: Mechanism, pharmacokinetics and future treatment strategies. Future Oncol. 2021, 17, 2243–2256. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, J.; Khatiwada, S.; Akon, A.C.; Yu, K.L.; Shen, S.; Zekry, A. Unveiling the complex relationship between gut microbiota and liver cancer: Opportunities for novel therapeutic interventions. Gut Microbes 2023, 15, 2240031. [Google Scholar] [CrossRef]
- Lee, S.K.; Lee, S.W.; Jang, J.W.; Bae, S.H.; Choi, J.Y.; Yoon, S.K. Immunological Markers, Prognostic Factors and Challenges Following Curative Treatments for Hepatocellular Carcinoma. Int. J. Mol. Sci. 2021, 22, 10271. [Google Scholar] [CrossRef]
- Chen, Y.; Hu, H.; Yuan, X.; Fan, X.; Zhang, C. Advances in Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma. Front. Immunol. 2022, 13, 896752. [Google Scholar] [CrossRef]
- Donne, R.; Lujambio, A. The liver cancer immune microenvironment: Therapeutic implications for hepatocellular carcinoma. Hepatology 2023, 77, 1773–1796. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Y.; Hong, W.; Wang, B.; Chen, Y.; Yang, P.; Zhou, J.; Fan, J.; Zeng, Z.; Du, S. Gut microbiota modulate radiotherapy-associated antitumor immune responses against hepatocellular carcinoma Via STING signaling. Gut Microbes 2022, 14, 2119055. [Google Scholar] [CrossRef]
- Wang, K.; Yu, H.M.; Xiang, Y.J.; Cheng, Y.Q.; Ni, Q.Z.; Guo, W.X.; Shi, J.; Feng, S.; Zhai, J.; Cheng, S.Q. Efficacy and safety of radiotherapy combined with atezolizumab plus bevacizumab in treating hepatocellular carcinoma with portal vein tumour thrombus: A study protocol. BMJ Open 2022, 12, e064688. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 97) | General Model | Propensity Score Matching Model | ||||
|---|---|---|---|---|---|---|---|
| Ate/Bev Group | TACE + RT Group | p-Value | Ate/Bev Group | TACE + RT Group | p-Value | ||
| (n = 37) | (n = 60) | (n = 27) | (n = 32) | ||||
| Age, years | 59.1 ± 10.7 | 60.7 ± 12.9 | 58.1 ± 9.0 | 0.283 | 58.1 ± 12.0 | 59.6 ± 9.1 | 0.578 |
| Male | 87 (89.7%) | 35 (94.6%) | 52 (86.7%) | 0.366 | 25 (92.6%) | 30 (93.8%) | 1.000 |
| Cause (n, %) | 0.074 | 0.954 | |||||
| HBV | 73 (76.0%) | 24 (64.9%) | 49 (81.7%) | 20 (74.1%) | 25 (78.1%) | ||
| Others | 23 (24.2%) | 13 (35.1%) | 11 (18.3%) | 7 (25.9%) | 7 (21.9%) | ||
| Treatment-naïve (n, %) | 67 (69.1%) | 22 (59.5%) | 45 (75.0%) | 0.167 | 16 (59.3%) | 25 (78.1%) | 0.199 |
| AST, IU/mL | 70.5 ± 46.1 | 64.1 ± 35.6 | 74.5 ± 51.5 | 0.245 | 68.5 ± 38.2 | 78.5 ± 56.6 | 0.425 |
| ALT, IU/mL | 42.2 ± 31.0 | 35.0 ± 23.7 | 46.5 ± 33.6 | 0.051 | 38.6 ± 26.6 | 49.2 ± 41.3 | 0.240 |
| T.bil, mg/dL | 1.0 ± 0.6 | 0.9 ± 0.7 | 1.1 ± 0.5 | 0.205 | 1.0 ± 0.7 | 1.1 ± 0.5 | 0.945 |
| Alb, g/dL | 3.7 ± 0.6 | 3.8 ± 0.4 | 3.7 ± 0.7 | 0.158 | 3.9 ± 0.4 | 3.9 ± 0.4 | 0.855 |
| PLT, 103/μL | 151.7 ± 64.2 | 162.6 ± 66.0 | 145.0 ± 62.6 | 0.190 | 169.0 ± 69.2 | 151.9 ± 66.6 | 0.339 |
| INR. | 1.1 [1.0; 1.2] | 1.1 [1.0; 1.1] | 1.1 [1.0; 1.2] | 0.293 | 1.1 [1.0; 1.2] | 1.1 [1.0; 1.2] | 0.976 |
| Cr, mg/dL | 0.8 [0.7; 0.9] | 0.7 [0.7; 0.9] | 0.8 [0.6; 0.9] | 0.442 | 0.7 [0.7; 0.9] | 0.9 [0.6; 1.0] | 0.488 |
| CP class A | 84 (86.6%) | 34 (91.9%) | 50 (83.3%) | 0.371 | 24 (88.9%) | 27 (84.4%) | 0.902 |
| AFP, ng/mL | 240.3 [23.9; 1917.6] | 484.4 [40.0; 3175.0] | 189.2 [20.4; 1408.4] | 0.277 | 237.0 [29.9; 2730.0] | 274.6 [27.1; 1408.4] | 0.632 |
| PIVKA, mAU/mL | 1723.0 [161.0; 6670.0] | 2877.0 [230.0; 7521.0] | 1344.0 [140.9; 5870.5] | 0.653 | 2877.0 [245.4; 7753.3] | 3436.3 [208.8; 7065.6] | 0.849 |
| Tumor Size, cm | 8.2 ± 4.6 | 7.6 ± 4.8 | 8.5 ± 4.5 | 0.354 | 7.8 ± 5.0 | 8.8 ± 4.9 | 0.448 |
| Multiple intrahepatic HCC (≥2 nodule) | 68 (70.1%) | 27 (73.0%) | 41 (68.3%) | 0.798 | 19 (70.4%) | 23 (71.9%) | 1.000 |
| Bilobar intrahepatic HCC | 34 (35.1%) | 14 (37.8%) | 20 (33.3%) | 0.816 | 10 (37.0%) | 12 (37.5%) | 1.000 |
| VP4 PVTT | 45 (46.4%) | 15 (40.5%) | 30 (50.0%) | 0.485 | 13 (48.1%) | 15 (46.9%) | 1.000 |
| Adverse Events (AEs) | Total | Ate/Bev | TACE + RT | p-Value |
|---|---|---|---|---|
| (n = 97) | (n = 37) | (n = 60) | ||
| AE yes | 16 (16.5%) | 7 (18.9%) | 9 (15.0%) | 0.823 |
| AE types according to grades | ||||
| Grade 1–2 | 0.068 | |||
| - Proteinuria | 3 (3.1%) | 3 (8.1%) | 0 (0.0%) | |
| - Others | 2 (2.1%) | 1 (2.7%) | 1 (1.7%) | |
| Grade 3–4 | 0.524 | |||
| - Varix bleeding | 7 (7.2%) | 2 (5.4%) | 5 (8.3%) | |
| - Hepatic encephalopathy | 2 (2.1%) | 1 (2.7%) | 1 (1.7%) | |
| - HCC rupture | 2 (2.1%) | 0 (0.0%) | 2 (3.3%) |
| Characteristics | HR | 95% CI | p-Value |
|---|---|---|---|
| Age ≥ 60 | 1.75 | 0.86, 3.54 | 0.12 |
| Male | 2.15 | 0.51, 9.03 | 0.3 |
| Ate/Bev Tx. | 0.38 | 0.15, 1.00 | 0.049 |
| AST ≥ 60, IU/mL | 1.47 | 0.73, 2.96 | 0.3 |
| ALT ≥ 40, IU/mL | 1.16 | 0.58, 2.31 | 0.7 |
| T.bil ≥ 1.0, mg/dL | 1.97 | 0.98, 3.96 | 0.058 |
| Alb ≤ 3.5, g/dL | 1.13 | 0.46, 2.75 | 0.8 |
| INR ≥ 1.1 | 1.00 | 0.50, 2.00 | 1.0 |
| AFP ≥ 200, ng/mL | 0.93 | 0.47, 1.87 | 0.8 |
| PIVKA ≥ 40, mAU/mL | 0.89 | 0.31, 2.55 | 0.8 |
| Size ≥ 8.0, cm | 1.42 | 0.71, 2.85 | 0.3 |
| Multiple intrahepatic HCC | 0.63 | 0.31, 1.28 | 0.2 |
| Bilobar intrahepatic HCC | 0.98 | 0.46, 2.07 | 1.0 |
| VP4 PVTT | 1.33 | 0.66, 2.66 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.K.; Kwon, J.H.; Lee, S.W.; Lee, H.L.; Kim, H.Y.; Kim, C.W.; Song, D.S.; Chang, U.I.; Yang, J.M.; Nam, S.W.; et al. A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis. Cancers 2023, 15, 4423. https://doi.org/10.3390/cancers15174423
Lee SK, Kwon JH, Lee SW, Lee HL, Kim HY, Kim CW, Song DS, Chang UI, Yang JM, Nam SW, et al. A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis. Cancers. 2023; 15(17):4423. https://doi.org/10.3390/cancers15174423
Chicago/Turabian StyleLee, Soon Kyu, Jung Hyun Kwon, Sung Won Lee, Hae Lim Lee, Hee Yeon Kim, Chang Wook Kim, Do Seon Song, U Im Chang, Jin Mo Yang, Soon Woo Nam, and et al. 2023. "A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis" Cancers 15, no. 17: 4423. https://doi.org/10.3390/cancers15174423
APA StyleLee, S. K., Kwon, J. H., Lee, S. W., Lee, H. L., Kim, H. Y., Kim, C. W., Song, D. S., Chang, U. I., Yang, J. M., Nam, S. W., Kim, S. -H., Song, M. J., Kim, J. H., Lee, A., Yang, H., Bae, S. H., Han, J. W., Nam, H., Sung, P. S., ... Kim, M. (2023). A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis. Cancers, 15(17), 4423. https://doi.org/10.3390/cancers15174423