
The Impact of Mechanical Debridement Techniques on Titanium Implant Surfaces: A Comparison of Sandblasted, Acid-Etched, and Femtosecond Laser-Treated Surfaces

 ,
,  , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
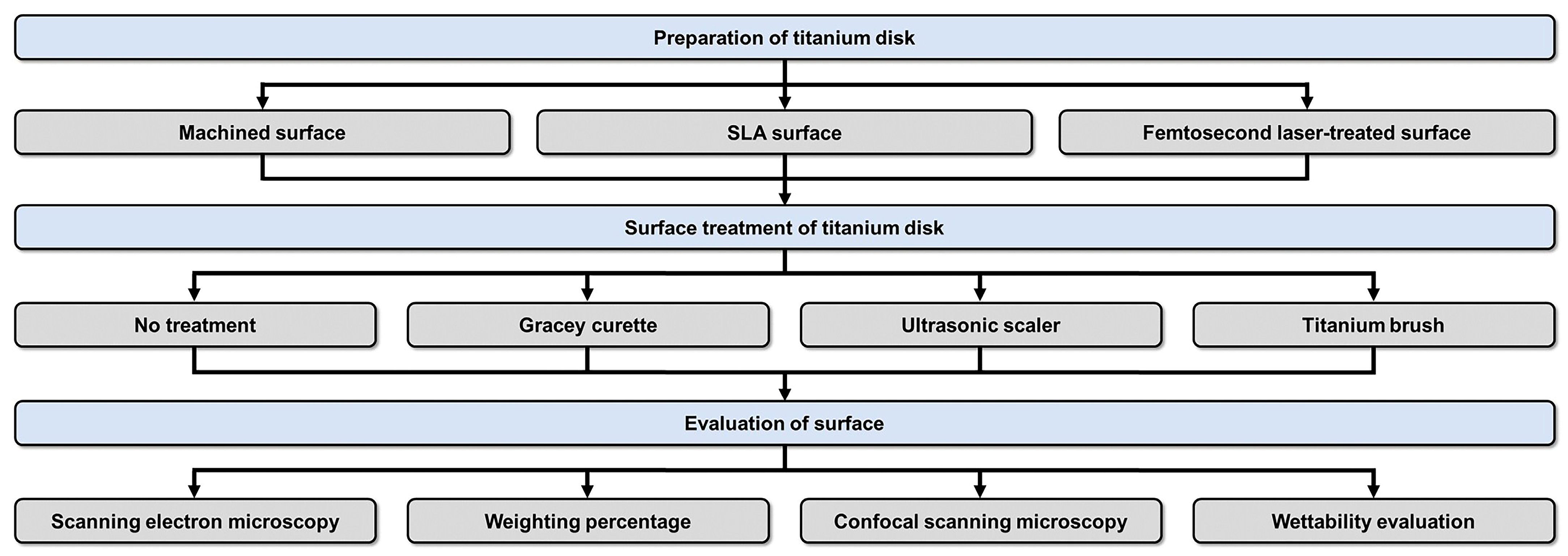
2. Materials and Methods
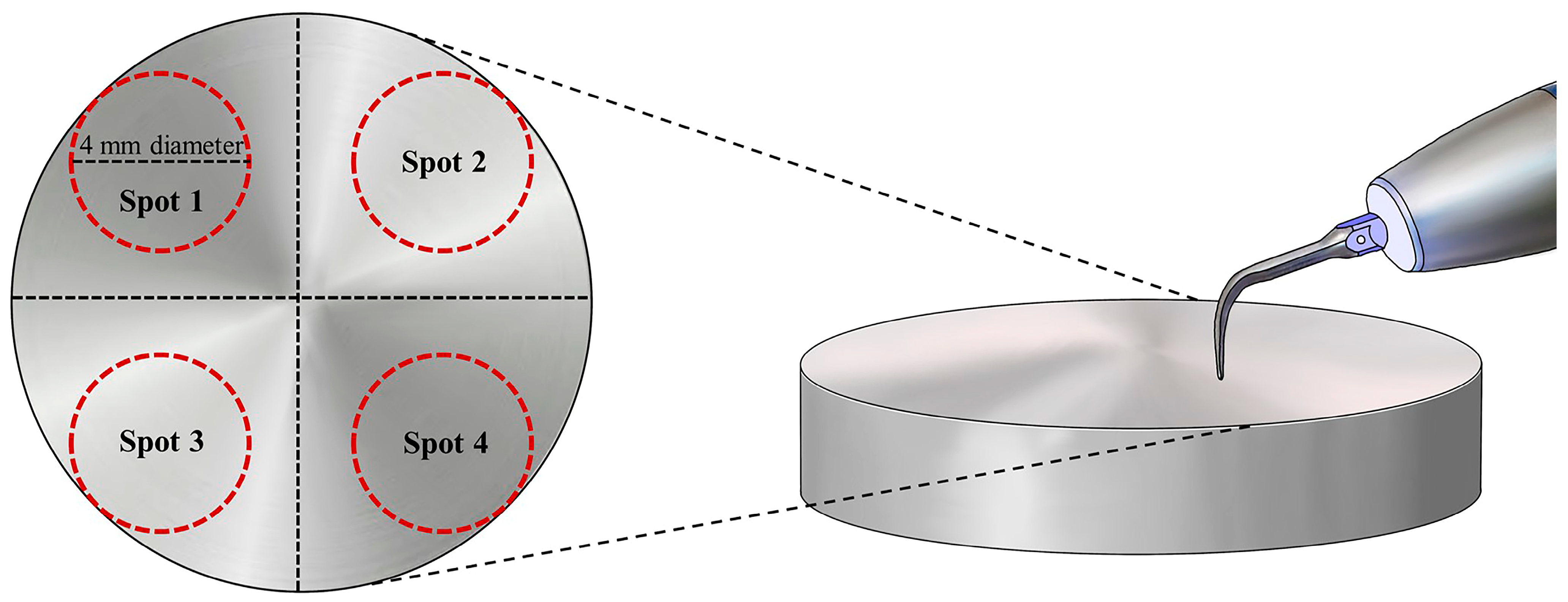
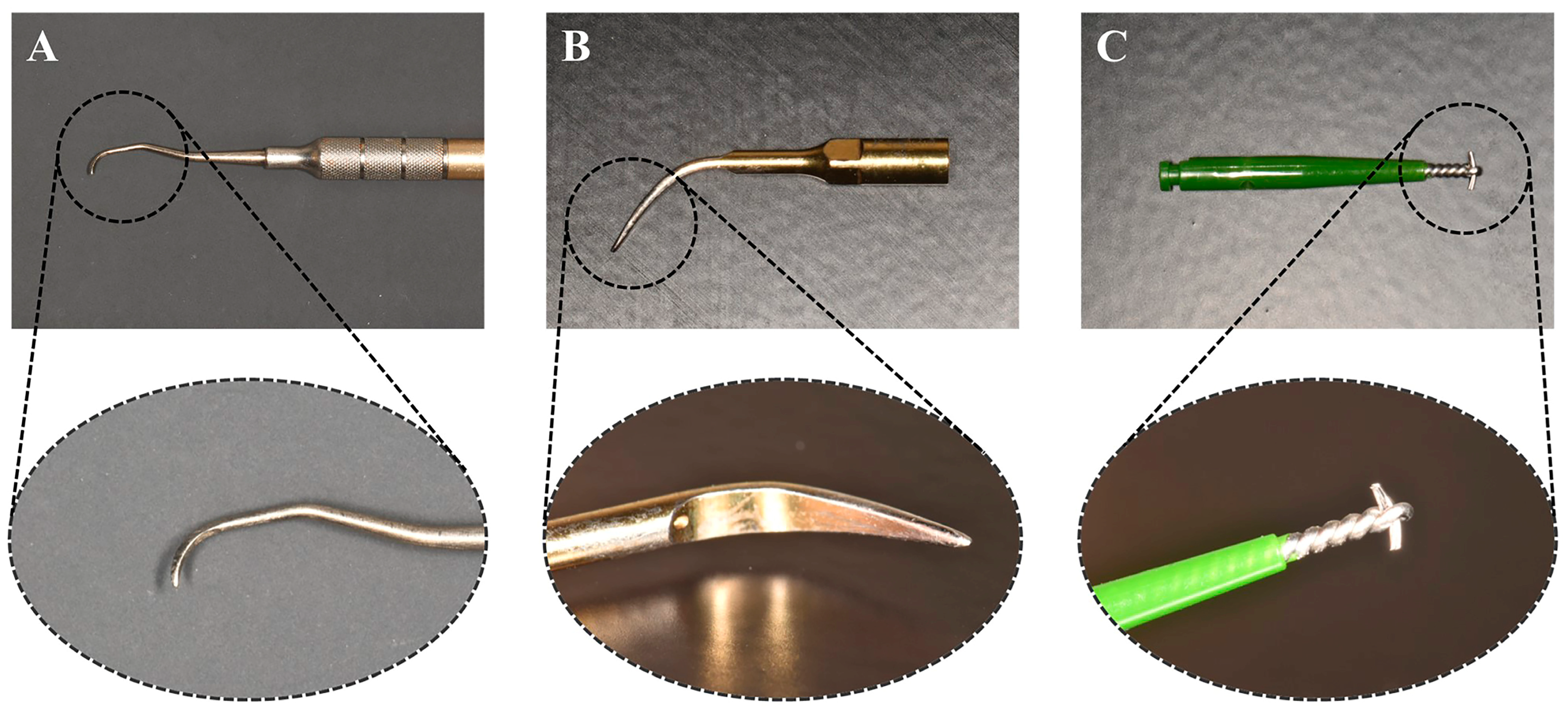
2.1. Surface Treatment of Ti Disks
2.2. SEM, Weight Percentage, and Confocal Scanning Microscopy
2.3. Wettability Evaluation
2.4. Statistical Analysis
3. Results
3.1. SEM Analysis
3.2. Elemental Weight Percentages
3.3. Confocal Laser Scanning Microscopy
3.4. Surface Roughness
3.5. Contact Angle
4. Discussion
4.1. SEM Analysis
4.2. Weight Percentage of Carbon, Oxygen, Ti, and Aluminum Atoms
4.3. Confocal Laser Scanning Microscopy and Surface Roughness
4.4. Contact Angle
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Mendoncxa, G.; Mendoncxa, D.B.; Aragão, F.J.; Cooper, L.F. Advancing dental implant surface technology; From micron- to nanotopography. Biomaterials 2008, 29, 3822–3835. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, L.T.; Leeuwenburgh, S.C.; Wolke, J.G.; Jansen, J.A. Organic-inorganic surface modifications for titanium implant surfaces. Pharm. Res. 2008, 25, 2357–2369. [Google Scholar] [CrossRef] [PubMed]
- Wall, I.; Donos, N.; Carlqvist, K.; Jones, F.; Brett, P. Modified titanium surfaces promote accelerated osteogenic differentiation of mesenchymal stromal cells in vitro. Bone 2009, 45, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Polyzois, I.; Maguire, R. Re-osseointegration on previously contaminated surfaces: A systematic review. Clin. Oral Implant. Res. 2009, 20, 216–227. [Google Scholar] [CrossRef]
- Subramani, K.; Jung, R.E.; Molenberg, A.; Hammerle, C.H. Biofilm on dental implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2009, 24, 616–626. [Google Scholar]
- Barbour, M.E.; O’Sullivan, D.J.; Jenkinson, H.F.; Jagger, D.C. The effects of polishing methods on surface morphology, roughness and bacterial colonisation of titanium abutments. J. Mater. Sci. Mater. Med. 2007, 18, 1439–1447. [Google Scholar] [CrossRef]
- Augthun, M.; Tinschert, J.; Huber, A. In vitro studies on the effect of cleaning methods on different implant surfaces. J. Periodontol. 1998, 6, 857–864. [Google Scholar] [CrossRef]
- Lindhe, J.; Nyman, S. The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health. A longitudinal study of periodontal therapy in case of advanced disease. J. Clin. Periodontol. 1975, 2, 67–79. [Google Scholar] [CrossRef]
- Listgarten, M.A. The role of dental plaque in gingivitis and Periodontitis. J. Clin. Periodontol. 1988, 15, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Newman, H.N. Update on plaque and periodontal disease. J. Clin. Periodontol. 1980, 7, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Lacefield, W.R. Materials characteristics of uncoated/ceramic-coated implant materials. Adv. Dent. Res. 1999, 13, 21–26. [Google Scholar] [CrossRef]
- Özcan, M.; Hämmerle, C. Titanium as a reconstruction and implant material in dentistry: Advantages and pitfalls. Materials 2012, 5, 1528–1545. [Google Scholar] [CrossRef]
- Rosales-Leal, J.I.; Rodríguez-Valverde, M.A.; Mazzaglia, G. Effect of roughness, wettability and morphology of engineered titanium surfaces on osteoblast-like cell adhesion. Colloids Surf. A Physicochem. Eng. Asp. 2010, 365, 222–229. [Google Scholar] [CrossRef]
- Nakae, H.; Yoshida, M.; Yokota, M. Effects of roughness pitch of surfaces on their wettability. J. Mater. Sci. 2005, 40, 2287–2293. [Google Scholar] [CrossRef]
- Ponsonnet, L.; Reybier, K.; Jaffrezic, N. Relationship between surface properties (roughness, wettability) of titanium and titanium alloys and cell behaviour. Mater. Sci. Eng. C 2003, 23, 551–560. [Google Scholar] [CrossRef]
- Sollazzo, V.; Pezzetti, F.; Scarano, A. Zirconium oxide coating improves implant osseointegration in vivo. Dent. Mater. 2008, 24, 357–361. [Google Scholar] [CrossRef]
- Goyal, N.; Priyanka, R.K. Effect of various implant surface treatments on osseointegration—A literature review. Indian J. Dent. Sci. 2012, 4, 154–157. [Google Scholar]
- Novaes, A.B., Jr.; de Souza, S.L.S.; de Barros, R.R.M.; Pereira, K.K.Y.; Iezzi, G.; Piattelli, A. Influence of implant surfaces on osseointegration. Braz. Dent. J. 2010, 21, 471–481. [Google Scholar] [CrossRef]
- Bernardi, S.; Bianchi, S.; Tomei, A.R.; Continenza, M.A.; Macchiarelli, G. Microbiological and SEM-EDS Evaluation of Titanium Surfaces Exposed to Periodontal Gel: In Vitro Study. Materials 2019, 12, 1448. [Google Scholar] [CrossRef] [PubMed]
- Knabe, C.; Klar, F.; Fitzner, R.; Radlanski, R.J.; Gross, U. In vitro investigation of titanium and hydroxyapatite dental implant surfaces using a rat bone marrow stromal cell culture system. Biomaterials 2002, 23, 3235–3245. [Google Scholar] [CrossRef] [PubMed]
- Fouda, M.F.A.; Nemat, A.; Gawish, A.; Baiuomy, A.R. Does the coating of titanium implants by hydroxyapatite affect the elaboration of free radicals. An experimental study. Aust. J. Basic Appl. Sci. 2009, 3, 1122–1129. [Google Scholar]
- Depprich, R.; Ommerborn, M.; Zipprich, H. Behavior of osteoblastic cells cultured on titanium and structured zirconia surfaces. Head Face Med. 2008, 4, 29. [Google Scholar] [CrossRef]
- London, R.M.; Roberts, F.A.; Baker, D.A.; Rohrer, M.D.; O’Neal, R.B. Histologic comparison of a thermal dual-etched implant surface to machined, TPS, and HA surfaces: Bone contact in vivo in rabbits. Int. J. Oral Maxillofac. Implant. 2002, 17, 369–376. [Google Scholar]
- Bonfante, E.A.; Marin, C.; Granato, R. Histologic and biomechanical evaluation of alumina-blasted/acid-etched and resorbable blasting media surfaces. J. Oral Implantol. 2012, 38, 549–556. [Google Scholar] [CrossRef]
- Parsikia, F.; Amini, P.; Asgari, S. Influence of mechanical and chemical surface treatments on the formation of bone-like structure in cpTi for endosseous dental implants. Appl. Surf. Sci. 2012, 259, 283–287. [Google Scholar] [CrossRef]
- He, J.; Zhou, W.; Zhou, X. The anatase phase of nanotopography titania plays an important role on osteoblast cell morphology and proliferation. J. Mater. Sci. Mater. Med. 2008, 19, 3465–3472. [Google Scholar] [CrossRef]
- Hung, K.-Y.; Lo, S.-C.; Shih, C.-S.; Yang, Y.-C.; Feng, H.-P.; Lin, Y.-C. Titanium surface modified by hydroxyapatite coating for dental implants. Surf. Coat. Technol. 2013, 231, 337–345. [Google Scholar] [CrossRef]
- Bihn, S.K.; Son, K.; Son, Y.T.; Dahal, R.H.; Kim, S.; Kim, J.; Lee, K.B. In Vitro Biofilm Formation on Zirconia Implant Surfaces Treated with Femtosecond and Nanosecond Lasers. J. Funct. Biomater. 2023, 14, 486. [Google Scholar] [CrossRef]
- Cho, S.-A.; Jung, S.-K. A removal torque of the laser-treated titanium implants in rabbit tibia. Biomaterials 2003, 24, 4859–4863. [Google Scholar] [CrossRef]
- Conforto, E.; Aronsson, B.-O.; Salito, A.; Crestou, C.; Caillard, D. Rough surfaces of titanium and titanium alloys for implants and prostheses. Mater. Sci. Eng. C 2004, 24, 611–618. [Google Scholar] [CrossRef]
- Monetta, T.; Bellucci, F. The effect of sand-blasting and hydrofluoric acid etching on Ti CP 2 and Ti CP 4 surface topography. Open J. Regen. Med. 2012, 1, 41–50. [Google Scholar]
- Zinger, O.; Anselme, K.; Denzer, A. Time-dependent morphology and adhesion of osteoblastic cells on titanium model surfaces featuring scale-resolved topography. Biomaterials 2004, 25, 2695–2711. [Google Scholar] [CrossRef] [PubMed]
- Xue, W.; Liu, X.; Zheng, X.; Ding, C. In vivo evaluation of plasma-sprayed titanium coating after alkali modification. Biomaterials 2005, 26, 3029–3037. [Google Scholar] [CrossRef]
- Hallgren, C.; Reimers, H.; Chakarov, D.; Gold, J.; Wennerberg, A. An in vivo study of bone response to implants topographically modified by laser micromachining. Biomaterials 2003, 24, 701–710. [Google Scholar] [CrossRef]
- He, F.M.; Yang, G.L.; Li, Y.N.; Wang, X.X.; Zhao, S.F. Early bone response to sandblasted, dual acid-etched and H2O2/HCl treated titanium implants: An experimental study in the rabbit. Int. J. Oral Maxillofac. Surg. 2009, 38, 677–681. [Google Scholar] [CrossRef]
- Kim, H.; Choi, S.-H.; Ryu, J.-J.; Koh, S.-Y.; Park, J.-H.; Lee, I.-S. The biocompatibility of SLA-treated titanium implants. Biomed. Mater. 2008, 3, 25011. [Google Scholar] [CrossRef]
- Chung, S.H.; Mazur, E. Surgical applications of femtosecond lasers. J. Biophotonics 2009, 2, 557–572. [Google Scholar] [CrossRef]
- Niemz, M.H. Laser-Tissue Interactions: Fundamentals and Applications; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Patil, D.; Aravindan, S.; Kaushal Wasson, M.; Rao, P.V. Fast fabrication of superhydrophobic titanium alloy as antibacterial surface using nanosecond laser texturing. J. Micro Nano-Manuf. 2018, 6, 011002. [Google Scholar] [CrossRef]
- Seo, B.Y.; Son, K.; Son, Y.T.; Dahal, R.H.; Kim, S.; Kim, J.M.; Hwang, J.H.; Kwon, S.M.; Lee, J.M.; Lee, K.B.; et al. Influence of Dental Titanium Implants with Different Surface Treatments Using Femtosecond and Nanosecond Lasers on Biofilm Formation. J. Funct. Biomater. 2023, 14, 297. [Google Scholar] [CrossRef] [PubMed]
- Cochran, D.L. The use of reduced healing times on ITI® implants with a sandblasted and acid-etched (SLA) surface: Early results from clinical trials on ITI® SLA implants. Clin. Oral Implant. Res. 2002, 13, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.K.; Paeng, K.; Jung, U.W.; Choi, S.H.; Sanz, M.; Sanz-Martín, I. The effect of five mechanical instrumentation protocols on implant surface topography and roughness: A scanning electron microscope and confocal laser scanning microscope analysis. Clin. Oral Implant. Res. 2019, 30, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-K.; Park, S.-Y.; Son, K.; Kim, Y.-G.; Yu, W.-J.; Lee, K.-B.; Lee, J.-M. Alterations in Surface Roughness and Chemical Characteristics of Sandblasted and Acid-Etched Titanium Implants after Irradiation with Different Diode Lasers. Appl. Sci. 2020, 10, 4167. [Google Scholar] [CrossRef]
- Hakki, S.S.; Tatar, G.; Dundar, N.; Demiralp, B. The effect of different cleaning methods on the surface and temperature of failed titanium implants: An in vitro study. Lasers Med. Sci. 2017, 32, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Wennerberg, A. On osseointegration in relation to implant surfaces. Clin. Implant. Dent. Relat. Res. 2019, 21, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Sartoretto, S.C.; Alves, A.T.N.N.; Resende, R.F.B.; Calasans-Maia, J.; Granjeiro, J.M.; Calasans-Maia, M.D. Early osseointegration driven by the surface chemistry and wettability of dental implants. J. Appl. Oral Sci. 2015, 23, 279–297. [Google Scholar] [CrossRef] [PubMed]
- Milleret, V.; Lienemann, P.S.; Gasser, A.; Bauer, S.; Ehrbar, M.; Wennerberg, A. Rational design and in vitro characterization of novel dental implant and abutment surfaces for balancing clinical and biological needs. Clin. Implant. Dent. Relat. Res. 2019, 21, e15–e24. [Google Scholar] [CrossRef]
- Vorobyev, A.Y.; Guo, C. Femtosecond laser structuring of titanium implants. Appl. Surf. Sci. 2007, 253, 7272–7280. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Method | Weight Percentage | |||
|---|---|---|---|---|---|
| C | O | Ti | Al | ||
| Machined group | Control | 1.2 | 5.05 | 93.75 | - |
| Titanium curette | 1.06 | 6.26 | 91.93 | 0.74 | |
| Titanium scaler | 0.94 | 9.03 | 90.02 | - | |
| Titanium brush | 1.01 | 5.44 | 93.55 | - | |
| SLA group | Control | 0.55 | 4.83 | 94.61 | - |
| Titanium curette | 1.76 | 7.18 | 87.88 | 3.19 | |
| Titanium scaler | 0.6 | 5.19 | 94.2 | - | |
| Titanium brush | 1.04 | 4.71 | 94.24 | - | |
| Femtosecond laser-treated group | Control | 1.64 | 19.32 | 79.05 | - |
| Titanium curette | 1.21 | 13.07 | 85.52 | 0.2 | |
| Titanium scaler | 1.25 | 11.06 | 87.68 | - | |
| Titanium brush | 1.26 | 18.34 | 80.41 | - | |
| Roughness Type | Surface Treatment | Surface Type | Mean | SD | 95% Confidence Interval | p * | Comparison ** | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Ra | Control | Machined | 3.374 | 1.662 | 1.630 | 5.118 | <0.05 | AB |
| SLA | 2.536 | 0.240 | 2.284 | 2.788 | A | |||
| Femto | 5.610 | 2.765 | 2.708 | 8.511 | B | |||
| Titanium Curette | Machined | 3.124 | 1.893 | 1.137 | 5.111 | A | ||
| SLA | 2.796 | 0.210 | 2.576 | 3.016 | A | |||
| Femto | 5.786 | 2.156 | 3.524 | 8.048 | B | |||
| Titanium Scaler | Machined | 3.911 | 1.721 | 2.105 | 5.717 | A | ||
| SLA | 2.143 | 0.288 | 1.840 | 2.445 | B | |||
| Femto | 5.822 | 0.790 | 4.993 | 6.650 | C | |||
| Titanium Brush | Machined | 4.243 | 1.751 | 2.405 | 6.081 | AB | ||
| SLA | 2.694 | 1.046 | 1.596 | 3.791 | A | |||
| Femto | 6.103 | 0.735 | 5.332 | 6.874 | B | |||
| Rough-ness Type | Surface Treatment | Surface Type | Mean | SD | 95% Confidence Interval | p * | Comparison ** | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Sa | Control | Machined | 0.204 | 0.109 | 0.090 | 0.318 | <0.001 | A |
| SLA | 1.698 | 1.127 | 0.516 | 2.881 | A | |||
| Femto | 5.380 | 2.570 | 2.683 | 8.077 | B | |||
| Titanium Curette | Machined | 0.255 | 0.142 | 0.106 | 0.404 | A | ||
| SLA | 1.876 | 1.246 | 0.568 | 3.184 | A | |||
| Femto | 5.553 | 2.153 | 3.293 | 7.813 | B | |||
| Titanium Scaler | Machined | 0.363 | 0.205 | 0.148 | 0.577 | A | ||
| SLA | 1.234 | 0.856 | 0.336 | 2.132 | A | |||
| Femto | 6.083 | 0.538 | 5.518 | 6.648 | B | |||
| Titanium Brush | Machined | 0.378 | 0.199 | 0.170 | 0.586 | A | ||
| SLA | 2.151 | 1.167 | 0.927 | 3.375 | B | |||
| Femto | 6.214 | 0.575 | 5.611 | 6.817 | C | |||
| Surface Type | Treatment Type | Mean | SD | 95% Confidential Interval | p * | Comparison ** | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Machined | Control | 72.837 | 5.302 | 69.901 | 75.773 | 0.012 | A |
| Curette | 73.294 | 2.563 | 71.875 | 74.713 | A | ||
| Scaler | 73.061 | 5.429 | 70.054 | 76.067 | A | ||
| Brush | 67.712 | 6.679 | 64.013 | 71.411 | B | ||
| SLA | Control | 99.883 | 12.482 | 92.971 | 106.795 | <0.001 | A |
| Curette | 80.739 | 11.713 | 74.252 | 87.225 | B | ||
| Scaler | 75.317 | 14.249 | 67.427 | 83.208 | B | ||
| Brush | 73.865 | 9.564 | 68.568 | 79.161 | B | ||
| Femtosecond laser | Control | 94.073 | 5.926 | 90.792 | 97.355 | <0.001 | A |
| Curette | 96.100 | 7.931 | 91.708 | 100.492 | A | ||
| Scaler | 86.287 | 3.826 | 84.169 | 88.406 | B | ||
| Brush | 85.253 | 5.593 | 82.156 | 88.350 | B | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eun, S.-M.; Son, K.; Hwang, S.-M.; Son, Y.-T.; Kim, Y.-G.; Suh, J.-Y.; Hwang, J.H.; Kwon, S.-M.; Lee, J.H.; Kim, H.D.; et al. The Impact of Mechanical Debridement Techniques on Titanium Implant Surfaces: A Comparison of Sandblasted, Acid-Etched, and Femtosecond Laser-Treated Surfaces. J. Funct. Biomater. 2023, 14, 502. https://doi.org/10.3390/jfb14100502
Eun S-M, Son K, Hwang S-M, Son Y-T, Kim Y-G, Suh J-Y, Hwang JH, Kwon S-M, Lee JH, Kim HD, et al. The Impact of Mechanical Debridement Techniques on Titanium Implant Surfaces: A Comparison of Sandblasted, Acid-Etched, and Femtosecond Laser-Treated Surfaces. Journal of Functional Biomaterials. 2023; 14(10):502. https://doi.org/10.3390/jfb14100502
Chicago/Turabian StyleEun, Seung-Mo, Keunbada Son, Sung-Min Hwang, Young-Tak Son, Yong-Gun Kim, Jo-Young Suh, Jun Ho Hwang, Sung-Min Kwon, Jong Hoon Lee, Hyun Deok Kim, and et al. 2023. "The Impact of Mechanical Debridement Techniques on Titanium Implant Surfaces: A Comparison of Sandblasted, Acid-Etched, and Femtosecond Laser-Treated Surfaces" Journal of Functional Biomaterials 14, no. 10: 502. https://doi.org/10.3390/jfb14100502
APA StyleEun, S.-M., Son, K., Hwang, S.-M., Son, Y.-T., Kim, Y.-G., Suh, J.-Y., Hwang, J. H., Kwon, S.-M., Lee, J. H., Kim, H. D., Lee, K.-B., & Lee, J.-M. (2023). The Impact of Mechanical Debridement Techniques on Titanium Implant Surfaces: A Comparison of Sandblasted, Acid-Etched, and Femtosecond Laser-Treated Surfaces. Journal of Functional Biomaterials, 14(10), 502. https://doi.org/10.3390/jfb14100502