
Radiographic Biomarkers for Knee Osteoarthritis: A Narrative Review

Abstract
:1. Introduction
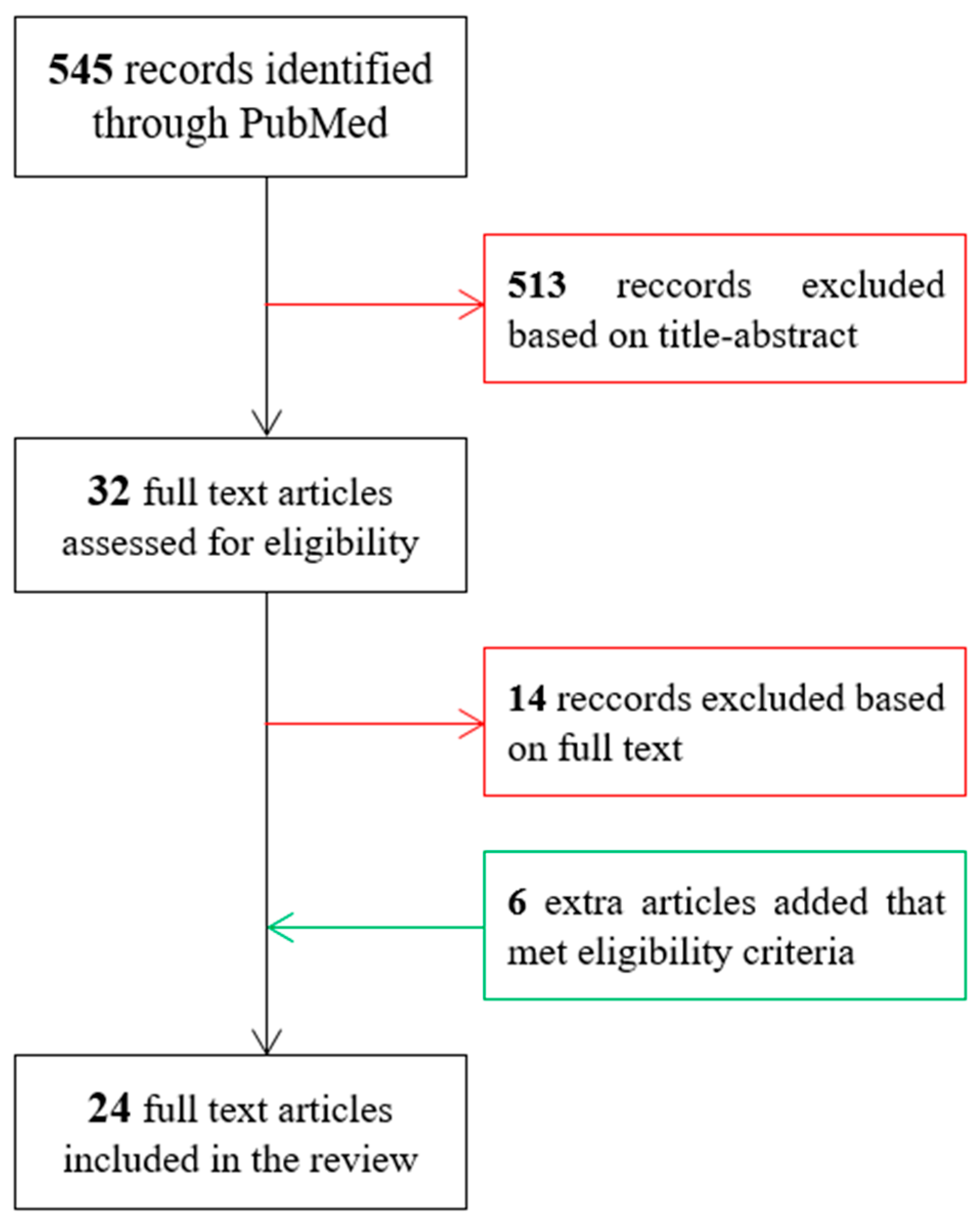
2. Methods
- Name of the study;
- Number of subjects (and images) included;
- Definition of radiographic progression;
- Inclusion criteria;
- Radiographic biomarkers investigated;
- Performance results (if possible, the area under the receiver operating characteristic (ROC) curve (AUC) score, because AUC is usually used to indicate the overall accuracy of a test according to its sensitivity and its specificity).
3. Results
- Prediction of radiographic KOA incidence;
- Prediction of KOA progression;
- Prediction of total knee arthroplasty risk.
3.1. Prediction of KOA Incidence
3.1.1. Increase in Medial Joint Space Narrowing
3.1.2. Increase in Kellgren–Lawrence Grade
3.2. Prediction of KOA Progression
3.2.1. Increase in Medial Joint Space Narrowing
3.2.2. Increase in Kellgren–Lawrence (KL) Grade
3.2.3. Increase in Medial Joint Space Width
3.3. Prediction of Total Knee Replacement Risk
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Richard, M.J.; Driban, J.B.; McAlindon, T.E. Pharmaceutical treatment of osteoarthritis. Osteoarthr. Cartil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Latourte, A.; Kloppenburg, M.; Richette, P. Emerging pharmaceutical therapies for osteoarthritis. Nat. Rev. Rheumatol. 2020, 16, 673–688. [Google Scholar] [CrossRef]
- Gale, D.; Chaisson, C.; Totterman, S.; Schwartz, R.; Gale, M.; Felson, D. Meniscal subluxation: Association with osteoarthritis and joint space narrowing. Osteoarthr. Cartil. 1999, 7, 526–532. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Lane, N.E.; Buckland-Wright, C. Radiographic methods in knee osteoarthritis: A further comparison of semiflexed (MTP), schuss-tunnel, and weight-bearing anteroposterior views for joint space narrowing and osteophytes. J. Rheumatol. 2002, 29, 2597–2601. [Google Scholar]
- Nevitt, M.; Sharma, L. OMERACT workshop radiography session 1. Osteoarthr. Cartil. 2006, 14, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Emrani, P.; Katz, J.; Kessler, C.; Reichmann, W.; Wright, E.; McAlindon, T.; Losina, E. Joint space narrowing and Kellgren–Lawrence progression in knee osteoarthritis: An analytic literature synthesis. Osteoarthr. Cartil. 2008, 16, 873–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakellariou, G.; Conaghan, P.; Zhang, W.; Bijlsma, J.W.J.; Bøyesen, P.; D’Agostino, M.A.; Doherty, M.; Fodor, D.; Kloppenburg, M.; Miese, F.; et al. EULAR recommendations for the use of imaging in the clinical management of peripheral joint osteoarthritis. Ann. Rheum. Dis. 2017, 76, 1484–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.; Arden, N.K. Strategies for the prevention of knee osteoarthritis. Nat. Rev. Rheumatol. 2015, 12, 92–101. [Google Scholar] [CrossRef]
- Reyes, C.; Leyland, K.M.; Peat, G.; Cooper, C.; Arden, N.K.; Prieto-Alhambra, D. Association Between Overweight and Obesity and Risk of Clinically Diagnosed Knee, Hip, and Hand Osteoarthritis: A Population-Based Cohort Study. Arthritis Rheumatol. 2016, 68, 1869–1875. [Google Scholar] [CrossRef] [Green Version]
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.; Protheroe, J.; Jordan, K. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Runhaar, J.; van Middelkoop, M.; Reijman, M.; Vroegindeweij, D.; Oei, E.H.G.; Bierma-Zeinstra, S.M.A. Malalignment: A possible target for prevention of incident knee osteoarthritis in overweight and obese women. Rheumatology 2014, 53, 1618–1624. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; McWilliams, D.F.; Ingham, S.L.; A Doherty, S.; Muthuri, S.; Muir, K.R.; Doherty, M. Nottingham knee osteoarthritis risk prediction models. Ann. Rheum. Dis. 2011, 70, 1599–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazzarini, N.; Runhaar, J.; Bay-Jensen, A.; Thudium, C.; Bierma-Zeinstra, S.; Henrotin, Y.; Bacardit, J. A machine learning approach for the identification of new biomarkers for knee osteoarthritis development in overweight and obese women. Osteoarthr. Cartil. 2017, 25, 2014–2021. [Google Scholar] [CrossRef] [Green Version]
- Kerkhof, H.J.M.; A Bierma-Zeinstra, S.M.; Arden, N.K.; Metrustry, S.; Castano-Betancourt, M.; Hart, D.J.; Hofman, A.; Rivadeneira, F.; Oei, E.H.G.; Spector, T.D.; et al. Prediction model for knee osteoarthritis incidence, including clinical, genetic and biochemical risk factors. Ann. Rheum. Dis. 2013, 73, 2116–2121. [Google Scholar] [CrossRef]
- Halilaj, E.; Le, Y.; Hicks, J.; Hastie, T.; Delp, S. Modeling and predicting osteoarthritis progression: Data from the osteoarthritis initiative. Osteoarthr. Cartil. 2018, 26, 1643–1650. [Google Scholar] [CrossRef] [Green Version]
- Krakowski, P.; Karpiński, R.; Jojczuk, M.; Nogalska, A.; Jonak, J. Knee MRI Underestimates the Grade of Cartilage Lesions. Appl. Sci. 2021, 11, 1552. [Google Scholar] [CrossRef]
- Hayashi, D.; Roemer, F.W.; Guermazi, A. Imaging of Osteoarthritis by Conventional Radiography, MR Imaging, PET–Computed Tomography, and PET–MR Imaging. PET Clin. 2018, 14, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Mathiessen, A.; Cimmino, M.A.; Hammer, H.B.; Haugen, I.K.; Iagnocco, A.; Conaghan, P.G. Imaging of osteoarthritis (OA): What is new? Best Pract. Res. Clin. Rheumatol. 2016, 30, 653–669. [Google Scholar] [CrossRef]
- Dieppe, P.; Cushnaghan, J.; Young, P.; Kirwan, J. Prediction of the progression of joint space narrowing in osteoarthritis of the knee by bone scintigraphy. Ann. Rheum. Dis. 1993, 52, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Goldring, M.B.; Goldring, S.R. Articular cartilage and subchondral bone in the pathogenesis of osteoarthritis. Ann. N. Y. Acad. Sci. 2010, 1192, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fu, S.; Gong, Z.; Zhu, Z.; Zeng, D.; Cao, P.; Lin, T.; Chen, T.; Wang, X.; Lartey, R.; et al. MRI-based Texture Analysis of Infrapatellar Fat Pad to Predict Knee Osteoarthritis Incidence. Radiology 2022, 304, 611–621. [Google Scholar] [CrossRef]
- Zeng, N.; Yan, Z.-P.; Chen, X.-Y.; Ni, G.-X. Infrapatellar Fat Pad and Knee Osteoarthritis. Aging Dis. 2020, 11, 1317–1328. [Google Scholar] [CrossRef] [PubMed]
- Hirvasniemi, J.; Thevenot, J.; Guermazi, A.; Podlipská, J.; Roemer, F.W.; Nieminen, M.T.; Saarakkala, S. Differences in tibial subchondral bone structure evaluated using plain radiographs between knees with and without cartilage damage or bone marrow lesions—The Oulu Knee Osteoarthritis study. Eur. Radiol. 2017, 27, 4874–4882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsiadlo, P.; Nevitt, M.; Wolski, M.; Stachowiak, G.; Lynch, J.; Tolstykh, I.; Felson, D.; Segal, N.; Lewis, C.; Englund, M. Baseline trabecular bone and its relation to incident radiographic knee osteoarthritis and increase in joint space narrowing score: Directional fractal signature analysis in the MOST study. Osteoarthr. Cartil. 2016, 24, 1736–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almhdie-Imjabbar, A.; Podsiadlo, P.; Ljuhar, R.; Jennane, R.; Nguyen, K.-L.; Toumi, H.; Saarakkala, S.; Lespessailles, E. Trabecular bone texture analysis of conventional radiographs in the assessment of knee osteoarthritis: Review and viewpoint. Thromb. Haemost. 2021, 23, 208. [Google Scholar] [CrossRef]
- Kraus, V.B.; Collins, J.E.; Charles, H.C.; Pieper, C.F.; Whitley, L.; Losina, E.; Nevitt, M.; Hoffmann, S.; Roemer, F.; Guermazi, A.; et al. Predictive Validity of Radiographic Trabecular Bone Texture in Knee Osteoarthritis. Arthritis Rheumatol. 2017, 70, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Guan, B.; Liu, F.; Haj-Mirzaian, A.; Demehri, S.; Samsonov, A.; Neogi, T.; Guermazi, A.; Kijowski, R. Deep learning risk assessment models for predicting progression of radiographic medial joint space loss over a 48-MONTH follow-up period. Osteoarthr. Cartil. 2020, 28, 428–437. [Google Scholar] [CrossRef]
- Kraus, V.B.; Feng, S.; Wang, S.; White, S.; Ainslie, M.; Brett, A.; Holmes, A.; Charles, H.C. Trabecular morphometry by fractal signature analysis is a novel marker of osteoarthritis progression. Arthritis Rheum. 2009, 60, 3711–3722. [Google Scholar] [CrossRef] [Green Version]
- Huynh, C.; Puyraimond-Zemmour, D.; Maillefert, J.; Conaghan, P.; Davis, A.; Gunther, K.-P.; Hawker, G.; Hochberg, M.; Kloppenburg, M.; Lim, K.; et al. Factors associated with the orthopaedic surgeon’s decision to recommend total joint replacement in hip and knee osteoarthritis: An international cross-sectional study of 1905 patients. Osteoarthr. Cartil. 2018, 26, 1311–1318. [Google Scholar] [CrossRef] [Green Version]
- Skou, S.T.; Roos, E.M.; Laursen, M.B.; Rathleff, M.S.; Arendt-Nielsen, L.; Simonsen, O.; Rasmussen, S. Criteria used when deciding on eligibility for total knee arthroplasty—Between thinking and doing. Knee 2015, 23, 300–305. [Google Scholar] [CrossRef]
- Verra, W.C.; Witteveen, K.Q.; Maier, A.; Gademan, M.G.J.; Van Der Linden, H.M.J.; Nelissen, R. The reason why orthopaedic surgeons perform total knee replacement: Results of a randomised study using case vignettes. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2697–2703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woloszynski, T.; Podsiadlo, P.; Stachowiak, G.W.; Kurzynski, M.; Lohmander, L.S.; Englund, M. Prediction of progression of radiographic knee osteoarthritis using tibial trabecular bone texture. Arthritis Rheum. 2012, 64, 688–695. [Google Scholar] [CrossRef]
- Duncan, R.; Peat, G.; Thomas, E.; Hay, E.M.; Croft, P. Incidence, progression and sequence of development of radiographic knee osteoarthritis in a symptomatic population. Ann. Rheum. Dis. 2011, 70, 1944–1948. [Google Scholar] [CrossRef] [PubMed]
- Golightly, Y.M.; Allen, K.D.; Helmick, C.G.; Schwartz, T.A.; Renner, J.B.; Jordan, J.M. Hazard of Incident and Progressive Knee and Hip Radiographic Osteoarthritis and Chronic Joint Symptoms in Individuals with and without Limb Length Inequality. J. Rheumatol. 2010, 37, 2133–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garriga, C.; Sánchez-Santos, M.T.; Judge, A.; Hart, D.; Spector, T.; Cooper, C.; Arden, N.K. Predicting Incident Radiographic Knee Osteoarthritis in Middle-Aged Women Within Four Years: The Importance of Knee-Level Prognostic Factors. Arthritis Care Res. 2019, 72, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Janvier, T.; Jennane, R.; Toumi, H.; Lespessailles, E. Subchondral tibial bone texture predicts the incidence of radiographic knee osteoarthritis: Data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2017, 25, 2047–2054. [Google Scholar] [CrossRef] [Green Version]
- Kinds, M.; Marijnissen, A.; Vincken, K.; Viergever, M.; Drossaers-Bakker, K.; Bijlsma, J.; Bierma-Zeinstra, S.; Welsing, P.; Lafeber, F. Evaluation of separate quantitative radiographic features adds to the prediction of incident radiographic osteoarthritis in individuals with recent onset of knee pain: 5-year follow-up in the CHECK cohort. Osteoarthr. Cartil. 2012, 20, 548–556. [Google Scholar] [CrossRef] [Green Version]
- Shamir, L.; Ling, S.; Scott, W.; Hochberg, M.; Ferrucci, L.; Goldberg, I. Early detection of radiographic knee osteoarthritis using computer-aided analysis. Osteoarthr. Cartil. 2009, 17, 1307–1312. [Google Scholar] [CrossRef] [Green Version]
- Joseph, G.B.; McCulloch, C.E.; Nevitt, M.C.; Neumann, J.; Gersing, A.S.; Kretzschmar, M.; Schwaiger, B.; Lynch, J.A.; Heilmeier, U.; Lane, N.E.; et al. Tool for osteoarthritis risk prediction (TOARP) over 8 years using baseline clinical data, X-ray, and MRI: Data from the osteoarthritis initiative. J. Magn. Reson. Imaging 2018, 47, 1517–1526. [Google Scholar] [CrossRef]
- Almhdie-Imjabbar, A.; Nguyen, K.-L.; Toumi, H.; Jennane, R.; Lespessailles, E. Prediction of knee osteoarthritis progression using radiological descriptors obtained from bone texture analysis and Siamese neural networks: Data from OAI and MOST cohorts. Thromb. Haemost. 2022, 24, 66. [Google Scholar] [CrossRef]
- Attur, M.; Krasnokutsky, S.; Zhou, H.; Samuels, J.; Chang, G.; Bencardino, J.; Rosenthal, P.; Rybak, L.; Huebner, J.L.; Kraus, V.B.; et al. The combination of an inflammatory peripheral blood gene expression and imaging biomarkers enhance prediction of radiographic progression in knee osteoarthritis. Thromb. Haemost. 2020, 22, 208. [Google Scholar] [CrossRef]
- Janvier, T.; Jennane, R.; Valery, A.; Harrar, K.; Delplanque, M.; Lelong, C.; Loeuille, D.; Toumi, H.; Lespessailles, E. Subchondral tibial bone texture analysis predicts knee osteoarthritis progression: Data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2016, 25, 259–266. [Google Scholar] [CrossRef] [Green Version]
- Woloszynski, T.; Podsiadlo, P.; Stachowiak, G.; Kurzynski, M. A dissimilarity-based multiple classifier system for trabecular bone texture in detection and prediction of progression of knee osteoarthritis. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2012, 226, 887–894. [Google Scholar] [CrossRef]
- Kraus, V.B.; Feng, S.; Wang, S.; White, S.; Ainslie, M.; Le Graverand, M.-P.H.; Brett, A.; Eckstein, F.; Hunter, D.J.; Lane, N.E.; et al. Subchondral Bone Trabecular Integrity Predicts and Changes Concurrently With Radiographic and Magnetic Resonance Imaging-Determined Knee Osteoarthritis Progression. Arthritis Rheum. 2013, 65, 1812–1821. [Google Scholar] [CrossRef] [Green Version]
- Tiulpin, A.; Klein, S.; Bierma-Zeinstra, S.M.A.; Thevenot, J.; Rahtu, E.; van Meurs, J.; Oei, E.H.G.; Saarakkala, S. Multimodal Machine Learning-based Knee Osteoarthritis Progression Prediction from Plain Radiographs and Clinical Data. Sci. Rep. 2019, 9, 20038. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, P.; Cicuttini, F.; Wolski, M.; Stachowiak, G.; Wluka, A. Trabecular bone texture detected by plain radiography is associated with an increased risk of knee replacement in patients with osteoarthritis: A 6 year prospective follow up study. Osteoarthr. Cartil. 2014, 22, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Kwoh, C.; Guehring, H.; Aydemir, A.; Hannon, M.; Eckstein, F.; Hochberg, M. Predicting knee replacement in participants eligible for disease-modifying osteoarthritis drug treatment with structural endpoints. Osteoarthr. Cartil. 2020, 28, 782–791. [Google Scholar] [CrossRef]
- Bihlet, A.R.; Bjerre-Bastos, J.J.; Andersen, J.R.; Byrjalsen, I.; Karsdal, M.A.; Bay-Jensen, A.-C. Clinical and biochemical factors associated with risk of total joint replacement and radiographic progression in osteoarthritis: Data from two phase III clinical trials. Semin. Arthritis Rheum. 2020, 50, 1374–1381. [Google Scholar] [CrossRef]
- Leung, K.; Zhang, B.; Tan, J.; Shen, Y.; Geras, K.J.; Babb, J.; Cho, K.; Chang, G.; Deniz, C.M. Prediction of Total Knee Replacement and Diagnosis of Osteoarthritis by Using Deep Learning on Knee Radiographs: Data from the Osteoarthritis Initiative. Radiology 2020, 296, 584–593. [Google Scholar] [CrossRef]
- Almhdie-Imjabbar, A.; Toumi, H.; Harrar, K.; Pinti, A.; Lespessailles, E. Subchondral tibial bone texture of conventional X-rays predicts total knee arthroplasty. Sci. Rep. 2022, 12, 8327. [Google Scholar] [CrossRef] [PubMed]
- Istas, J.; Lang, G. Quadratic variations and estimation of the local Hölder index of a Gaussian process. In Annales de l'Institut Henri Poincare (B) Probability and Statistics; Elsevier: Amsterdam, The Netherlands, 1997; Volume 33, pp. 407–436. [Google Scholar] [CrossRef] [Green Version]
- Haverkamp, D.J.; Schiphof, D.; Bierma-Zeinstra, S.M.; Weinans, H.; Waarsing, J.H. Variation in joint shape of osteoarthritic knees. Arthritis Rheum. 2011, 63, 3401–3407. [Google Scholar] [CrossRef]
- Kuo, P.-L.; Schrack, J.A.; Levine, M.E.; Shardell, M.D.; Simonsick, E.M.; Chia, C.W.; Moore, A.Z.; Tanaka, T.; An, Y.; Karikkineth, A.; et al. Longitudinal phenotypic aging metrics in the Baltimore Longitudinal Study of Aging. Nat. Aging 2022, 2, 635–643. [Google Scholar] [CrossRef]
- Peat, G.; Thomas, E.; Handy, J.; Wood, L.; Dziedzic, K.; Myers, H.; Wilkie, R.; Duncan, R.; Hay, E.; Hill, J.; et al. The Knee Clinical Assessment Study—CAS(K). A prospective study of knee pain and knee osteoarthritis in the general population. BMC Musculoskelet. Disord. 2004, 5, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, K. The chingford study. Public Health 1981, 95, 347–352. [Google Scholar] [CrossRef]
- Jordan, J.M. An Ongoing Assessment of Osteoarthritis in African Americans and Caucasians in North Carolina: The Johnston County Osteoarthritis Project. Trans. Am. Clin. Clim. Assoc. 2015, 126, 77–86. [Google Scholar]
- Hofman, A.; Van Duijn, C.M.; Franco, O.; Ikram, M.A.; Janssen, H.L.A.; Klaver, C.; Kuipers, E.J.; Nijsten, T.E.C.; Stricker, B.H.C.; Tiemeier, H.; et al. The Rotterdam Study: 2012 objectives and design update. Eur. J. Epidemiology 2011, 26, 657–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, D.J.; Mootoosamy, I.; Doyle, D.V.; Spector, T.D. The relationship between osteoarthritis and osteoporosis in the general population: The Chingford Study. Ann. Rheum. Dis. 1994, 53, 158–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckstein, F.; Buck, R.J.; Burstein, D.; Charles, H.C.; Crim, J.; Hudelmaier, M.; Hunter, D.J.; Hutchins, G.; Jackson, C.; Kraus, V.B.; et al. Precision of 3.0 Tesla quantitative magnetic resonance imaging of cartilage morphology in a multicentre clinical trial. Ann. Rheum. Dis. 2008, 67, 1683–1688. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosmer, D.W.; Lemeshow, S. Assessing the Fit of the Model. In Applied Logistic Regression; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2000; pp. 143–202. [Google Scholar]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gao, Y.; Sun, X.; Liu, Z.; Zhang, Z.; Qin, L.; Song, J.; Wang, H.; Wu, I.X. Predictive models for the incidence of Parkinson’s disease: Systematic review and critical appraisal. Rev. Neurosci. 2022, 34, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Tazin, T.; Alam, N.; Dola, N.N.; Bari, M.S.; Bourouis, S.; Khan, M.M. Stroke Disease Detection and Prediction Using Robust Learning Approaches. J. Healthc. Eng. 2021, 2021, e7633381. [Google Scholar] [CrossRef] [PubMed]
- Bayramoglu, N.; Nieminen, M.T.; Saarakkala, S. Machine learning based texture analysis of patella from X-rays for detecting patellofemoral osteoarthritis. Int. J. Med. Inform. 2022, 157, 104627. [Google Scholar] [CrossRef]
- Kwon, S.; Ro, D.; Song, M.; Han, H.-S.; Lee, M.; Kim, H. Identifying key gait features associated with the radiological grade of knee osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1755–1760. [Google Scholar] [CrossRef]
- Wong, A.; Beattie, K.; Emond, P.; Inglis, D.; Duryea, J.; Doan, A.; Ioannidis, G.; Webber, C.; O’Neill, J.; de Beer, J.; et al. Quantitative analysis of subchondral sclerosis of the tibia by bone texture parameters in knee radiographs: Site-specific relationships with joint space width. Osteoarthr. Cartil. 2009, 17, 1453–1460. [Google Scholar] [CrossRef] [Green Version]
- Felson, D.; Zhang, Y.; Hannan, M.; Naimark, A.; Weissman, B.N.; Aliabadi, P.; Levy, D. The incidence and natural history of knee osteoarthritis in the elderly, the framingham osteoarthritis study. Arthritis Rheum. 1995, 38, 1500–1505. [Google Scholar] [CrossRef]
- Driban, J.B.; Davis, J.E.; Lu, B.; Price, L.L.; Ward, R.J.; Mackay, J.W.; Eaton, C.B.; Lo, G.H.; Barbe, M.F.; Zhang, M.; et al. Accelerated Knee Osteoarthritis Is Characterized by Destabilizing Meniscal Tears and Preradiographic Structural Disease Burden. Arthritis Rheumatol. 2019, 71, 1089–1100. [Google Scholar] [CrossRef] [Green Version]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Teichtahl, A.J.; Abram, F.; Hussain, S.M.; Pelletier, J.-P.; Cicuttini, F.M.; Martel-Pelletier, J. Knee pain as a predictor of structural progression over 4 years: Data from the Osteoarthritis Initiative, a prospective cohort study. Thromb. Haemost. 2018, 20, 250. [Google Scholar] [CrossRef] [Green Version]
- LaValley, M.P.; Lo, G.H.; Price, L.L.; Driban, J.B.; Eaton, C.B.; McAlindon, T.E. Development of a clinical prediction algorithm for knee osteoarthritis structural progression in a cohort study: Value of adding measurement of subchondral bone density. Thromb. Haemost. 2017, 19, 95. [Google Scholar] [CrossRef] [PubMed]
- Hirvasniemi, J.; Thevenot, J.; Multanen, J.; Haapea, M.; Heinonen, A.; Nieminen, M.; Saarakkala, S. Association between radiography-based subchondral bone structure and MRI-based cartilage composition in postmenopausal women with mild osteoarthritis. Osteoarthr. Cartil. 2017, 25, 2039–2046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, G.; Ding, C.; Cicuttini, F.; Jones, G. A longitudinal study of the association between knee alignment and change in cartilage volume and chondral defects in a largely non-osteoarthritic population. J. Rheumatol. 2007, 34, 181–186. [Google Scholar] [PubMed]
- MacKay, J.W.; Kapoor, G.; Driban, J.B.; Lo, G.H.; McAlindon, T.E.; Toms, A.P.; McCaskie, A.W.; Gilbert, F.J. Association of subchondral bone texture on magnetic resonance imaging with radiographic knee osteoarthritis progression: Data from the Osteoarthritis Initiative Bone Ancillary Study. Eur. Radiol. 2018, 28, 4687–4695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heilmeier, U.; Wamba, J.M.; Joseph, G.B.; Darakananda, K.; Callan, J.; Neumann, J.; Link, T.M. Baseline knee joint effusion and medial femoral bone marrow edema, in addition to MRI-based T2 relaxation time and texture measurements of knee cartilage, can help predict incident total knee arthroplasty 4–7 years later: Data from the Osteoarthritis Initiative. Skelet. Radiol. 2018, 48, 89–101. [Google Scholar] [CrossRef]
- Barr, A.; Dube, B.; Hensor, E.; Kingsbury, S.R.; Peat, G.; Bowes, M.A.; Sharples, L.; Conaghan, P.G. The relationship between three-dimensional knee MRI bone shape and total knee replacement—A case control study: Data from the Osteoarthritis Initiative. Rheumatology 2016, 55, 1585–1593. [Google Scholar] [CrossRef] [Green Version]
- Bowes, M.A.; Vincent, G.R.; Wolstenholme, C.B.; Conaghan, P. A novel method for bone area measurement provides new insights into osteoarthritis and its progression. Ann. Rheum. Dis. 2013, 74, 519–525. [Google Scholar] [CrossRef]
- Lo, G.H.; Schneider, E.; Driban, J.B.; Price, L.L.; Hunter, D.J.; Eaton, C.B.; Hochberg, M.C.; Jackson, R.D.; Kwoh, C.K.; Nevitt, M.C.; et al. Periarticular bone predicts knee osteoarthritis progression: Data from the Osteoarthritis Initiative. Semin. Arthritis Rheum. 2018, 48, 155–161. [Google Scholar] [CrossRef]
- Dell’Isola, A.; Allan, R.; Smith, S.L.; Marreiros, S.S.P.; Steultjens, M. Identification of clinical phenotypes in knee osteoarthritis: A systematic review of the literature. BMC Musculoskelet. Disord. 2016, 17, 425. [Google Scholar] [CrossRef]


{kind=link}
| Objective | Included Studies | Nubmer of Studies |
|---|---|---|
| Prediction of KOA incidence | [14,15,33,34,35,36,37,38,39,40] | 10 |
| Prediction of KOA 1 progression | [27,28,29,33,34,35,41,42,43,44,45,46] | 12 |
| Prediction of TKA 2 risk | [47,48,49,50,51] | 5 |
| Authors (Publication Year, Reference) | Cohort Name (number of Subjects, % of Cases) | Period (Months) | Inclusion Criterion | Incidence Definition | Main Radiographic Biomarkers | Best AUC |
|---|---|---|---|---|---|---|
| Garriga et al. (2020) [36] | Chingford (649) | 48 | KL 8 ≤ 1, JSN < 1 | KL ≥ 2 | Hip α-angle | 0.80 |
| Joseph et al. (2018) [40] | OAI 1 (641, 13%) | 72 | KL ≤ 2 | KL > 2 | KL & KA 13 | 0.67 |
| Janvier et al. (2017) [37] | OAI (319, 13%) | 48 | KL = 0 | ΔJSN 10 ≥ 1 | TBT 14 | 0.73 |
| Janvier et al. (2017) [37] | OAI (319, 13%) | 48 | KL = 0 | ΔKL ≥ 1 | TBT | 0.69 |
| Lazzarini et al. (2017) [14] | PROOF 2 (352,11%) | 30 | KL = 0 | mJSN 11 ≥ 1 mm | NJSASM 15 | 0.74 |
| Lazzarini et al. (2017) [14] | PROOF (352,12%) | 30 | KL = 0 | lJSN 12 ≥ 1 mm | NJSASM | 0.73 |
| Kerkhof et al. (2014) [15] | Rotterdam (2628,18%) | KL ≤ 1 | KL ≥ 2 | KL | 0.79 | |
| Kinds et al. (2012) [38] | CHECK 3 (653, 20%) | 60 | KL ≤ 1 | KL ≥ 2 | JSW 16 & OSTA 17 | 0.69 |
| Woloszynski et al. (2012) [33] | LU 4 (105, 34%) | 48 | KL ≤ 1 | ΔJSN ≥ 1 | TBT | 0.75 |
| Duncan et al. (2011) [34] | CAS-K 5 (253, 22%) | 36 | KL = 0 or 1, PO 9 = 0 | KL ≥ 2 or PO > 0 | TFJOA 18 | - |
| Golightly et al. (2010) [35] | JCO 6 (2734 *, 15%) | 36–156 | KL ≤ 1 | KL ≥ 2 | LLI 19 | - |
| Shamir et al. (2009) [39] | BLSA 7 (123, 32%) | 240 | KL = 0 | KL ≥ 2 | TBT | - |
| Authors (Publication Year, Reference) | Cohort name (number of Subjects, % of cases) | Period (Months) | Inclusion Criterion | Progression Definition | Main Radiographic Biomarkers | AUC |
|---|---|---|---|---|---|---|
| Almhdie-Imjabbar et al. (2022) [41] | OAI 1 (1888, 16%) | 48 | 1 < KL 10 < 4 | ΔmJSN 14 ≥ 0.5 | TBT 16, JSN | 0.75 |
| Almhdie-Imjabbar et al. (2022) [41] | MOST 2 (683, 36%) | 60 | 1 < KL < 4 | ΔmJSN ≥ 0.5 | TBT, JSN | 0.80 |
| Guan et al. (2020) [28] | OAI (1950, 48%) | 48 | 1 < KL < 4 | ΔJSW ≥ 0.7 | KL, CNNf 17 | 0.86 |
| Attur et al. (2020) [42] | OAI (204, 30%) NYU 3 (243, 30%) | 24 | 1 < KL < 4 | ΔmJSN ≥ 0.5 mm | MLOS 18 | 0.67 |
| Tiulpin et al. (2019) [46] | OAI (2711, 27%) MOST (3918, 47%) | 60 | KL ≥ 1 | ΔKL ≥ 1 | KL, CNNf | 0.81 |
| Kraus et al. (2018) [27] | FNIH 4 (579, 32%) | 24–48 | 0 < KL < 4, JSN 11 < 2 | ΔJSW ≥ 0.7 | TBT | 0.65 |
| Janvier et al. (2017) [43] | OAI (1124, 14%) | 48 | 1 < KL < 4 | ΔmJSN ≥ 1 | TBT, JSN | 0.77 |
| Kraus et al. (2013) [45] | Pfizer (58, 36%) | 12–24 | 1 < KL < 4, JSW 12 ≥ 2 mm | ΔJSW ≥ 5% ΔJSA 15 ≥ 5% | TBT | 0.85 |
| Woloszynski et al. (2012) [44] | UWA 5 (50, 24%) | 48 | KL > 1 | ΔmJSN ≥ 1 | TBT | - |
| Woloszynski et al. (2012) [33] | LU 6 (105, 27%) | 48 | KL ≥ 2 | ΔJSN ≥ 1 | TBT | 0.77 |
| Duncan et al. (2011) [34] | CAS-K 7 (91, 25%) | 36 | KL = 2, PO 13 =1 or 2 | KL ≥ 3 or PO = 3 | PFJOA 19 | - |
| Golightly et al. (2010) [35] | JCO 8 (1282 *, 34%) | 36–156 | KL ≥ 1 | ΔKL ≥ 1 | LLI 20 | - |
| Golightly et al. (2010) [35] | JCO (643 *, 27%) | 36–156 | KL ≥ 2 | ΔKL ≥ 1 | LLI | - |
| Kraus et al. (2009) [29] | POP 9 (138, 13%) | 36 | 0 < KL < 4 | ΔmJSN ≥ 1 | TBT, KA 21 | 0.79 |
| Authors (Publication Year, Reference) | Cohort Name (Number of Subjects, % of Cases) | Period (Months) | Inclusion Criterion | Main Radiographic Biomarkers | AUC |
|---|---|---|---|---|---|
| Almhdie-Imjabbar et al. (2022) [51] | OAI 1 (4382, 9%), | 108 | 0 ≤ KL 4 ≤ 4, | TBT 7 & KL & JSN 8 | 0.92 |
| Almhdie-Imjabbar et al. (2022) [51] | OAI (4296, 7%) | 108 | 0 ≤ KL ≤ 3 | TBT 7 & KL & JSN | 0.86 |
| Leung et al. (2020) [50] | OAI (728, 50%) | 108 | 0 ≤ KL ≤ 4 | KL, RNetF 9 | 0.87 |
| Kwoh et al. (2020) [48] | OAI (627, 17%) | 82 | 2 ≤ KL ≤ 3 | JSW | 0.61 |
| Bihlet et al. (2020) [49] | NCT 2 (935, 2%) | 24 | 2 ≤ KL ≤ 3 JSW 5 ≥ 2.0 mm | KL | 0.75 |
| Podsiadlo et al. (2014) [47] | ACHMA 3 (114, 25%) | 72 | 0 ≤ KL ≤ 3 OST 6 ≥ 1 | TBT | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almhdie-Imjabbar, A.; Toumi, H.; Lespessailles, E. Radiographic Biomarkers for Knee Osteoarthritis: A Narrative Review. Life 2023, 13, 237. https://doi.org/10.3390/life13010237
Almhdie-Imjabbar A, Toumi H, Lespessailles E. Radiographic Biomarkers for Knee Osteoarthritis: A Narrative Review. Life. 2023; 13(1):237. https://doi.org/10.3390/life13010237
Chicago/Turabian StyleAlmhdie-Imjabbar, Ahmad, Hechmi Toumi, and Eric Lespessailles. 2023. "Radiographic Biomarkers for Knee Osteoarthritis: A Narrative Review" Life 13, no. 1: 237. https://doi.org/10.3390/life13010237
APA StyleAlmhdie-Imjabbar, A., Toumi, H., & Lespessailles, E. (2023). Radiographic Biomarkers for Knee Osteoarthritis: A Narrative Review. Life, 13(1), 237. https://doi.org/10.3390/life13010237