
Towards a Deep-Learning Approach for Prediction of Fractional Flow Reserve from Optical Coherence Tomography

 , ,
, ,
Abstract
:1. Introduction
- -
- fully connected neural network, commonly referred to as artificial neural networks (ANNs). Potential disadvantages of ANNs are the large number of trainable parameters, which leads to the requirement of large training datasets, and the difficulty in capturing the inherent properties in 1D/2D/3D data structures
- -
- convolutional neural networks (CNNs). Compared to ANNs, CNNs can capture the inherent properties in 1D/2D/3D data structures, but still require relatively large training sets. Also, fixed size input data are required if the network is not fully convolutional.
- -
- recurrent neural networks (RNNs) [34]. RNNs have the advantage that a variable length input sequence can be processed, but they may be affected by vanishing and exploding gradient issues.
2. Materials and Methods
2.1. Data Set
2.1.1. Study Design
2.1.2. Study Population
2.1.3. Procedure Protocol
2.2. Data Pre-Processing
- -
- selection of the proximal start and distal end slice, which define the coronary artery region of interest. Slices representing the catheter are excluded, alongside other slices with sub-optimal image quality (e.g., blood artifacts);
- -
- rejecting/correcting erroneous contours within the selected slice-range: the automatically detected contours may be incorrect on certain slices, typically in bifurcation regions and/or if the lumen has a profoundly non-circular shape (e.g., concave shape). Erroneous bifurcation contours are rejected, while erroneous contours in the stenosis region are corrected (required in less than 10% of the OCT acquisitions).
2.3. Deep Neural Network Based FFR Prediction
- -
- a regression approach: models predict a rational number representing invasive FFR
- -
- a classification approach: models predict the class of the FFR value (positive, i.e., FFR ≤ 0.8, or negative, i.e., FFR > 0.8)
- -
- a FSL approach: similar to the classification approach.
3. Results
3.1. Population Characteristics
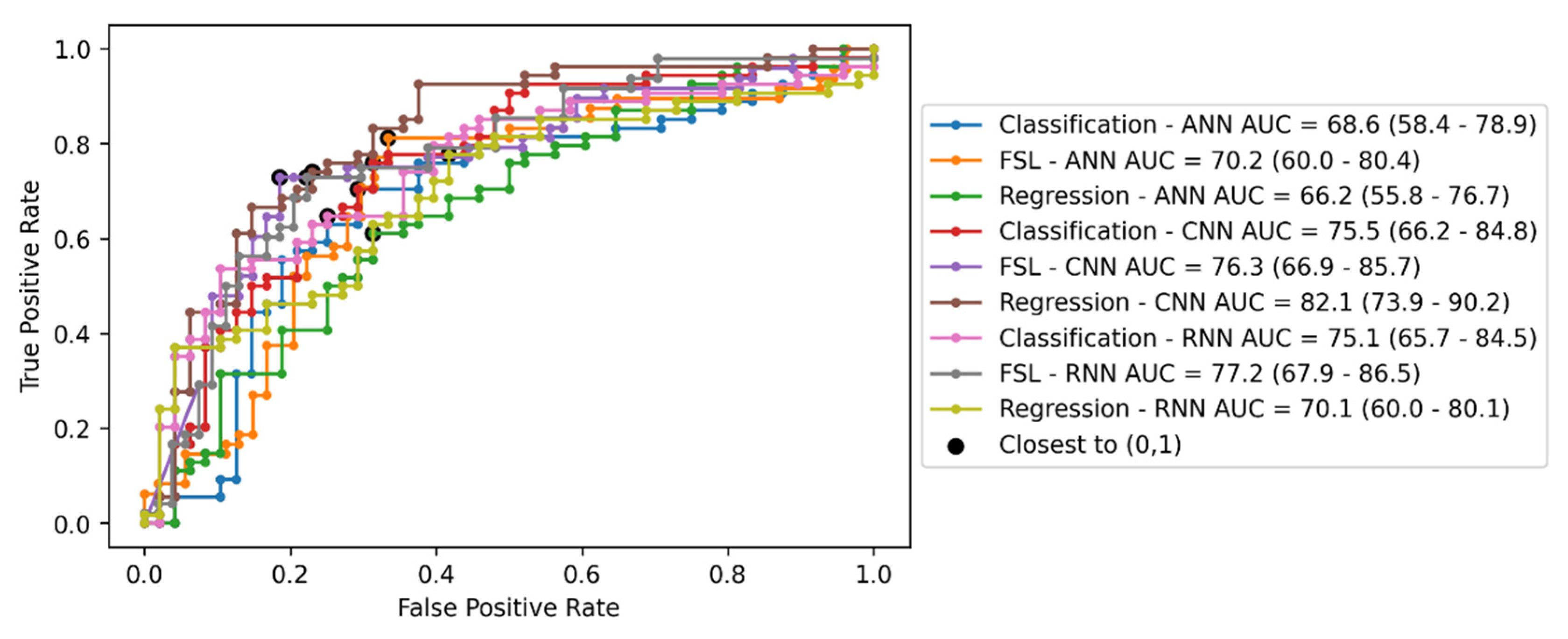
3.2. Invasive FFR Prediction Performance
3.3. Subgroup Analyses
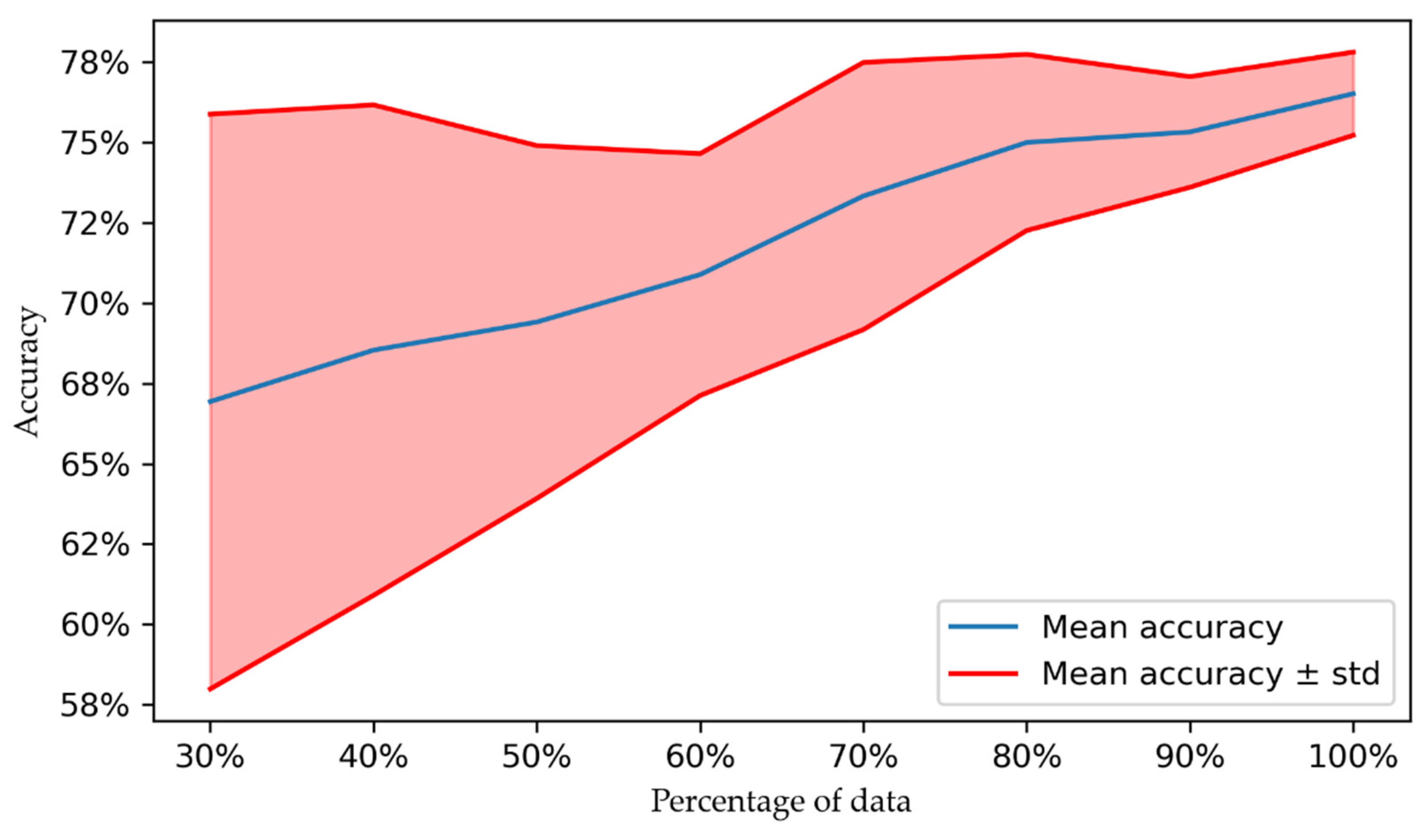
3.4. Effect of Dataset Size
3.5. Saliency Maps and Runtime
4. Discussion and Conclusions
4.1. Deep Learning-Based Prediction of FFR
4.2. Clinical Impact
4.3. Limitations
4.4. Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CVD | Cardiovascular disease |
| CAD | Coronary artery disease |
| XA | X-ray coronary Angiography |
| OCT | Optical coherence tomography |
| PCI Percutaneous coronary intervention | |
| FFR | Fractional flow reserve |
| CABG | Coronary artery bypass graft |
| CFG | Computational fluid dynamics |
| CCTA | Coronary computed tomography angiography |
| ML | Machine Learning |
| IVUS | Intravascular ultrasound |
| DNN | Deep neural network |
| DL | Deep learning |
| ANN | Artificial neural network |
| CNN | Convolutional neural network |
| RNN | Recurrent neural network |
| FSL | Few-shot learning |
| ReLU | Rectified linear unit |
| GRU | Gated recurrent unit |
| MLD | Minimum lumen diameter |
| %DS | Percentage diameter stenosis |
| NPV | Negative predictive value |
| PPV | Positive predictive value |
| MAE | Mean absolute error |
| ME | Mean error |
| MSE | Mean squared error |
| LAD | Left Anterior Descending artery |
| LCx | Left Circumflex artery |
| RCA | Right Coronary Artery |
| Arch. | Architecture |
| Corr. | Correlation |
| TP | True positive |
| TN | True negative |
| FP | False positive |
| FN | False negative |
| CFR | Coronary flow reserve |
| iFR | Instantaneous wave-free ratio |
| HSR | Hyperemic stenosis resistance |
| BSR | Basal stenosis resistance |
| FC | Fully connected |
| BCE | Binary cross entropy |
| FoV | Field of view |
Appendix A.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Index | Layer | Input Features | Output Features | Activation Function | Regularization |
|---|---|---|---|---|---|
| 1 | FC | 376 | 32 | ReLU | - |
| 2 | FC | 32 | 64 | ReLU | - |
| 3 | FC | 64 | 128 | ReLU | - |
| 4 | FC | 128 | 256 | ReLU | Dropout |
| 5 | FC | 256 | 1 | Sigmoid | - |
| Layer Index | Layer | Kernel Size | Input Channels | Output Channels | Stride | Activation Function | Regularization | Normalization | Receptive FoV |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Conv1D | 3 | 1 | 64 | 2 | ReLU | - | Batch norm | 3 |
| 2 | Conv1D | 3 | 64 | 128 | 2 | ReLU | - | Batch norm | 7 |
| 3 | Conv1D | 3 | 128 | 256 | 2 | ReLU | - | Batch norm | 15 |
| 4 | Conv1D | 3 | 256 | 512 | 2 | ReLU | - | Batch norm | 31 |
| 5 | Conv1D | 3 | 512 | 512 | 2 | ReLU | - | Batch norm | 63 |
| 6 | Conv1D | 3 | 512 | 512 | 1 | ReLU | - | Batch norm | 127 |
| 7 | Conv1D | 3 | 512 | 512 | 1 | ReLU | - | Batch norm | 191 |
| 8 | Conv1D | 3 | 512 | 512 | 1 | ReLU | - | Batch norm | 255 |
| Layer | Input Features | Output Features | Activation | Regularization |
|---|---|---|---|---|
| FC | 2048 | 1024 | ReLU | Dropout |
| FC | 1024 | 1 | Sigmoid | - |
| Layer | Input Features | Hidden Size | Output Features | Activation | Regularization |
|---|---|---|---|---|---|
| Bidirectional GRU | 512 | 512 | 1024 | - | Dropout |
| FC | 1024 | - | 1 | Sigmoid | - |
Appendix A.1. Prototypical Networks
Appendix A.2. Loss Functions
References
- Ryan, T.J. The coronary angiogram and its seminal contributions to cardiovascular medicine over five decades. Circulation 2002, 106, 752–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez-Chico, J.L.; Alegría-Barrero, E.; Teijeiro-Mestre, R.; Chan, P.H.; Tsujioka, H.; de Silva, R.; Viceconte, N.; Lindsay, A.; Patterson, T.; Foin, N. Optical coherence tomography: From research to practice. Eur. Heart J.-Cardiovasc. Imaging 2012, 13, 370–384. [Google Scholar] [CrossRef]
- Gutiérrez-Chico, J.L.; Regar, E.; Nüesch, E.; Okamura, T.; Wykrzykowska, J.; di Mario, C.; Windecker, S.; van Es, G.-A.; Gobbens, P.; Jüni, P. Delayed coverage in malapposed and side-branch struts with respect to well-apposed struts in drug-eluting stents: In vivo assessment with optical coherence tomography. Circulation 2011, 124, 612–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Chico, J.L.; Wykrzykowska, J.; Nüesch, E.; van Geuns, R.J.; Koch, K.T.; Koolen, J.J.; di Mario, C.; Windecker, S.; van Es, G.-A.; Gobbens, P. Vascular tissue reaction to acute malapposition in human coronary arteries: Sequential assessment with optical coherence tomography. Circ. Cardiovasc. Interv. 2012, 5, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, Z.A.; Maehara, A.; Généreux, P.; Shlofmitz, R.A.; Fabbiocchi, F.; Nazif, T.M.; Guagliumi, G.; Meraj, P.M.; Alfonso, F.; Samady, H. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): A randomised controlled trial. Lancet 2016, 388, 2618–2628. [Google Scholar] [CrossRef]
- Gonzalo, N.; Escaned, J.; Alfonso, F.; Nolte, C.; Rodriguez, V.; Jimenez-Quevedo, P.; Bañuelos, C.; Fernández-Ortiz, A.; Garcia, E.; Hernandez-Antolin, R. Morphometric assessment of coronary stenosis relevance with optical coherence tomography: A comparison with fractional flow reserve and intravascular ultrasound. J. Am. Coll. Cardiol. 2012, 59, 1080–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pijls, N.H.; de Bruyne, B.; Peels, K.; van der Voort, P.H.; Bonnier, H.J.; Bartunek, J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; vant Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [Green Version]
- Tu, S.; Bourantas, C.V.; Nørgaard, B.L.; Kassab, G.S.; Koo, B.K.; Reiber, J. Image-based assessment of fractional flow reserve. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2015, 11, V50–V54. [Google Scholar] [CrossRef]
- Yang, D.H.; Kim, Y.-H.; Roh, J.H.; Kang, J.-W.; Ahn, J.-M.; Kweon, J.; Lee, J.B.; Choi, S.H.; Shin, E.-S.; Park, D.-W. Diagnostic performance of on-site CT-derived fractional flow reserve versus CT perfusion. Eur. Heart J.-Cardiovasc. Imaging 2017, 18, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Coenen, A.; Lubbers, M.M.; Kurata, A.; Kono, A.; Dedic, A.; Chelu, R.G.; Dijkshoorn, M.L.; Gijsen, F.J.; Ouhlous, M.; van Geuns, R.-J.M. Fractional flow reserve computed from noninvasive CT angiography data: Diagnostic performance of an on-site clinician-operated computational fluid dynamics algorithm. Radiology 2015, 274, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Renker, M.; Schoepf, U.J.; Wang, R.; Meinel, F.G.; Rier, J.D.; Bayer II, R.R.; Möllmann, H.; Hamm, C.W.; Steinberg, D.H.; Baumann, S. Comparison of diagnostic value of a novel noninvasive coronary computed tomography angiography method versus standard coronary angiography for assessing fractional flow reserve. Am. J. Cardiol. 2014, 114, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.-K.; Erglis, A.; Doh, J.-H.; Daniels, D.V.; Jegere, S.; Kim, H.-S.; Dunning, A.; DeFrance, T.; Lansky, A.; Leipsic, J. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms: Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J. Am. Coll. Cardiol. 2011, 58, 1989–1997. [Google Scholar]
- Tu, S.; Westra, J.; Yang, J.; von Birgelen, C.; Ferrara, A.; Pellicano, M.; Nef, H.; Tebaldi, M.; Murasato, Y.; Lansky, A. Diagnostic accuracy of fast computational approaches to derive fractional flow reserve from diagnostic coronary angiography: The international multicenter FAVOR pilot study. Cardiovasc. Interv. 2016, 9, 2024–2035. [Google Scholar]
- Tröbs, M.; Achenbach, S.; Röther, J.; Redel, T.; Scheuering, M.; Winneberger, D.; Klingenbeck, K.; Itu, L.; Passerini, T.; Kamen, A. Comparison of fractional flow reserve based on computational fluid dynamics modeling using coronary angiographic vessel morphology versus invasively measured fractional flow reserve. Am. J. Cardiol. 2016, 117, 29–35. [Google Scholar] [CrossRef]
- Papafaklis, M.I.; Muramatsu, T.; Ishibashi, Y.; Lakkas, L.S.; Nakatani, S.; Bourantas, C.V.; Ligthart, J.; Onuma, Y.; Echavarria-Pinto, M.; Tsirka, G. Fast virtual functional assessment of intermediate coronary lesions using routine angiographic data and blood flow simulation in humans: Comparison with pressure wire-fractional flow reserve. EuroIntervention 2014, 10, 574–583. [Google Scholar] [CrossRef]
- Tu, S.; Barbato, E.; Köszegi, Z.; Yang, J.; Sun, Z.; Holm, N.R.; Tar, B.; Li, Y.; Rusinaru, D.; Wijns, W. Fractional flow reserve calculation from 3-dimensional quantitative coronary angiography and TIMI frame count: A fast computer model to quantify the functional significance of moderately obstructed coronary arteries. JACC Cardiovasc. Interv. 2014, 7, 768–777. [Google Scholar] [CrossRef] [Green Version]
- Morris, P.D.; Ryan, D.; Morton, A.C.; Lycett, R.; Lawford, P.V.; Hose, D.R.; Gunn, J.P. Virtual fractional flow reserve from coronary angiography: Modeling the significance of coronary lesions: Results from the VIRTU-1 (VIRTUal Fractional Flow Reserve From Coronary Angiography) study. JACC Cardiovasc. Interv. 2013, 6, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seike, F.; Uetani, T.; Nishimura, K.; Kawakami, H.; Higashi, H.; Aono, J.; Nagai, T.; Inoue, K.; Suzuki, J.; Kawakami, H. Intracoronary optical coherence tomography-derived virtual fractional flow reserve for the assessment of coronary artery disease. Am. J. Cardiol. 2017, 120, 1772–1779. [Google Scholar] [CrossRef]
- Jang, S.-J.; Ahn, J.-M.; Kim, B.; Gu, J.-M.; Sung, H.J.; Park, S.-J.; Oh, W.-Y. Comparison of accuracy of one-use methods for calculating fractional flow reserve by intravascular optical coherence tomography to that determined by the pressure-wire method. Am. J. Cardiol. 2017, 120, 1920–1925. [Google Scholar] [CrossRef]
- Yu, W.; Huang, J.; Jia, D.; Chen, S.; Raffel, O.C.; Ding, D.; Tian, F.; Kan, J.; Zhang, S.; Yan, F. Diagnostic accuracy of intracoronary optical coherence tomography-derived fractional flow reserve for assessment of coronary stenosis severity. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2019, 15, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, J.; Kim, J.-S.; Lim, J.; Kim, G.; Lee, S.; Lee, J.S.; Shin, D.-H.; Kim, B.-K.; Ko, Y.-G.; Choi, D. Assessing computational fractional flow reserve from optical coherence tomography in patients with intermediate coronary stenosis in the left anterior descending artery. Circ. Cardiovasc. Interv. 2016, 9, e003613. [Google Scholar] [CrossRef] [PubMed]
- Itu, L.; Sharma, P.; Mihalef, V.; Kamen, A.; Suciu, C.; Lomaniciu, D. A patient-specific reduced-order model for coronary circulation. In Proceedings of the 2012 9th IEEE International Symposium on Biomedical Imaging (ISBI), Barcelona, Spain, 2–5 May 2012; pp. 832–835. [Google Scholar]
- Deng, S.-B.; Jing, X.-D.; Wang, J.; Huang, C.; Xia, S.; Du, J.-L.; Liu, Y.-J.; She, Q. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in coronary artery disease: A systematic review and meta-analysis. Int. J. Cardiol. 2015, 184, 703–709. [Google Scholar] [CrossRef]
- Bishop, C.M.; Nasrabadi, N.M. Pattern Recognition and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2006; Volume 4. [Google Scholar]
- Zheng, Y.; Comaniciu, D. Marginal Space Learning for Medical Image Analysis; Springer: Berlin/Heidelberg, Germany, 2014; Volume 2, p. 6. [Google Scholar]
- Mansi, T.; Georgescu, B.; Hussan, J.; Hunter, P.J.; Kamen, A.; Comaniciu, D. Data-driven reduction of a cardiac myofilament model. In Proceedings of the International Conference on Functional Imaging and Modeling of the Heart, London, UK, 20–22 June 2013; pp. 232–240. [Google Scholar]
- Tøndel, K.; Indahl, U.G.; Gjuvsland, A.B.; Vik, J.O.; Hunter, P.; Omholt, S.W.; Martens, H. Hierarchical Cluster-based Partial Least Squares Regression (HC-PLSR) is an efficient tool for metamodelling of nonlinear dynamic models. BMC Syst. Biol. 2011, 5, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itu, L.; Rapaka, S.; Passerini, T.; Georgescu, B.; Schwemmer, C.; Schoebinger, M.; Flohr, T.; Sharma, P.; Comaniciu, D. A machine-learning approach for computation of fractional flow reserve from coronary computed tomography. J. Appl. Physiol. 2016, 121, 42–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.; Lee, J.G.; Kang, S.J.; Kim, W.J.; Choi, S.Y.; Ko, J.; Min, H.S.; Choi, G.H.; Kang, D.Y.; Lee, P.H. Angiography-based machine learning for predicting fractional flow reserve in intermediate coronary artery lesions. J. Am. Heart Assoc. 2019, 8, e011685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, J.-J.; Son, T.D.; Ha, J.; Kim, J.-S.; Hong, S.-J.; Ahn, C.-M.; Kim, B.-K.; Ko, Y.-G.; Choi, D.; Hong, M.-K. Optical coherence tomography-based machine learning for predicting fractional flow reserve in intermediate coronary stenosis: A feasibility study. Sci. Rep. 2020, 10, 20421. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-G.; Ko, J.; Hae, H.; Kang, S.-J.; Kang, D.-Y.; Lee, P.H.; Ahn, J.-M.; Park, D.-W.; Lee, S.-W.; Kim, Y.-H. Intravascular ultrasound-based machine learning for predicting fractional flow reserve in intermediate coronary artery lesions. Atherosclerosis 2020, 292, 171–177. [Google Scholar] [CrossRef]
- Deng, L.; Yu, D. Deep learning: Methods and applications. Found. Trends Signal Processing 2014, 7, 197–387. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Wang, Y.; Yao, Q.; Kwok, J.T.; Ni, L.M. Generalizing from a few examples: A survey on few-shot learning. ACM Comput. Surv. 2020, 53, 1–34. [Google Scholar] [CrossRef]
- Jiang, X.; Zeng, Y.; Xiao, S.; He, S.; Ye, C.; Qi, Y.; Zhao, J.; Wei, D.; Hu, M.; Chen, F. Automatic detection of coronary metallic stent struts based on YOLOv3 and R-FCN. Comput. Math. Methods Med. 2020, 2020, 1793517. [Google Scholar] [CrossRef]
- Wang, Z.; Jenkins, M.W.; Linderman, G.C.; Bezerra, H.G.; Fujino, Y.; Costa, M.A.; Wilson, D.L.; Rollins, A.M. 3-D stent detection in intravascular OCT using a Bayesian network and graph search. IEEE Trans. Med. Imaging 2015, 34, 1549–1561. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Gutiérrez-Chico, J.L.; Tauzin, H.; Yang, W.; Li, Y.; Yu, W.; Chu, M.; Guillon, B.; Bai, J.; Meneveau, N. Automatic stent reconstruction in optical coherence tomography based on a deep convolutional model. Biomed. Opt. Express 2020, 11, 3374–3394. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Mehanna, E.; Li, C.; Zhu, H.; He, C.; Lu, F.; Zhao, K.; Gong, Y.; Wang, Z. Stent detection with very thick tissue coverage in intravascular OCT. Biomed. Opt. Express 2021, 12, 7500–7516. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.S.; Tan, L.K.; Chan, C.K.; Chee, K.H.; Liew, Y.M. Automated segmentation of metal stent and bioresorbable vascular scaffold in intravascular optical coherence tomography images using deep learning architectures. Phys. Med. Biol. 2021, 66, 245026. [Google Scholar] [CrossRef]
- Lee, J.; Gharaibeh, Y.; Kolluru, C.; Zimin, V.N.; Dallan, L.A.P.; Kim, J.N.; Bezerra, H.G.; Wilson, D.L. Segmentation of Coronary Calcified Plaque in Intravascular OCT Images Using a Two-Step Deep Learning Approach. IEEE Access 2020, 8, 225581–225593. [Google Scholar] [CrossRef]
- Gharaibeh, Y.; Prabhu, D.S.; Kolluru, C.; Lee, J.; Zimin, V.; Bezerra, H.G.; Wilson, D.L. Coronary calcification segmentation in intravascular OCT images using deep learning: Application to calcification scoring. J. Med. Imaging 2019, 6, 045002. [Google Scholar] [CrossRef] [Green Version]
- Abdolmanafi, A.; Duong, L.; Ibrahim, R.; Dahdah, N. A deep learning-based model for characterization of atherosclerotic plaque in coronary arteries using optical coherence tomography images. Med. Phys. 2021, 48, 3511–3524. [Google Scholar] [CrossRef]
- Pociask, E.; Malinowski, K.P.; Ślęzak, M.; Jaworek-Korjakowska, J.; Wojakowski, W.; Roleder, T. Fully automated lumen segmentation method for intracoronary optical coherence tomography. J. Healthc. Eng. 2018, 2018, 1414076. [Google Scholar] [CrossRef] [Green Version]
- Jiao, C.; Xu, Z.; Bian, Q.; Forsberg, E.; Tan, Q.; Peng, X.; He, S. Machine learning classification of origins and varieties of Tetrastigma hemsleyanum using a dual-mode microscopic hyperspectral imager. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 261, 120054. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Shen, F.; Deng, H.; Cai, F.; Chen, S. Smartphone imaging spectrometer for egg/meat freshness monitoring. Anal. Methods 2022, 14, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Snell, J.; Swersky, K.; Zemel, R. Prototypical networks for few-shot learning. Adv. Neural Inf. Processing Syst. 2017, 30. [Google Scholar]
- Kern, M.J.; Lerman, A.; Bech, J.-W.; De Bruyne, B.; Eeckhout, E.; Fearon, W.F.; Higano, S.T.; Lim, M.J.; Meuwissen, M.; Piek, J.J. Physiological assessment of coronary artery disease in the cardiac catheterization laboratory: A scientific statement from the American Heart Association Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology. Circulation 2006, 114, 1321–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradski, G. The openCV library. Dr. Dobb’s J. Softw. Tools Prof. Program. 2000, 25, 120–123. [Google Scholar]
- Patro, S.; Sahu, K.K. Normalization: A preprocessing stage. arXiv 2015, arXiv:1503.06462. [Google Scholar] [CrossRef]
- Agarap, A.F. Deep learning using rectified linear units (relu). arXiv 2018, arXiv:1803.08375. [Google Scholar]
- Santurkar, S.; Tsipras, D.; Ilyas, A.; Madry, A. How does batch normalization help optimization? Adv. Neural Inf. Processing Syst. 2018, 31. [Google Scholar]
- Dey, R.; Salem, F.M. Gate-variants of gated recurrent unit (GRU) neural networks. In Proceedings of the 2017 IEEE 60th International Midwest Symposium on Circuits and Systems (MWSCAS), Boston, MA, USA, 6–9 August 2017; pp. 1597–1600. [Google Scholar]
- Han, J.; Moraga, C. The influence of the sigmoid function parameters on the speed of backpropagation learning. In Proceedings of the International Workshop on Artificial Neural Networks, Malaga-Torremolinos, Spain, 7–9 June 1995; pp. 195–201. [Google Scholar]
- Wong, T.-T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Zhang, Z. Improved adam optimizer for deep neural networks. In Proceedings of the 2018 IEEE/ACM 26th International Symposium on Quality of Service (IWQoS), Banff, AB, Canada, 4–6 June 2018; pp. 1–2. [Google Scholar]
- Kline, D.M.; Berardi, V.L. Revisiting squared-error and cross-entropy functions for training neural network classifiers. Neural Comput. Appl. 2005, 14, 310–318. [Google Scholar] [CrossRef]
- Liashchynskyi, P.; Liashchynskyi, P. Grid search, random search, genetic algorithm: A big comparison for NAS. arXiv 2019, arXiv:1912.06059. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Processing Syst. 2019, 32. [Google Scholar]
- Hoo, Z.H.; Candlish, J.; Teare, D. What is an ROC curve? Emerg. Med. J. 2017, 34, 357–359. [Google Scholar] [CrossRef] [PubMed]
- Lobo, J.M.; Jiménez-Valverde, A.; Real, R. AUC: A misleading measure of the performance of predictive distribution models. Glob. Ecol. Biogeogr. 2008, 17, 145–151. [Google Scholar] [CrossRef]
- Unal, I. Defining an optimal cut-point value in ROC analysis: An alternative approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Wong, H.B.; Lim, G.H. Measures of diagnostic accuracy: Sensitivity, specificity, PPV and NPV. Proc. Singap. Healthc. 2011, 20, 316–318. [Google Scholar] [CrossRef]
- Genders, T.S.; Spronk, S.; Stijnen, T.; Steyerberg, E.W.; Lesaffre, E.; Hunink, M.M. Methods for calculating sensitivity and specificity of clustered data: A tutorial. Radiology 2012, 265, 910–916. [Google Scholar] [CrossRef]
- Lakshminarayanan, B.; Pritzel, A.; Blundell, C. Simple and scalable predictive uncertainty estimation using deep ensembles. Adv. Neural Inf. Processing Syst. 2017, 30. [Google Scholar]
- Wieneke, H.; Von Birgelen, C.; Haude, M.; Eggebrecht, H.; Mohlenkamp, S.; Schmermund, A.; Bose, D.; Altmann, C.; Bartel, T.; Erbel, R. Determinants of coronary blood flow in humans: Quantification by intracoronary Doppler and ultrasound. J. Appl. Physiol. 2005, 98, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, Y.; Johnson, N.P.; Berry, C.; De Bruyne, B.; Gould, K.L.; Jeremias, A.; Oldroyd, K.G.; Pijls, N.H.; Fearon, W.F.; Investigators, C.S. The influence of lesion location on the diagnostic accuracy of adenosine-free coronary pressure wire measurements. JACC Cardiovasc. Interv. 2016, 9, 2390–2399. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Vedaldi, A.; Zisserman, A. Deep inside convolutional networks: Visualising image classification models and saliency maps. arXiv 2013, arXiv:1312.6034. [Google Scholar]
- Bote-Curiel, L.; Munoz-Romero, S.; Gerrero-Curieses, A.; Rojo-Álvarez, J.L. Deep learning and big data in healthcare: A double review for critical beginners. Appl. Sci. 2019, 9, 2331. [Google Scholar] [CrossRef] [Green Version]
- Demir-Kavuk, O.; Kamada, M.; Akutsu, T.; Knapp, E.-W. Prediction using step-wise L1, L2 regularization and feature selection for small data sets with large number of features. BMC Bioinform. 2011, 12, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Wong, S.C.; Gatt, A.; Stamatescu, V.; McDonnell, M.D. Understanding data augmentation for classification: When to warp? In Proceedings of the 2016 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Gold Coast, Australia, 30 November–2 December 2016; pp. 1–6. [Google Scholar]
- Kumamaru, K.K.; Fujimoto, S.; Otsuka, Y.; Kawasaki, T.; Kawaguchi, Y.; Kato, E.; Takamura, K.; Aoshima, C.; Kamo, Y.; Kogure, Y. Diagnostic accuracy of 3D deep-learning-based fully automated estimation of patient-level minimum fractional flow reserve from coronary computed tomography angiography. Eur. Heart J.-Cardiovasc. Imaging 2020, 21, 437–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zreik, M.; van Hamersvelt, R.W.; Khalili, N.; Wolterink, J.M.; Voskuil, M.; Viergever, M.A.; Leiner, T.; Išgum, I. Deep learning analysis of coronary arteries in cardiac CT angiography for detection of patients requiring invasive coronary angiography. IEEE Trans. Med. Imaging 2019, 39, 1545–1557. [Google Scholar] [CrossRef] [Green Version]
- Petraco, R.; Park, J.J.; Sen, S.; Nijjer, S.; Malik, I.; Pinto, M.E.; Asrress, K.; Nam, C.W.; Foale, R.; Sethi, A. Hybrid iFR-FFR decision-making strategy: Implications for enhancing universal adoption of physiology-guided coronary revascularization. Am. J. Cardiol. 2013, 111, 54B. [Google Scholar] [CrossRef]
- Guo, X.; Tang, D.; Molony, D.; Yang, C.; Samady, H.; Zheng, J.; Mintz, G.S.; Maehara, A.; Wang, L.; Pei, X. A machine learning-based method for intracoronary oct segmentation and vulnerable coronary plaque cap thickness quantification. Int. J. Comput. Methods 2019, 16, 1842008. [Google Scholar] [CrossRef]
- Lyras, K.G.; Lee, J. An improved reduced-order model for pressure drop across arterial stenoses. PLoS ONE 2021, 16, e0258047. [Google Scholar] [CrossRef]
- Gutiérrez-Chico, J.L.; Chen, Y.; Yu, W.; Ding, D.; Huang, J.; Huang, P.; Jing, J.; Chu, M.; Wu, P.; Tian, F. Diagnostic accuracy and reproducibility of optical flow ratio for functional evaluation of coronary stenosis in a prospective series. Cardiol. J. 2020, 27, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Georgousis, S.; Kenning, M.P.; Xie, X. Graph deep learning: State of the art and challenges. IEEE Access 2021, 9, 22106–22140. [Google Scholar] [CrossRef]
- Kern, M.J. Coronary physiology revisited: Practical insights from the cardiac catheterization laboratory. Circulation 2000, 101, 1344–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, S.; Escaned, J.; Malik, I.S.; Mikhail, G.W.; Foale, R.A.; Mila, R.; Tarkin, J.; Petraco, R.; Broyd, C.; Jabbour, R. Development and validation of a new adenosine-independent index of stenosis severity from coronary wave–intensity analysis: Results of the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study. J. Am. Coll. Cardiol. 2012, 59, 1392–1402. [Google Scholar] [CrossRef] [Green Version]
- Meuwissen, M.; Siebes, M.; Chamuleau, S.A.; van Eck-Smit, B.L.; Koch, K.T.; de Winter, R.J.; Tijssen, J.G.; Spaan, J.A.; Piek, J.J. Hyperemic stenosis resistance index for evaluation of functional coronary lesion severity. Circulation 2002, 106, 441–446. [Google Scholar] [CrossRef] [Green Version]
- van de Hoef, T.P.; Nolte, F.; Damman, P.; Delewi, R.; Bax, M.; Chamuleau, S.A.; Voskuil, M.; Siebes, M.; Tijssen, J.G.; Spaan, J.A. Diagnostic accuracy of combined intracoronary pressure and flow velocity information during baseline conditions: Adenosine-free assessment of functional coronary lesion severity. Circ. Cardiovasc. Interv. 2012, 5, 508–514. [Google Scholar] [CrossRef] [Green Version]





| Male | 66 (82%) |
| Female | 14 (18%) |
| Age (years) | 60.5 ± 11.2 years |
| Race | All Caucasian |
| Weight | 81.93 ± 16.15 kg |
| Height | 172.13 ± 8.05 cm |
| Diabetes | 27 (33.75%) |
| Hypertension | 60 (75%) |
| Hypercholesterolemia | 62 (77.5%) |
| Smoking history | 42 (52.5%) |
| Family history of CAD | 3 (2.9%) |
| Previous myocardial infarction | 46 (45%) |
| Previous Angina | 64 (80%) |
| Ejection fraction | 48.28 ± 6.31% |
| Index Artery | |
|---|---|
| Left Anterior Descending artery (LAD) | 57 |
| Left Circumflex artery (LCx) | 20 |
| Right Coronary Artery (RCA) | 25 |
| Fractional Flow Reserve | |
| Mean ± SD | 0.80 ± 0.08 |
| Median (IQR) | 0.83 (0.75−0.86) |
| FFR ≤ 0.80 | 48 |
| FFR < 0.75 | 25 |
| 0.75 ≤ FFR ≤ 0.85 | 47 |
| FFR > 0.85 | 30 |
| Validation | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approach | Ensemble Arch. | Train_Accuracy [%] | Accuracy [%] | Sensitivity [%] | Specificity [%] | NPV [%] | PPV [%] | AUC [%] | MAE | ME | MSE | Corr. |
| Regression | ANN | 73.7 | 64.7 (55.1–73.3) | 61.1 (47.8–80.1) | 68.8 (54.7–80.1) | 61.1 (47.8–73.0) | 68.8 (54.7–80.1) | 66.2 (55.8–76.7) | 0.062 | 0.007 | 0.105 | 0.273 |
| CNN | 85.9 | 75.5 (66.3–82.8) | 74.1 (61.1–86.7) | 77.1 (63.5–86.7) | 72.5 (59.1–82.9) | 78.4 (65.4–87.5) | 82.1 (73.9–90.2) | 0.082 | −0.008 | 0.015 | 0.342 | |
| RNN | 69.7 | 68.6 (59.1–76.8) | 77.8 (65.1–71.2) | 58.3 (44.3–71.2) | 70.0 (54.6–81.9) | 67.7 (55.4–78.0) | 70.1 (60–80.1) | 0.072 | 0.022 | 0.011 | 0.261 | |
| Classification | ANN | 78.4 | 70.6 (61.1–78.6) | 70.4 (57.2–81.8) | 70.8 (56.8–81.8) | 68.0 (54.2–79.2) | 73.1 (59.7–83.2) | 68.6 (58.4–78.9) | - | - | - | - |
| CNN | 98.7 | 72.5 (63.2–80.3) | 75.9 (63.1–80.1) | 68.8 (54.7–80.1) | 71.7 (57.5–82.7) | 73.2 (60.4–83.0) | 75.5 (66.2–84.8) | - | - | - | - | |
| RNN | 73.8 | 69.6 (60.1–77.7) | 64.8 (51.5–85.1) | 75.0 (61.2–85.1) | 65.5 (52.3–76.6) | 74.5 (60.5–84.7) | 75.1 (65.7–74.5) | - | - | - | - | |
| FSL | ANN | 78.9 | 72.5 (63.2–80.3) | 79.2 (65.7–77.8) | 66.7 (53.4–77.8) | 78.3 (64.4–87.7) | 67.9 (54.8–78.6) | 70.2 (60–80.4) | - | - | - | - |
| CNN | 78.6 | 77.5 (68.4–84.5) | 72.9 (59.0–89.6) | 81.5 (69.2–89.6) | 77.2 (64.8–86.2) | 77.8 (63.7–87.5) | 76.3 (66.9–85.7) | - | - | - | - | |
| RNN | 75.6 | 75.5 (66.3–82.8) | 72.9 (59.0–86.8) | 77.8 (65.1–86.8) | 76.4 (63.7–85.6) | 74.5 (60.5–84.7) | 77.2 (60–80.1) | - | - | - | - | |
| Predicted Values | Actual Values | ||
| Positive (1) | Negative (0) | ||
| Positive (1) | 35 | 13 | |
| Negative (0) | 11 | 44 | |
| Accuracy | ||||||
|---|---|---|---|---|---|---|
| Approach | Ensemble Arch. | Mean [%] | Std [%] | Min [%] | Max [%] | Uncertainty [%] |
| Regression | ANN | 61.57 | 4.55 | 53.92 | 70.59 | 4.48 |
| CNN | 61.76 | 2.65 | 55.88 | 65.69 | 12.91 | |
| RNN | 63.19 | 3.82 | 54.9 | 71.57 | 2.25 | |
| Classification | ANN | 68.43 | 1.69 | 65.69 | 72.55 | 32.55 |
| CNN | 67.75 | 3.1 | 63.73 | 73.53 | 32.9 | |
| RNN | 68.04 | 1.71 | 64.71 | 71.57 | 31.69 | |
| FSL | ANN | 66.67 | 3.34 | 59.8 | 72.55 | 30.9 |
| CNN | 75.59 | 1.2 | 72.55 | 76.47 | 2.77 | |
| RNN | 74.46 | 1.37 | 71.57 | 76.47 | 34.71 | |
| FFR Interval | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| FFR > 0.85 | 86.6 (70.3–94.6) | N/A | 86.6 (70.3–94.6) |
| 0.75–0.85 | 68.0 (53.8–79.6) | 60.8 (40.7–77.8) | 75.0 (55.1–88.0) |
| FFR < 0.75 | 84.0 (65.3–93.6) | 84.0 (65.3–93.6) | N/A |
| Coronary Artery | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| LAD | 75.4 (62.8–84.7) | 76.4 (60.0–87.5) | 73.9 (53.5–87.4) |
| LCX | 85.0 (58.3–91.9) | 80.0 (37.5–96.3) | 86.6 (54.8–92.9) |
| RCA | 76.0 (56.5–88.5) | 55.5 (26.6–81.1) | 87.5 (63.9–96.5) |
| LAD Lesions Location | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| proximal LAD | 74.1 (56.7–86.2) | 70.5 (46.8–86.7) | 78.5 (52.4–92.4) |
| mid/distal LAD | 76.9 (57.9−88.9) | 82.3 (58.9–93.8) | 66.6 (35.4–87.9) |
| Gender | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| Male | 78.8 (67.7–85.1) | 73.8 (58.9–84.6) | 83.7 (67.3–90.2) |
| Female | 70.5 (46.8–86.7) | 66.6 (29.9–90.3) | 72.7 (43.4–90.2) |
| Age Interval | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| <58 | 81.2 (64.6–91.1) | 75.0 (53.2–88.8) | 91.6 (64.6–98.5) |
| 58–66 | 69.2 (50.9–79.3) | 60.0 (35.7–80.1) | 75.0 (50.8–85.0) |
| >66 | 83.8 (67.3–92.9) | 84.6 (57.7–95.6) | 83.3 (60.7–94.1) |
| Vessel Length [cm] | Accuracy [%] | Sensitivity [%] | Specificity [%] |
|---|---|---|---|
| <4.74 | 77.1 (57.9–85.8) | 53.8 (29.1–76.7) | 90.9 (66.6–92.5) |
| 4.74–5.74 | 75.0 (57.8–86.7) | 78.5 (52.4–92.4) | 72.2 (49.1–87.5) |
| >5.74 | 79.4 (63.2–89.6) | 80.9 (59.9–92.3) | 76.9 (49.7–91.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatfaludi, C.-A.; Tache, I.-A.; Ciușdel, C.F.; Puiu, A.; Stoian, D.; Itu, L.M.; Calmac, L.; Popa-Fotea, N.-M.; Bataila, V.; Scafa-Udriste, A. Towards a Deep-Learning Approach for Prediction of Fractional Flow Reserve from Optical Coherence Tomography. Appl. Sci. 2022, 12, 6964. https://doi.org/10.3390/app12146964
Hatfaludi C-A, Tache I-A, Ciușdel CF, Puiu A, Stoian D, Itu LM, Calmac L, Popa-Fotea N-M, Bataila V, Scafa-Udriste A. Towards a Deep-Learning Approach for Prediction of Fractional Flow Reserve from Optical Coherence Tomography. Applied Sciences. 2022; 12(14):6964. https://doi.org/10.3390/app12146964
Chicago/Turabian StyleHatfaludi, Cosmin-Andrei, Irina-Andra Tache, Costin Florian Ciușdel, Andrei Puiu, Diana Stoian, Lucian Mihai Itu, Lucian Calmac, Nicoleta-Monica Popa-Fotea, Vlad Bataila, and Alexandru Scafa-Udriste. 2022. "Towards a Deep-Learning Approach for Prediction of Fractional Flow Reserve from Optical Coherence Tomography" Applied Sciences 12, no. 14: 6964. https://doi.org/10.3390/app12146964
APA StyleHatfaludi, C. -A., Tache, I. -A., Ciușdel, C. F., Puiu, A., Stoian, D., Itu, L. M., Calmac, L., Popa-Fotea, N. -M., Bataila, V., & Scafa-Udriste, A. (2022). Towards a Deep-Learning Approach for Prediction of Fractional Flow Reserve from Optical Coherence Tomography. Applied Sciences, 12(14), 6964. https://doi.org/10.3390/app12146964