
Estrogen Deficiency Impairs Osseointegration in Hypertensive Rats Even Treated with Alendronate Coated on the Implant Surface

 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Strus Cycle and Ovariectomy Surgery
2.3. Losartan Treatment and Systolic Blood Pressure
2.4. Treatment of Implants with Sodium Alendronate
2.5. Implant Placement
2.6. Fluorochrome Application
2.7. Euthanasia
2.8. Analysis
2.8.1. Biomechanical Test
2.8.2. Computed Microtomography (MicroCT)
2.8.3. Epifluorescence Microscopy
2.9. Statistics
3. Results
3.1. Systolic Blood Pressure
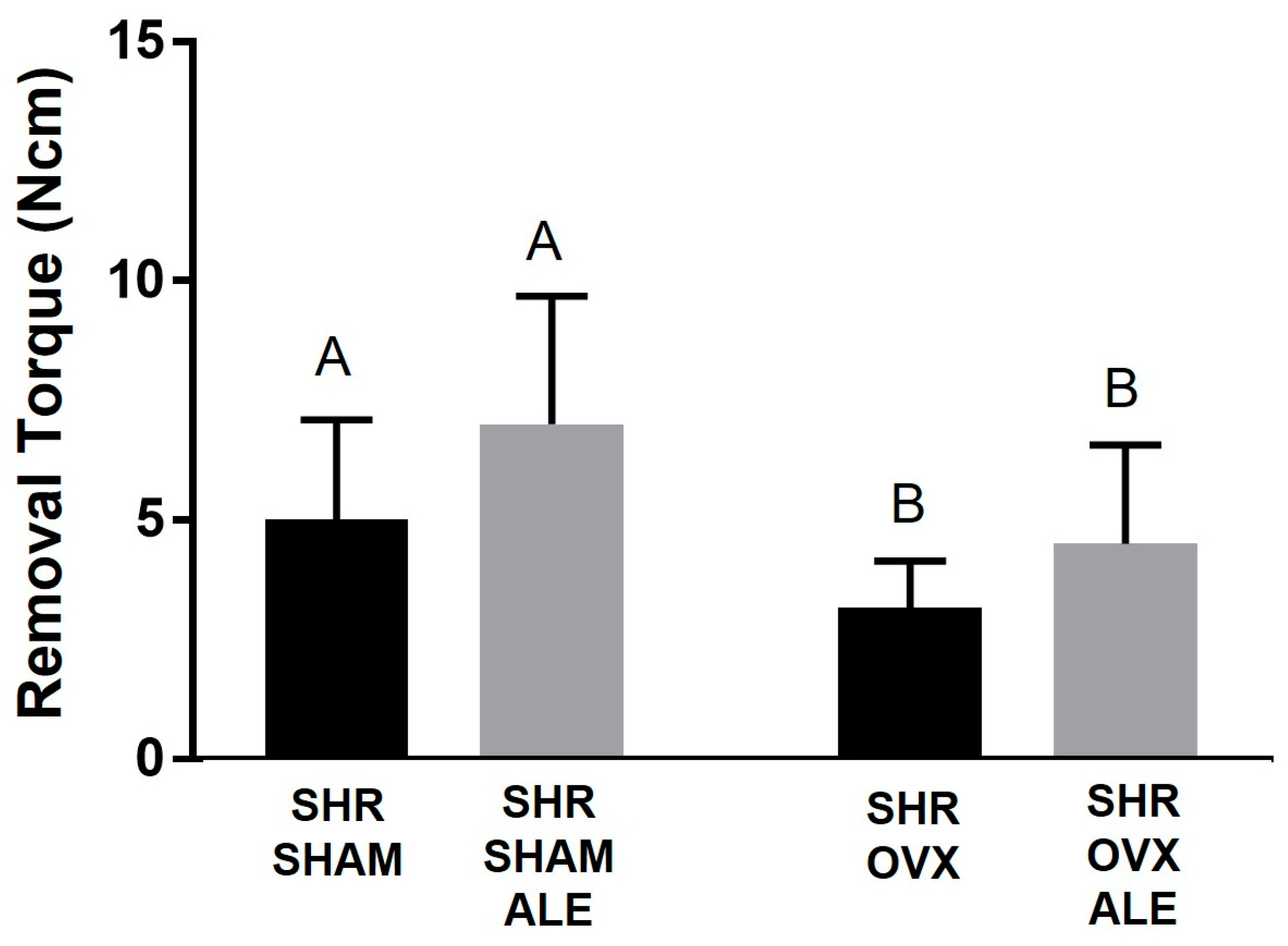
3.2. Removal Torque Values
3.3. Microcomputed Tomography Results
3.4. Epifluorescence Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.; Nicol, C.W.; Gatto, S.N.; Bredin, S.S. Cardiovascular Disease and Osteoporosis: Balancing Risk Management. Vasc. Health Risk Manag. 2007, 3, 673–689. [Google Scholar] [PubMed]
- Varenna, M.; Manara, M.; Galli, L.; Binelli, L.; Zucchi, F.; Sinigaglia, L. The Association between Osteoporosis and Hypertension: The Role of a Low Dairy Intake. Calcif. Tissue Int. 2013, 93, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Barton, M.; Meyer, M.R. Postmenopausal Hypertension: Mechanisms and Therapy. Hypertension 2009, 54, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Chai, H.; Ge, J.; Li, L.; Li, J.; Ye, Y. Hypertension Is Associated with Osteoporosis: A Case-Control Study in Chinese Postmenopausal Women. BMC Musculoskelet. Disord. 2021, 22, 253. [Google Scholar] [CrossRef]
- Khosla, S.; Hofbauer, L.C. Osteoporosis Treatment: Recent Developments and Ongoing Challenges. Lancet Diabetes Endocrinol. 2017, 5, 898–907. [Google Scholar] [CrossRef]
- McCarron, D.A.; Yung, N.N.; Ugoretz, B.A.; Krutzik, S. Disturbances of Calcium Metabolism in the Spontaneously Hypertensive Rat. Hypertension 1981, 3, I162–I167. [Google Scholar] [CrossRef]
- Wright, G.L.; Rankin, G.O. Concentrations of Ionic and Total Calcium in Plasma of Four Models of Hypertension. Am. J. Physiol. 1982, 243, H365–H370. [Google Scholar] [CrossRef]
- Musini, V.M.; Gueyffier, F.; Puil, L.; Salzwedel, D.M.; Wright, J.M. Pharmacotherapy for Hypertension in Adults Aged 18 to 59 Years. Cochrane Database Syst. Rev. 2017, 8, CD008276. [Google Scholar] [CrossRef]
- Santos, C.F.; Morandini, A.C.; Dionisio, T.J.; Faria, F.A.; Lima, M.C.; Figueiredo, C.M.; Colombini-Ishikiriama, B.L.; Sipert, C.R.; Maciel, R.P.; Akashi, A.P.; et al. Functional Local Renin-Angiotensin System in Human and Rat Periodontal Tissue. PLoS ONE 2015, 10, e0134601. [Google Scholar] [CrossRef]
- Donmez, B.O.; Unal, M.; Ozdemir, S.; Ozturk, N.; Oguz, N.; Akkus, O. Effects of losartan treatment on the physicochemical properties of diabetic rat bone. J. Bone Miner. Metab. 2017, 35, 161–170. [Google Scholar] [CrossRef]
- Moura, A.P.; Montalvany-Antonucci, C.C.; Rodrigues de Albuquerque Taddei, S.; Queiroz-Junior, C.M.; Biguetti, C.C.; Garlet, G.P.; Ferreira, A.J.; Teixeira, M.M.; Silva, T.A.; Andrade, I., Jr. Effects of Angiotensin II Type I Receptor Blocker Losartan on Orthodontic Tooth Movement. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Nakagami, H.; Osako, M.K.; Hanayama, R.; Kunugiza, Y.; Kizawa, T.; Tomita, T.; Yoshikawa, H.; Ogihara, T.; Morishita, R. Angiotensin II Accelerates Osteoporosis by Activating Osteoclasts. FASEB J. 2008, 22, 2465–2475. [Google Scholar] [CrossRef] [PubMed]
- Nakai, K.; Kawato, T.; Morita, T.; Yamazaki, Y.; Tanaka, H.; Tonogi, M.; Oki, H.; Maeno, M. Angiotensin II suppresses osteoblastic differentiation and mineralized nodule formation via AT1 receptor in ROS17/2.8 cells. Arch. Med. Sci. AMS 2015, 11, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Al-Majed, A.R.; Assiri, E.; Khalil, N.Y.; Abdel-Aziz, H.A. Losartan: Comprehensive Profile. Profiles Drug Subst. Excip. Relat. Methodol. 2015, 40, 159–194. [Google Scholar] [CrossRef]
- Bastos, M.F.; Brilhante, F.V.; Goncalves, T.E.; Pires, A.G.; Napimoga, M.H.; Marques, M.R.; Duarte, P.M. Hypertension May Affect Tooth-Supporting Alveolar Bone Quality: A Study in Rats. J. Periodontol. 2010, 81, 1075–1083. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Blom, A.W.; Whitehouse, M.R.; Kehoe, P.G.; Laukkanen, J.A. Renin-Angiotensin System Inhibitors and Risk of Fractures: A Prospective Cohort Study and Meta-Analysis of Published Observational Cohort Studies. Eur. J. Epidemiol. 2017, 32, 947–959. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, D.S.; Faitelson, A.V.; Gudyrev, O.S.; Dubrovin, G.M.; Pokrovski, M.V.; Ivanov, A.V. Comparative Evaluation of Enalapril and Losartan in Pharmacological Correction of Experimental Osteoporosis and Fractures of Its Background. J. Osteoporos. 2013, 2013, 325693. [Google Scholar] [CrossRef]
- Wiens, M.; Etminan, M.; Gill, S.S.; Takkouche, B. Effects of Antihypertensive Drug Treatments on Fracture Outcomes: A Meta-Analysis of Observational Studies. J. Intern. Med. 2006, 260, 350–362. [Google Scholar] [CrossRef]
- Lee, J.; Adachi, K.; Gionhaku, N.; Fujita, S.; Uchida, T.; Gerstner, G.E.; Koshikawa, N. Evidence That Angiotensin II Enhances Apomorphine-Induced Jaw Movements via AT1 Receptors in the Ventrolateral Striatum: Studies by Magnet-Sensing System in Freely Moving Rats. Methods Find. Exp. Clin. Pharmacol. 2004, 26, 195–199. [Google Scholar] [CrossRef]
- Garcia-Denche, J.T.; Wu, X.; Martinez, P.P.; Eimar, H.; Ikbal, D.J.; Hernandez, G.; Lopez-Cabarcos, E.; Fernandez-Tresguerres, I.; Tamimi, F. Membranes over the Lateral Window in Sinus Augmentation Procedures: A Two-Arm and Split-Mouth Randomized Clinical Trials. J. Clin. Periodontol. 2013, 40, 1043–1051. [Google Scholar] [CrossRef]
- Jeal, W.; Barradell, L.B.; McTavish, D. Alendronate. A Review of Its Pharmacological Properties and Therapeutic Efficacy in Postmenopausal Osteoporosis. Drugs 1997, 53, 415–434. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Yamamoto, T.; Oda, E.; Nakamura, M.; Fujiwara, S. Real-World Evidence of Raloxifene versus Alendronate in Preventing Non-Vertebral Fractures in Japanese Women with Osteoporosis: Retrospective Analysis of a Hospital Claims Database. J. Bone Miner. Metab. 2016, 36, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, Y.B.; Li, Z.; Shim, J.S.; Moon, H.S.; Jung, H.S.; Chung, M.K. Effect of Alendronate on Healing of Extraction Sockets and Healing around Implants. Oral Dis. 2011, 17, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Kellesarian, S.V.; Abduljabbar, T.; Vohra, F.; Malignaggi, V.R.; Malmstrom, H.; Romanos, G.E.; Javed, F. Role of Local Alendronate Delivery on the Osseointegration of Implants: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 912–921. [Google Scholar] [CrossRef]
- Kennel, K.A.; Drake, M.T. Adverse Effects of Bisphosphonates: Implications for Osteoporosis Management. Mayo Clin. Proc. 2009, 84, 632–638. [Google Scholar] [CrossRef]
- He, L.; Sun, X.; Liu, Z.; Qiu, Y.; Niu, Y. Pathogenesis and Multidisciplinary Management of Medication-Related Osteonecrosis of the Jaw. Int. J. Oral Sci. 2020, 12, 30. [Google Scholar] [CrossRef]
- Jakobsen, T.; Kold, S.; Bechtold, J.E.; Elmengaard, B.; Søballe, K. Effect of Topical Alendronate Treatment on Fixation of Implants Inserted with Bone Compaction. Clin. Orthop. Relat. Res. 2006, 444, 229–234. [Google Scholar] [CrossRef]
- Vohra, F.; Al-Rifaiy, M.Q.; Almas, K.; Javed, F. Efficacy of Systemic Bisphosphonate Delivery on Osseointegration of Implants under Osteoporotic Conditions: Lessons from Animal Studies. Arch. Oral Biol. 2014, 59, 912–920. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Long, J.A.; Evans, H.M.L. The Oestrous Cycle in the Rat and It’s Associated Phenomena; Memoirs of the University of California, University of California Press: Berkeley, CA, USA, 1922. [Google Scholar]
- Mulinari-Santos, G.; Santos, J.S.D.; Palin, L.P.; da Silva, A.C.E.; Antoniali, C.; Faverani, L.P.; Okamoto, R. Losartan Improves Alveolar Bone Dynamics in Normotensive Rats but Not in Hypertensive Rats. J. Appl. Oral Sci. 2019, 27, e20180574. [Google Scholar] [CrossRef]
- Kitagawa, I.L.; Miyazaki, C.M.; Pitol-Palin, L.; Okamoto, R.; de Vasconcellos, L.M.R.; Constantino, C.J.L.; Lisboa-Filho, P.N. Titanium-Based Alloy Surface Modification with TiO2 and Poly(Sodium 4-Styrenesulfonate) Multilayers for Dental Implants. ACS Appl. Bio Mater. 2021, 4, 3055–3066. [Google Scholar] [CrossRef]
- Ramalho-Ferreira, G.; Faverani, L.P.; Grossi-Oliveira, G.A.; Okamoto, T.; Okamoto, R. Alveolar Bone Dynamics in Osteoporotic Rats Treated with Raloxifene or Alendronate: Confocal Microscopy Analysis. J. Biomed. Opt. 2015, 20, 038003. [Google Scholar] [CrossRef] [PubMed]
- Mulinari-Santos, G.; de Souza Batista, F.R.; Kirchweger, F.; Tangl, S.; Gruber, R.; Okamoto, R. Losartan Reverses Impaired Osseointegration in Spontaneously Hypertensive Rats. Clin. Oral Implant. Res. 2018, 29, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Dempster, D.W.; Compston, J.E.; Drezner, M.K.; Glorieux, F.H.; Kanis, J.A.; Malluche, H.; Meunier, P.J.; Ott, S.M.; Recker, R.R.; Parfitt, A.M. Standardized Nomenclature, Symbols, and Units for Bone Histomorphometry: A 2012 Update of the Report of the ASBMR Histomorphometry Nomenclature Committee. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2013, 28, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Aoki, K. Development of a strain of spontaneously hypertensive rats. Jpn. Circ. J. 1963, 27, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Huo, Y.; Yao, C.; Sun, J.; Zhang, Y. The Effect of the Angiotensin-Converting Enzyme Inhibitor on Bone Health in Castrated Hypertensive Rats Is Mediated via the Kinin-Kallikrein System. J. Renin. Angiotensin Aldosterone Syst. 2022, 2022, 9067167. [Google Scholar] [CrossRef] [PubMed]
- Gruber, R. Molecular and Cellular Basis of Bone Resorption. Wien. Med. Wochenschr. 2015, 165, 48–53. [Google Scholar] [CrossRef]
- Teitelbaum, S.L. Bone Resorption by Osteoclasts. Science 2000, 289, 1504–1508. [Google Scholar] [CrossRef]
- Mantovani, A.; Sozzani, S.; Introna, M. Endothelial Activation by Cytokines. Ann. N. Y. Acad. Sci. 1997, 832, 93–116. [Google Scholar] [CrossRef]
- Ramasamy, S.K.; Kusumbe, A.P.; Schiller, M.; Zeuschner, D.; Bixel, M.G.; Milia, C.; Gamrekelashvili, J.; Limbourg, A.; Medvinsky, A.; Santoro, M.M.; et al. Blood Flow Controls Bone Vascular Function and Osteogenesis. Nat. Commun. 2016, 7, 13601. [Google Scholar] [CrossRef]
- Rizzoni, D.; Pasini, E.; Flati, V.; Rodella, L.F.; Paiardi, S.; Assanelli, D.; De Ciuceis, C.; Porteri, E.; Boari, G.E.; Rezzani, R.; et al. Angiotensin Receptor Blockers Improve Insulin Signaling and Prevent Microvascular Rarefaction in the Skeletal Muscle of Spontaneously Hypertensive Rats. J. Hypertens. 2008, 26, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Donmez, B.O.; Ozdemir, S.; Sarikanat, M.; Yaras, N.; Koc, P.; Demir, N.; Karayalcin, B.; Oguz, N. Effect of Angiotensin II Type 1 Receptor Blocker on Osteoporotic Rat Femurs. Pharmacol. Rep. PR 2012, 64, 878–888. [Google Scholar] [CrossRef] [PubMed]
- Dionísio, T.J.; Souza, G.P.; Colombini-Ishikiriama, B.L.; Garbieri, T.F.; Parisi, V.A.; Oliveira, G.M.; Cano, I.P.; Rodini, C.O.; Oliveira, S.H.P.; Greene, A.S.; et al. AT1 Receptor Antagonism Promotes Bone Loss Attenuation in Experimental Periodontitis, Block Inflammatory Mediators, Upregulate Antioxidant Enzymes and Bone Formation Markers. J. Periodontol. 2019, 91, 533–544. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulinari-Santos, G.; dos Santos, J.S.; Kitagawa, I.L.; de Souza Batista, F.R.; Botacin, P.R.; Antoniali, C.; Lisboa-Filho, P.N.; Okamoto, R. Estrogen Deficiency Impairs Osseointegration in Hypertensive Rats Even Treated with Alendronate Coated on the Implant Surface. J. Funct. Biomater. 2023, 14, 471. https://doi.org/10.3390/jfb14090471
Mulinari-Santos G, dos Santos JS, Kitagawa IL, de Souza Batista FR, Botacin PR, Antoniali C, Lisboa-Filho PN, Okamoto R. Estrogen Deficiency Impairs Osseointegration in Hypertensive Rats Even Treated with Alendronate Coated on the Implant Surface. Journal of Functional Biomaterials. 2023; 14(9):471. https://doi.org/10.3390/jfb14090471
Chicago/Turabian StyleMulinari-Santos, Gabriel, Jaqueline Silva dos Santos, Igor Lebedenco Kitagawa, Fábio Roberto de Souza Batista, Paulo Roberto Botacin, Cristina Antoniali, Paulo Noronha Lisboa-Filho, and Roberta Okamoto. 2023. "Estrogen Deficiency Impairs Osseointegration in Hypertensive Rats Even Treated with Alendronate Coated on the Implant Surface" Journal of Functional Biomaterials 14, no. 9: 471. https://doi.org/10.3390/jfb14090471
APA StyleMulinari-Santos, G., dos Santos, J. S., Kitagawa, I. L., de Souza Batista, F. R., Botacin, P. R., Antoniali, C., Lisboa-Filho, P. N., & Okamoto, R. (2023). Estrogen Deficiency Impairs Osseointegration in Hypertensive Rats Even Treated with Alendronate Coated on the Implant Surface. Journal of Functional Biomaterials, 14(9), 471. https://doi.org/10.3390/jfb14090471